
Open Access, Volume 9
The importance of 99m tc-RBC to detect the bleeding site undiagnosed by other methods: A case report
Silvia Hoirisch-Clapauch1 ; Sergio Augusto Lopes de Souza2 ; Bianca Gutfilen2*
1Hospital Federal dos Servidores do Estado, Ministry of Health, Rio de Janeiro, Brazil.
2Universidade Federal do Rio de Janeiro, Medical Radiology Department, Rio de Janeiro, Brazil.
Bianca Gutfilen
Hospital Universitário Clementino Fraga Filho - Departamento de Radiologia Universidade Federal do Rio
de Janeiro (UFRJ), Rua Prof. Rodolpho Paulo Rocco 255, subsolo, Ilha do Fundão, CEP: 21941-913, Rio de
Janeiro - RJ-Brazil.
Tel: 55-21-3938-6274;
Email: bianca.gutfilen@gmail.com
Received : July 04, 2023,
Accepted : Aug 16, 2023
Published : Aug 23, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Ileal and jejunal lesions, accounting for approximately 5% of gastrointestinal bleeding, are seldom visualized with barium and endoscopy studies. We present a case of iron deficiency anemia without overt bleeding, unresponsive to iron therapy. Upper endoscopy, colonoscopy, and mesenteric angiogram were normal, and the patient was misdiagnosed as having myelodysplasia. A bleeding lesion was identified in the jejunum with 99mTc-red blood cell scintigraphy. This paper shows the importance of 99mTc-RBC scintigraphy, especially in cases where other diagnostic methods cannot detect bleeding.
Keywords: Anemia; Endoscopy; Blood cell.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Gutfilen B (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Hoirisch-Clapauch S, Lopes de Souza SA, Gutfilen B. The importance of 99mtc-RBC to detect the bleeding site undiagnosed by other methods: A case report. Open J Clin Med Case Rep. 2023; 2096.
Introduction
The mortality related to gastrointestinal bleeding ranges from 10–30%, so timely diagnosis and treatment are critical [1]. Approximately 5% of gastrointestinal bleeding lesions are between the proximal jejunum and terminal ileum [2]. These lesions are seldom seen in radiologic or endoscopic studies due to the length and peristalsis of the small intestine and overlapping loops [2].
We present a case of iron-deficiency anemia unresponsive to iron therapy without overt bleeding. Upper endoscopy, colonoscopy, and mesenteric angiogram were normal, and 99mTc-red blood cell (99mTcRBC) scintigraphy identified the bleeding lesion. This paper highlights the importance of 99mTc-RBC scintigraphy in detecting gastrointestinal bleeding sites
Case Presentation
A 41-year-old Caucasian man sought primary care, complaining of fatigue. His hemoglobin was 10.1 g/dl, the Mean Corpuscular Volume (MCV) was 64 µ3 , and ferritin was 9 μg/l, consistent with iron deficiency anemia. Tumor markers were negative, and a fecal occult blood test was positive, but upper endoscopy and colonoscopy failed to identify the source of bleeding. He was empirically treated with anthelmintics and was given oral iron, showing a gradual increase in hemoglobin levels.
After eight months, the patient returned with intense fatigue. At that time, the hemoglobin was 7.4 g/dl, and ferritin was 9 μg/l. He was prescribed intravenous iron, and again, there was a gradual increase in hemoglobin levels. Ten months later, the hemoglobin was 4.9 g/dl, and ferritin was 9 μg/l. He was on intravenous iron and started weekly red blood cell transfusions. As the hemoglobin levels did not increase, he was referred to a tertiary hospital with a presumed diagnosis of myelodysplasia. Upon admission, he complained of extreme fatigue and 11% unintentional weight loss over four months due to nausea. He denied bleeding or diarrhea and referred that his only medication was iron. Physical examination revealed cachexia, severe pallor, and resting tachycardia. The hemoglobin was 2.2 g/dl, and ferritin was 9 μg/dl, still consistent with iron deficiency anemia, not myelodysplasia. He was given intravenous iron, antifibrinolytic therapy with intravenous tranexamic acid, erythropoietin, and red blood cell transfusions. An upper endoscopy, a colonoscopy, and a mesenteric angiogram failed to identify the bleeding site. However, the colonoscopy showed fresh blood in the terminal ileum. No surgeon agreed to operate on the patient in that clinical situation.
