
Open Access, Volume 11
Spontaneous recanalization of the middle cerebral artery after a stroke and decompressive craniectomy, A case report
Eduardo Trejo-Olguín; Maurilio Vicente Ochoa-González; Christian Félix-Montiel; T. Edgar Omar Rodríguez-Guajardo; Jesús Alberto Morales-Gómez*; Ángel Martínez-Ponce de León
Hospital Universitario «José Eleuterio González», Monterrey, Nuevo León, Mexico.
Jesús Alberto Morales-Gómez
Hospital Universitario “José Eleuterio González”, Monterrey, Nuevo León, Mexico.
Email: chfelix0016@gmail.com
Received : June 20, 2025,
Accepted : July 24, 2025
Published : July 31, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Occlusion of the Middle Cerebral Artery (MCA) is the most common form of large vessel ischemic stroke. Mechanical thrombectomy is the gold standard for eligible patients within the therapeutic window, while intravenous thrombolysis remains an option in the absence of endovascular access. If both treatments are unfeasible and infarction progresses to a malignant profile, decompressive craniectomy is used as a salvage measure. In rare cases, spontaneous recanalization of the occluded vessel occurs, and its timing is crucial for favorable outcomes.
Clinical case: A 57-year-old male with type 2 diabetes, hypertension, and a history of smoking presented with left hemiparesis, dysarthria, and somnolence. Computed Tomography (CT) imaging revealed a large right MCA infarct. Due to presentation outside the therapeutic window, conservative management was initiated. Clinical deterioration led to decompressive craniectomy. Postoperatively, neurological improvement was noted. A CT angiogram at 48 hours revealed spontaneous recanalization of the right M1 segment, confirmed by cerebral angiography at two weeks. At three months, the patient showed a significant neurological improvement and partial motor recovery.
Conclusion: Spontaneous MCA recanalization is rare and not fully understood. Potential mechanisms include thrombolysis, hemodynamic changes, and collateral flow. Early recanalization, is associated with better outcomes, as observed in this case. Further research is needed to identify predictors and guide clinical management.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Felix C (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Trejo-Olguín E, Ochoa-González MV, Félix-Montiel C, Rodríguez-Guajardo TEO, Morales-Gómez JA, Martínez-Ponce de León A. Spontaneous recanalization of the middle cerebral artery after a stroke and decompressive craniectomy, A case report. Open J Clin Med Case Rep. 2025; 2372.
Introduction
Ischemic stroke is a leading cause of morbidity and mortality worldwide. Among its different presentations, occlusion of the MCA is the most prevalent, often resulting in profound neurological deficits. Current therapeutic paradigms prioritize prompt revascularization, primarily through mechanical thrombectomy within a defined therapeutic window. In institutions without endovascular capabilities, systemic thrombolysis is considered an alternative, provided the patient presents within the eligible timeframe [5,9].
Nevertheless, when revascularization is not achieved and the patient progresses to malignant infarction, the prognosis becomes poor, and decompressive craniectomy is often the only life-saving intervention. Despite extensive literature on reperfusion strategies, there have been extraordinary spontaneous recanalization cases observed and warrant further investigation [16].
Here, we present a case of a patient with MCA infarction who was not eligible for thrombolysis or thrombectomy, underwent decompressive craniectomy due to neurological deterioration, and was later found to exhibit spontaneous recanalization of the occluded artery.
Case Presentation
A 57-year-old male with a medical history of type 2 diabetes mellitus, systemic arterial hypertension, and a cumulative smoking exposure of 3.7 pack-years presented with a five-day history of dense left faciobrachio-crural hemiparesis, dysarthria, and somnolence. On admission, he scored 16 on the National Institutes of Health Stroke Scale (NIHSS) and 12 on the Glasgow Coma Scale (GCS).
Investigations: Non-contrast CT revealed ischemic changes in the right MCA territory with an Alberta Stroke Program Early CT Score (ASPECTS) score of 6 (Figure 1). The patient was deemed ineligible for pharmacological or mechanical recanalization due to exceeding the therapeutic window.
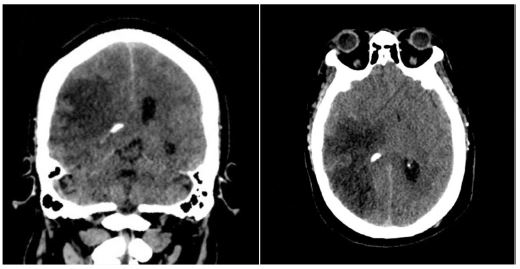
Figure 1: Computed tomography scan upon patient admission. Evidence of ischemic stroke due to right MCA occlusion is observed.
Twenty-four hours post-admission, his neurological status worsened (GCS decreased by 4 points), and a CT scan showed a significant midline shift. A right-sided frontotemporoparietal decompressive craniectomy was performed. Postoperatively, his GCS improved to 14 and motor strength improved to 3/5 on the Lovett scale (Figure 2). A Computed Tomography Angiography (CTA) performed 48 hours after surgery showed restored flow in the M1 and distal branches of the right MCA (Figure 3). A confirmatory cerebral angiogram at two weeks demonstrated patent flow throughout the MCA distribution (Figure 4).
