
Open Access, Volume 11
Late hemothorax due to intercostal pseudoaneurysm rupture: Management by superselective arterial embolization and thoracoscopic debridement: A case report
Sara Degiovanni*; Antonio Tuoro; Sara Vaquer; Federico Raveglia; Andrea Cara; Lidia Libretti; Emanuele Pirondini; Enrico Mario Cassina; Francesco Petrella
Department of Thoracic Surgery, Fondazione IRCCS San Gerardo dei Tintori, 20900 Monza, Italy.
Sara Degiovanni
Department of Thoracic Surgery, Fondazione IRCCS San Gerardo dei Tintori, 20900 Monza, via Curtatone 4, Milan (20122), Italy.
Tel: +39-3493335110;
Email: sara.degiovanni@unimi.it
Received : September 04, 2025,
Accepted : October 06, 2025
Published : October 31, 2025,
Archived : www.jclinmedcasereports.com
Abstract
We report the case of a 26-year-old man who was stabbed causing an intercostal lesion and subsequent formation of a pseudoaneurysm. After an initial admission for bilateral pneumothorax, treated with chest drainage, the patient was discharged haemodynamically stable and with a clear chest X-ray. Seven days later, the patient was re-admitted to the Emergency Department for left thoracodynia and fatigue. A chest CT angiography reported a contrast blush from the fifth left intercostal space and a late-fed hemothorax. Superselective arterial embolization and videothoracoscopic debridement effectively controlled the bleeding and evacuated clots. Postoperative clinical course was uneventful and the patient was discharged on postoperative day three. With this case report we want to emphasize the importance of a multidisciplinary approach to thoracic traumas.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Degiovanni S (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Degiovanni S, Tuoro A, Vaquer S, Raveglia F, Cara A, Libretti L, Pirondini E, et al. Late hemothorax due to intercostal pseudoaneurysm rupture: Management by superselective arterial embolization and thoracoscopic debridement: A case report. Open J Clin Med Case Rep. 2025; 2384.
Introduction
Late hemothorax is a but potentially life-treathing complications of penertrating injuries and pseudoaneurysm of the intercostal arteries is one of the rarest causes for this condition. Pseudoaneurysms may remain asymptomatic for a long time, but their rupture can cause massive bleeding and put the patient’s life at risk. The optimal management of these cases is still debated, but arterial embolization represents an effective and minimally invasive therapeutic option.
Case Presentation
Patient information
A 26-year-old male patient was admitted to the Accident and Emergency Department after being attacked with a knife. He referred acute back pain and shortness of breath; there was no associated fever, coughing or hemoptysis. Remote pathological history is silent.
Clinical findings and timeline
Clinical examination revealed two penetrating wounds in subscapular region bilaterally (approximately 1,5 cm each). A chest X-ray and chest CT were performed; radiological exams demonstrated bilateral pneumothorax and no active pleural effusion. Two chest tubes were immediately placed, one on each side, with active air leakage and sudden improvement of dyspnea. The patient was stabilized; a chest X-ray showed resolution of the bilateral pneumothorax and hemothorax. After 3 days of observation the pleural drainage were removed and the patient finally discharged for follow-up. One week later, the patient returned to the ER complaining of acute chest pain and dyspnea.
Diagnostic assessment
A new chest X-ray showed left hemothorax. Subsequently, a chest CT with contrast was performed, revealing the presence of an intercostal pseudoaneurysm in the fifth intercostal artery, with signs of active bleeding.
Therapeutic intervention
The patient underwent superselective arterial embolization of the involved intercostal artery (Figure 1). The procedure was successfully performed using microcoils (3 and 4 mm), obtaining immediate stop of bleeding (Figure 2). A left chest tube was placed and 1200 mL of blood were evacuated. The patient then underwent videothoracoscopic debridement to evacuate clots and some retained blood.
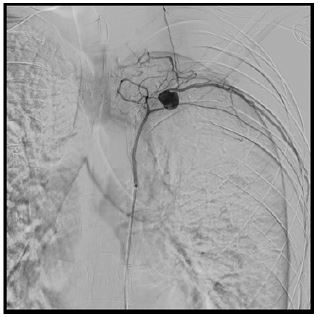
Figure 1: Angiographical embolization of intercostal pseudoaneurysm using microcoils.
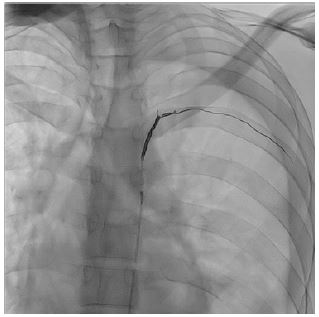
Figure 2: Successful superselective arterial embolization.

Figure 3: Chest X-ray performed one month after surgery.
Follow-up and outcomes
The patient was discharged in good general condition; chest X-ray performed one month after surgery did not disclose any pathologic finding (Figure 3).