99mTc-RBC scintigraphy was performed to evaluate possible bleeding sites. Initial scintigraphy images highly suggest bleeding in the left flank, anterior to the middle third of the kidney. Static images showed labeled erythrocytes in the left iliac fossa after 1 hour and in the mesogastrium and hypogastrium at 2.3 and 3 hours (Figure 1). SPECT analysis corroborated the findings of digestive bleeding in the left flank.
Based on 99mTc-RBC scintigraphy’s findings, the patient received another five packs of red blood cell units five days later, totalizing 59 packed red blood cell units. Surgeons finally decided to intervene based on 99mTc-RBC scintigraphy results, and a laparotomy disclosed a 1.5 × 1 cm ulcerated jejunal mass, 10 cm from the Treitz ligament (Figure 2). Histological examination showed angiodysplasia.
The patient was discharged two weeks after surgery on oral iron therapy. The hemoglobin was 7,2 g/dl on discharge and 13 g/dl two months later
Discussion
This case is unusual for the patient’s age-the average age of small bowel angiodysplasia is 72 years [3] and significant unintentional weight loss, mimicking a neoplastic disease. In addition, in severe anemia, gastric hypoxia may impair digestion, causing nausea and unintentional weight loss.
Considering the difficult increase in hemoglobin levels, the absence of overt bleeding, and normal upper endoscopy and colonoscopy, a strong suspicion was raised that the bleeding lesion was located in the small bowel.
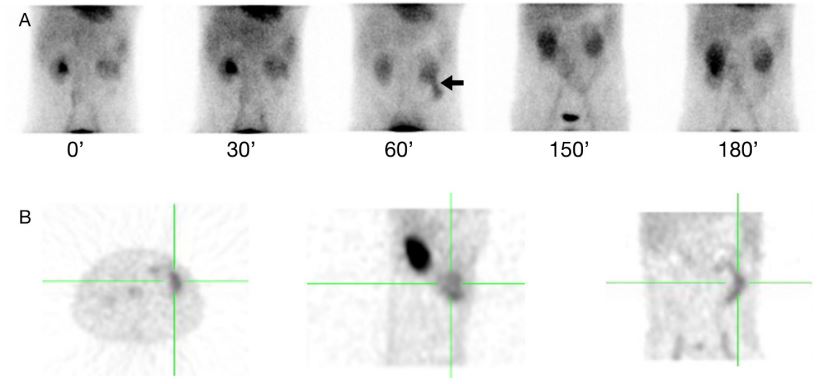
Figure 1: (A): 99mTc-RBC scintigraphy evolution from 0 to 180 minutes after intravenous administration showing the bleeding
site (arrow). (B) SPECT acquisition showing the bleeding site at axial, sagittal, and coronal planes (green triangulation).

Figure 2: A jejunal mass (A) and an ulcerated lesion (B, C).
The bleeding rate was >100 ml/day or >0.07 ml/min based on transfusion requirements. As the surgeons refused to intervene without identifying the bleeding site and capsule endoscopy was unavailable, 99mTc-RBC scintigraphy was essential to localize the lesion. This low-cost, non-invasive method allows observing bleeding for 24 hours without suffering interference from oral or parenteral iron or transfusion.
Conclusion
99mTc-RBC scintigraphy is an essential tool to identify gastrointestinal bleeding undetected by other methods.
Declarations
COI/Disclosure Statement: The authors declare no conflict of interest.
Source of funding: None.
Conflicts of interest: The authors have no conflicts of interest to declare.
References
- Grady E. Gastrointestinal bleeding scintigraphy in the early 21st century. J Nuclear Med 2016; 57: 252-9.
- Raju GS, Gerson L, Das A, Lewis B. American Gastroenterological Association (AGA) Institute technical review on obscure gastrointestinal bleeding. Gastroenterology 2007; 133: 1697-717.
- Holleran G, Hall B, Zgaga L, Breslin N, McNamara D. The natural history of small bowel angiodysplasia. Scand J Gastroenterol 2016; 51: 393-9.