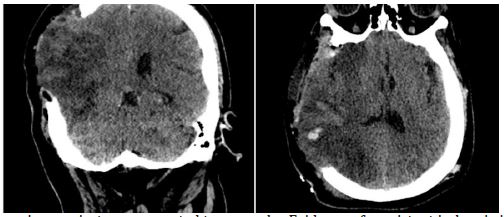
Figure 2: Post-decompressive craniectomy computed tomography. Evidence of persistent ischemia is observed in the right MCA territory.
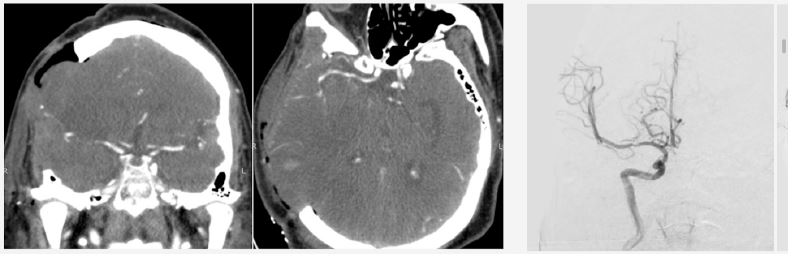
Figure 3: Computed tomography angiography 48 hours after decompressive craniectomy, showing vascular flow in the right MCA territory.
Follow up and prognosis
Upon discharge, the patient had an ECG score of 15, a Karnofsky Performance Score of 70, and residual hemiparesis of 3/5. At a three-month follow-up, he had improved to a Karnofsky score of 90 and 4/5 strength in the left upper limb, with persistent left facial nerve palsy (Figure 5).
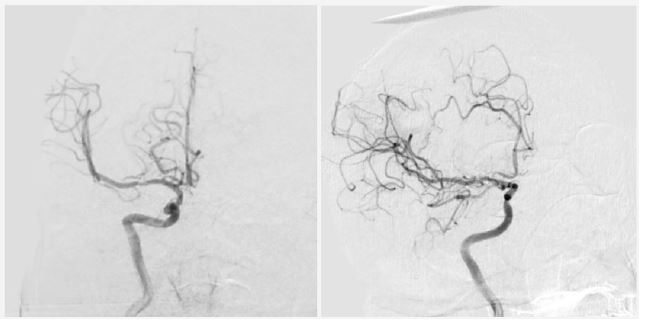
Figure 4: Cerebral angiography 2 weeks later, showing recanalization of the right MCA.

Figure 5: Images authorized by the patient and family. 3-month follow-up. Patient with Barre grade ⅘ hemiparesis in the left upper extremity, central paresis of the left seventh cranial nerve, and recovery of strength in the left lower extremity.
Discussion
Spontaneous recanalization of intracranial arteries such as the ICA and MCA has been reported, though its true incidence and mechanisms remain unclear. While once considered rare, more recent studies suggest it may be more common. Fieschi and Bozzao (1969) documented early findings of ICA recanalization [2]. Recanalization occurred in 40% of a 30-patient ICA occlusion cohort [1], with other studies reporting rates of 2.3-10.3% [15]. A meta-analysis on MCA occlusion revealed 21.4% recanalization within 24 hours and 52.7% within a week, though variations in imaging may explain discrepancies [3].
Timing of recanalization is highly variable—from hours to years—and earlier recanalization, like in this case, is associated with better outcomes [12]. Mechanisms include thrombus dissolution, undetected residual lumen, or collateral flow, though these do not always lead to clinical improvement [8].
Diagnostic imaging includes CTA (sensitivity 100%, specificity 98%), Doppler ultrasound (less reliable for intracranial vessels), and Digital Subtraction Angiography (DSA), the gold standard despite a 5% complication rate [14].
Management guidelines for spontaneous recanalization are lacking. Treatments include antiplatelets, anticoagulants, and statins, though their effectiveness in inducing recanalization is uncertain. Due to favorable outcomes, individualized treatment and monitoring are recommended [10].
Reported frequencies of MCA recanalization vary by modality (5–20%). Mechanisms proposed include vasospasm resolution, embolization, and intrinsic thrombolysis. Some patients may have had slow flow misinterpreted as occlusion [11,16]. Persistent M1 patency despite distal branch occlusion argues against artifactual diagnoses. Predictive factors include thrombus size, fibrin content, and collateral flow. Imaging advancements aid detection.
Prior studies confirm similar findings and support endogenous thrombolysis as a contributing factor [4,6,7,12,17]. Recanalization is more common in cardioembolic stroke or arterial dissection; antiplatelet/anticoagulant use in dissection may support thrombus resolution [8]. A meta-analysis reaffirmed early MCA recanalization rates and their correlation with improved outcomes [13].