Discussion/Conclusion
Intercostal artery pseudoaneurysm is a rare condition, mainly occurring after traumatic injury of the vessel, potentially resulting in blood leaking, chest wall hematoma and haemothorax. It may be due to blunt and penetrating thoracic trauma [2-4], thoracoscopic and laparoscopic procedures [5,6], cardiac surgery procedures and median sternotomy [7], as well as biopsies [8,9] and thoracentesis [10,11]. Patients usually present dyspnea, fatigue and anemia due to the hemothorax; often in need of blood transfusions. Signs and symptoms may also be delayed in case of late hemothorax, which can occur up to 1 month after the vessel injury. Diagnosis is usually obtained by arteriography, although doppler ultrasound is becoming increasingly and successfully adopted [11].
Treatment may vary according to the clinical and radiological findings. Arterial embolization is the most common and accepted therapy [12], but conservative management or cover stent grafting can represent an effective alternative [3]. Aneurysmectomy can be considered in case of unsuccessful embolization [2]. Arterial embolization can be performed with different devices, microcoils being the most common, as in our case, although other devices have been described (eg: glue-lipiodol mixture [13], polyvinyl alcohol particles and gelfoam slurry [8,14]. Ultrasound-guided thrombin injection [7,9] has been described as well as surgical open approach as first choice [2,5,15].
Multidisciplinary approach is paramount for properly treating penetrating thoracic injuries. Intercostal artery pseudoaneurysms in patients with penetrating thoracic injuries should be always taken into consideration in order to diagnose it before rupture. Superselective arterial embolization is an effective and safe technique to treat bleeding intercostal pseudoaneurysms, together with thoracoscopic pleural debridement to allow a complete lung re-expansion.
Ethics statement: Written informed consent for publication of the research details and clinical images was obtained from the patient.
Conflicts of interest: The authors have no conflicts of interest to declare.
References
- Rivera PA, Dattilo JB. Pseudoaneurysm. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
- Aoki T, Okada A, Tsuchida M, Hayashi J. Ruptured intercostal artery pseudoaneurysm after blunt thoracic trauma. Thorac Cardiovasc Surg. 2003;51:346–347.
- Sekino S, Takagi H, Kubota H, Kato T, Matsuno Y, Umemoto T. Intercostal artery pseudoaneurysm due to stab wound. J Vasc Surg. 2005;42:352–356.
- Gutierrez Romero DF, Barrufet M, Lopez-Rueda A, Burrel M. Ruptured intercostal artery pseudoaneurysm in a patient with blunt thoracic trauma: diagnosis and management. BMJ Case Rep. 2014;2014:bcr2013202019.
- Atherton WG, Morgan WE. False aneurysm of an intercostal artery after thoracoscopic sympathectomy. Ann R Coll Surg Engl. 1997;79:229–230.
- Bluebond-Langner R, Pinto PA, Kim FJ, Hsu T, Jarrett TW. Recurrent bleeding from intercostal arterial pseudoaneurysm after retroperitoneal laparoscopic radical nephrectomy. Urology. 2002;60:1111.
- Lenders G, Van Schil P, Rodrigus I, Bosmans J. Intercostal artery pseudoaneurysm: a rare complication of transaortic transcatheter aortic valve implantation. Interact Cardiovasc Thorac Surg. 2012;15:550–552.
- Melloni G, Bandiera A, Crespi G, Zannini P. Intercostal artery pseudoaneurysm after computed tomography-guided percutaneous fine needle aspiration lung biopsy. J Thorac Imaging. 2012;27:W48–W49.
- Vajtai Z, Roy N. Intercostal artery pseudoaneurysm after ultrasound-guided liver biopsy: a case report and review of the literature. Ultrasound Q. 2015;31:63–65.
- Long SS, Johnson PT, Fishman EK. Intercostal artery pseudoaneurysm due to thoracentesis: diagnosis with three-dimensional computed tomographic angiography. J Comput Assist Tomogr. 2012;36:100–102.
- Casper KP, Sanchirico PJ, Pfeiffer DC. Intercostal artery pseudoaneurysm following thoracentesis: multi-modal imaging and treatment. BMC Med Imaging. 2019;19:31.
- Yamakado K, Nakatsuka A, Tanaka N, Takano K, Matsumura K, Takeda K. Transcatheter arterial embolization of ruptured pseudoaneurysms with coils and n-butyl cyanoacrylate. J Vasc Interv Radiol. 2000;11:66–72.
- Chalapathi Rao M, Rathi AA, Reddy SP, Sahu S. Intercostal artery pseudoaneurysm complicating corrosive acid poisoning: diagnosis with CT and treatment with transarterial embolisation. Indian J Radiol Imaging. 2014;24:135–138.
- Sharma M, Singhal M, Kamble R, Bhalla A, Gorsi U, Khandelwal N. Intercostal artery pseudoaneurysm in pulmonary tuberculosis: a rare cause of hemoptysis. Lung India. 2019;36:63–65.
- Wallace RB, Nast EP. Postcoarctation mycotic intercostal arterial pseudoaneurysm. Am J Cardiol. 1987;59:1014–1015.
