
Open Access, Volume 11
Ischiopagus parasitic twin with omphalocele and bladder exstrophy: Renal failure reversed by excision – A case report
Dania Bouguermouh1*; Karim Meskouri2; Mohamed Redjimi1; Ladjal Yasmina1; Mazigh Timedjeghdine1
1Department of Pediatric Surgery, CHU Mustapha, University of Algiers, Algeria.
2Department of Thoracic and Cardiovascular Surgery, CHU Mustapha, University of Algiers, Algeria.
Dania Bouguermouh
Department of Pediatric Surgery, CHU Mustapha, University of Algiers, Algeria.
Tel: +213772432728;
Email: bouguermouhdania@yahoo.fr
Received : August 13, 2025,
Accepted : September 10, 2025
Published : September 30, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Parasitic twinning, or heteropagus, is a rare congenital malformation characterized by an incompletely formed twin attached to a well-developed autosite. We report an exceptional case of an ischiopagus parasitic twin presenting with acute renal failure at birth. The parasite included a well-formed lower limb, an upper limb segment with scapula, pelvic structures, digestive loops, and five vertebrae with vascularization from both internal iliac arteries. Surgical excision of the parasite was performed after stabilization, resulting in the resolution of renal failure. Despite initial postoperative improvement, the patient developed Disseminated Intravascular Coagulation (DIC) and died on postoperative day 20. This case illustrates the challenges of managing complex parasitic twins and highlights the potential for unpredictable, life-threatening complications even after technically successful surgery.
Keywords: Disseminated intravascular coagulation; Ischiopagus; Neonatal malformations; Parasitic twin; Pediatric surgery; Renal failure.
Abbreviations: DIC: Disseminated Intravascular Coagulation; MRI: Magnetic Resonance Imaging; CT: Computed Tomography.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Bouguermouh D (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Bouguermouh D, Meskouri K, Redjimi M, Yasmina L Timedjeghdine M, Timedjeghdine M. Ischiopagus parasitic twin with omphalocele and bladder exstrophy: Renal failure reversed by excision – A case report. Open J Clin Med Case Rep. 2025; 2379.
Introduction
Parasitic twinning is a rare developmental anomaly; with an incidence estimated at one in 1 – 2 million live births. The condition involves an incomplete twin (parasite) physically attached to a more developed fetus (autosite), most commonly at the epigastrium or pelvis [1]. Ischiopagus parasitic twins are among the rarest forms and often pose significant diagnostic, surgical, and ethical challenges [2]. These malformations can include vascular and visceral sharing, as well as genitourinary or digestive anomalies [3]. Although surgical excision may lead to functional recovery, postoperative outcomes remain unpredictable. We present a rare case of an ischiopagus parasitic twin with acute renal failure that resolved following resection of the parasite, but was complicated by fatal DIC.
Case Presentation
A male newborn was delivered at 38 weeks gestation via cesarean section for prenatal suspicion of a conjoined twin. Birth weight was 3500 g. On examination, the autosite had a normally formed trunk and limbs, but an additional lower limb, upper limb remnant, and segmental torso mass were attached to the right side of the pelvis.
Initial investigations revealed an omphalocele, a left colostomy for neonatal colonic perforation, and exstrophy of the bladder. MRI and CT imaging showed that the parasite contained five vertebrae, two ribs, a complete right lower limb with pelvic bone, a partial upper limb with hemiscapula, and a functional kidney and bladder system. Vascularization was derived from both internal iliac arteries of the autosite. The anteroposterior infantogram and the bony axial scan clearly illustrated the parasitic structures and vertebral segment (Figure 1).
The patient developed acute renal failure in the first days of life, characterized by anuria and elevated creatinine levels. A multidisciplinary decision was made to perform partial excision of the parasitic structures, preserving vital anatomy of the autosite. Surgery included resection of the lower and upper limbs and the majority of the pelvic mass. Postoperative urine output resumed promptly, and renal function normalized within 72 hours.
Preoperative, intraoperative, and specimen images provide a visual summary of the operative sequence (Figure 2). Postoperative appearance confirmed removal of parasitic elements and closure of abdominal wall defect (Figure 3).
Despite favorable immediate outcomes, the patient developed progressive thrombocytopenia, coagulopathy, and signs of multiorgan dysfunction. Despite intensive care support, the child died on postoperative day 20 from disseminated intravascular coagulation.
