
Open Access, Volume 11
Neurogenic thoracic outlet syndrome in an adolescent presenting with intrinsic hand muscle atrophy: Clinical case
Ana Isabel Moreira Ribeiro1*; Mário Ribeiro1; Angela Pereira1; Alexandra dos Santos2; César Silva2
1Pediatric Service, Braga Hospital, Portugal.
2Trofa Hospital, Gaia, Portugal.
Ana Isabel Moreira Ribeiro
Pediatric Service, Braga Hospital, Portugal.
Email: anabarrosribeiro@gmail.com
Received : August 01, 2025,
Accepted : September 24, 2025
Published : September 30, 2025,
Archived : www.jclinmedcasereports.com
Keywords: Neurogenic thoracic outlet syndrome; First rib anomaly.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Ribeiro AIM (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Ribeiro AIM, Ribeiro M, Pereira A, Santos AD, Silva C. Neurogenic thoracic outlet syndrome in an adolescent presenting with intrinsic hand muscle atrophy: Clinical case. Open J Clin Med Case Rep. 2025; 2383.
Description
We report the case of a 15-year-old caucasian male, with no relevant past medical history, who presented to a pediatric neurology consultation with a 10-month history of paresthesias in the lateral side of the right hand. This was accompanied by progressive motor deficit and increasing difficulty in performing Activities of Daily Living (ADLs), particularly writing and playing the drums.
Neurological examination revealed marked atrophy of the thenar eminence and interosseous muscles of the right hand, as well as mild atrophy of the muscles of the right forearm (Figure 1). Electromyography demonstrated signs of injury to the lower trunk of the right brachial plexus and hypoesthesia in the territory of the ulnar nerve. Ultrasound showed diffuse atrophy of the ventral muscles of the right hand, most prominent in the thenar region. A chest X-ray revealed a complete supernumerary cervical rib on the right side.
The patient underwent surgical resection of the anomalous rib via a supraclavicular approach with clavicular osteotomy. He has since been undergoing thrice-weekly physical therapy, which he continues to date, with gradual recovery of right hand strength, progressive reversal of muscle atrophy, and functional improvement in ADLs.
Neurogenic Thoracic Outlet Syndrome (TOS) is a rare but important pediatric condition, often caused by brachial plexus compression due to congenital bony anomalies like cervical ribs. Diagnosis is mainly clinical, supported by electromyography and imaging to confirm nerve involvement and structural defects, but clinical assessment remains key. Early diagnosis is vital to prevent irreversible nerve damage, muscle atrophy, and vascular complications. Treatment usually involves surgical decompression and physical therapy, with multidisciplinary care essential for optimal recovery [1-3].
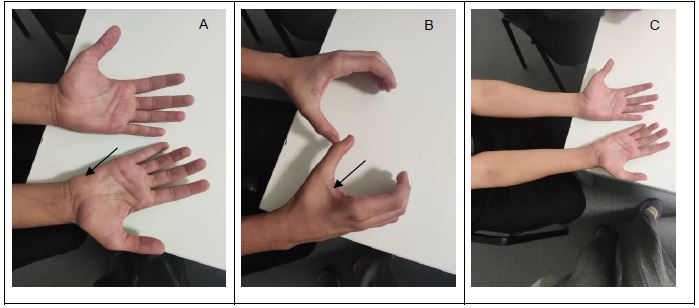
Figure 1: Atrophy of the thenar eminence (A) and interosseous muscles of the right hand (B), along with mild atrophy of the muscles of the right forearm (C).
References
- Rehemutula A, Zhang L, Chen L, Chen D, Gu Y. Managing pediatric thoracic outlet syndrome. Ital J Pediatr. 2015; 41: 22.
- Price A, Fredricks N, Truong N, North RY. Pediatric thoracic outlet syndrome: a systematic review and meta-analysis. J Neurosurg Pediatr. 2024; 33: 484-495.
- Abdalla BA, Kakamad FH, Namiq HS, et al. Pediatric thoracic outlet syndrome: a systematic review with metadata. Pediatr Surg Int. 2024; 40: 186.