In atherosclerotic occlusion, mechanisms remain uncertain. Yi et al. linked atrial fibrillation to lower recanalization and hypertension to higher rates. Buslovich and Hines reported chronic ICA recanalization confirmed histologically [19]. Mao et al. documented recanalization in three patients with vascular risk factors and collateral circulation—timing varied from one week to seven years [7].
Functional outcomes vary. Some patients recover neurologically, while others do not due to irreversible damage.
The possibility of recanalization without thrombolysis or intervention suggests conservative management may be viable when standard therapies are inaccessible.
Ultimately, timing is critical to prognosis. The phenomenon prompts reconsideration of thrombolysis indications and highlights the need for more research to refine patient selection.
Conclusion
Spontaneous recanalization of the middle cerebral artery is a recognized but not fully understood phenomenon that may occur in a subset of patients with ischemic stroke. Advances in neuroimaging have enhanced the detection and characterization of this entity; however, uncertainties persist regarding its true incidence, underlying pathophysiological mechanisms, and optimal therapeutic approach. Future investigations involving standardized imaging protocols and larger patient cohorts are essential to clarify these aspects and inform evidence-based clinical management.
Although the precise mechanisms have not been fully elucidated, spontaneous recanalization appears to be influenced by a combination of thrombotic, hemodynamic, and collateral factors. It may occur during both the early and late phases of atherosclerotic occlusion of the middle cerebral artery. The clinical impact is highly variable and depends on the timing of recanalization, the degree of pre-existing ischemic injury, and the extent of cerebral perfusion preserved during the occlusive event.
Recognition of this phenomenon holds significant implications for therapeutic decision-making, particularly in refining selection criteria for intravenous thrombolysis or mechanical thrombectomy. Further research is warranted to identify predictive biomarkers and to establish evidence-based guidelines for the management of patients with spontaneous arterial recanalization.
References
- Bogousslavsky J, Despland PA, Regli F. Spontaneous carotid dissection with acute stroke. Arch Neurol. 1987; 44: 137–140.
- Buslovich S, Hines GL. Spontaneous recanalization of chronic internal carotid artery occlusions: report of 3 cases. Vasc Endovascular Surg. 2011; 45: 93–97.
- Camporese G, Labropoulos N, Verlato F, et al. Benign outcome of objectively proven spontaneous recanalization of internal carotid artery occlusion. J Vasc Surg. 2011; 53: 323–329.
- Fieschi C, Bozzao L. Transient embolic occlusion of the middle cerebral and internal carotid arteries in cerebral apoplexy. J Neurol Neurosurg Psychiatry. 1969; 32: 236–240.
- Jadhav AP, Desai SM, Jovin TG. Indications for mechanical thrombectomy for acute ischemic stroke: current guidelines and beyond. Neurology. 2021; 97.
- Kassem-Moussa H, Graffagnino C. Nonocclusion and spontaneous recanalization rates in acute ischemic stroke: a review of cerebral angiography studies. Arch Neurol. 2002; 59: 1870.
- Klonaris C, Alexandrou A, Katsargyris A, Liasis N, Bastounis E. Late spontaneous recanalization of acute internal carotid artery occlusion. J Vasc Surg. 2006; 43: 844–847.
- Lee CY, Ryu CW, Koh JS, Kim GK. Late spontaneous recanalization of chronic middle cerebral artery occlusion. Neurointervention. 2012; 7: 113.
- Lui F, Hui C, Khan Suheb MZ, Patti L. Ischemic stroke. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2025.
- Mao Y, Huang Y, Zhang L, Nan G. Spontaneous recanalization of atherosclerotic middle cerebral artery occlusion: case report. Medicine (Baltimore). 2017; 96: e7372.
- Neumann-Haefelin T, Du Mesnil De Rochemont R, Fiebach JB, et al. Effect of incomplete (spontaneous and postthrombolytic) recanalization after middle cerebral artery occlusion: a magnetic resonance imaging study. Stroke. 2004; 35: 109–114.
- Oster JM, Aggarwal P. Spontaneous recanalization of the basilar artery with conservative management months after symptom onset. Neurol Int. 2009; 1: 17.
- Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a meta-analysis. Stroke. 2007; 38: 967–973.
- Weng L, Yao D, Wang R. Unusual images of ischemic stroke with hyperacute spontaneous recanalization: a case report. Ann Transl Med. 2020; 8: 1026.
- Wu H, Liu Y, Li B, Zhang H, Liu C. Prognosis of patients with late spontaneous recanalization of the atherosclerotic occlusion of internal carotid arteries: a pilot case series. Exp Ther Med. 2018.
- Xu Y, Qian G, Wei L, et al. Predictive factors for the spontaneous recanalization of large and middle cerebral arteries after acute occlusion. J Stroke Cerebrovasc Dis. 2016; 25: 1896–1900.
- Zanette EM, Roberti C, Mancini G, Pozzilli C, Bragoni M, Toni D. Spontaneous middle cerebral artery reperfusion in ischemic stroke: a follow-up study with transcranial Doppler. Stroke. 1995; 26: 430–433.