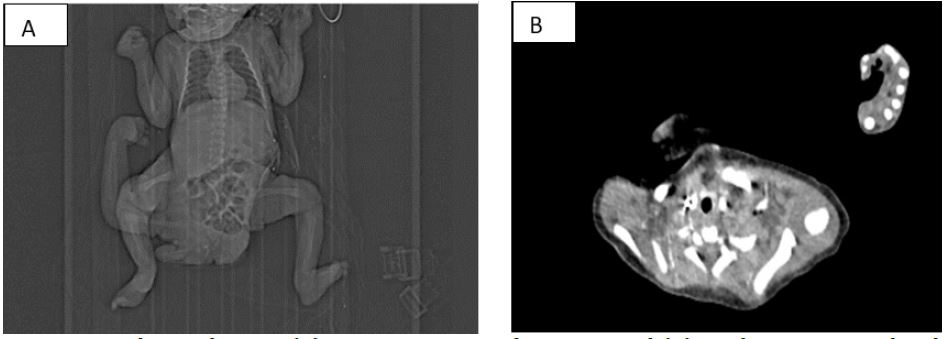
Figure 1: Image scanographique showing (A) anteroposterior infantogram and (B) axial CT scan revealing bony parasitic structures.
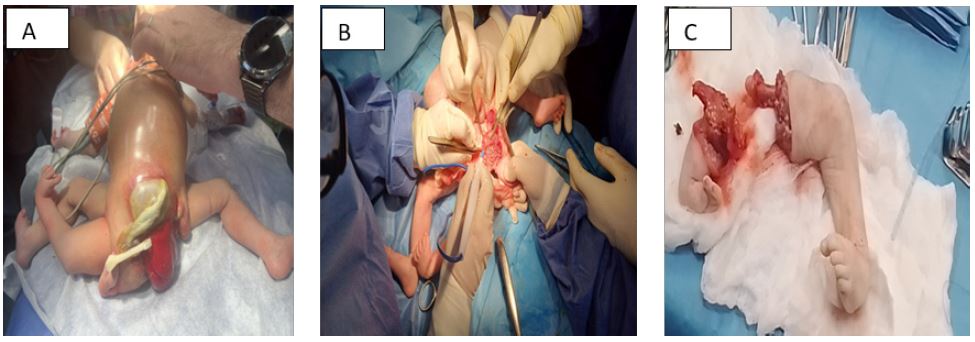
Figure 2: (A) Preoperative photograph showing the parasite, (B) Peroperative view, (C) Surgical specimen after excision.

Figure 3: Postoperative image of the autosite after closure.
Discussion/Conclusion
Parasitic twinning presents a spectrum of anatomical configurations that often require individualized surgical planning. In this case, the mechanical and possibly vascular burden of the parasite may have contributed to early renal compromise, reversed only after excision. The resolution of renal failure post-surgery highlights the potential benefits of timely intervention in such cases [4].
However, the unexpected progression to DIC despite surgical success reminds clinicians of the fragility of neonates with complex malformations. The etiology of DIC in this case is unclear—possibly related to massive tissue resection, endothelial injury, or sepsis. This outcome underscores the necessity for prolonged, multidisciplinary postoperative monitoring in high-risk neonates, even after initial recovery [5].
This case contributes to the limited literature on ischiopagus parasitic twins and serves as a cautionary tale regarding delayed and unpredictable complications. It reinforces the value of individualized care and the importance of parental counseling regarding prognosis and possible outcomes [6].
Declarations
Informed consent statement: Informed consent form was signed by the parents for the use of pictures according to the requirements of ethical Mustapha Hospital University.
Conflict of interest: The authors declare no conflict of interest.
Acknowledgements: We thank the pediatric intensive care and anesthesiology teams at CHU Mustapha for their dedicated management of this complex case.
References
- Spencer R. Parasitic conjoined twins: external, internal (fetuses in fetu and teratomas), and detached. Clin Anat. 2001; 14: 428–444.
- Kaufman MH. The embryology of conjoined twins. Childs Nerv Syst. 2004; 20: 508–525.
- Ebrahim MA, Shorbagy MM, Gawish AM, et al. Ischiopagus parasitic twin: surgical challenge in a neonate. Pediatr Surg Int. 2013 ; 29: 711–714.
- Lozano A, Munoz M, Gonzalez R, et al. Parasitic ischiopagus twin: embryologic, radiologic and surgical features. Fetal Diagn Ther. 2007; 22: 259–263.
- Spitz L, Kiely EM. Experience in the management of conjoined twins. Br J Surg. 2000 ; 87: 307–313.
- Ratan SK, Rattan KN, Magu S, et al. Ischiopagus parasitic twin: a case report and review of literature. J Pediatr Surg. 2005; 40: E9–E11.
