
Open Access, Volume 11
Rare pleomorphic adenoma in the nasal cavity: A case study
Teya van Biljouw1*; Matthew Fries2; Dinesh Rugnath2; Zhong Zheng3
1Trinity Medical Science University, St. Vincent and the Grenadines, USA.
2Department of Pathology, Houston Healthcare Georgia, USA.
3Department of Otolaryngology, Houston Healthcare Georgia, USA.
Teya van Biljouw
Trinity Medical Science University, St. Vincent and the Grenadines, USA.
Email: teya.vanbiljouwbath.22@tmsu.edu.vc
Received : May 28, 2025,
Accepted : June 23, 2025
Published : June 30, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Background: Pleomorphic adenomas are the most common salivary gland tumors found in the parotid gland. Comparatively, intranasal pleomorphic adenoma is a rare pathology. Surgical excision of histopathological analysis is required for definitive diagnosis and classically presents with myoepithelial cells in a myxoid stroma, with possible pseudopodia. Complete surgical excision is the mainstay treatment to reduce risk of recurrence.
Case details: We present a case of a pleomorphic adenoma in the anterior nasal cavity in a 76-year-old female. The patient reported symptoms of a nasal mass associated with facial pressure and intermittent nasal crusting and epistaxis.
Conclusion: Pleomorphic adenomas, while rare, can occur outside the salivary glands. Early diagnosis with histopathology, complete surgical resection and ongoing surveillance can ensure good prognosis and reduce the risk of recurrence. These benign tumors should be considered in differential diagnoses of patients presenting with nasal mass.
Keywords: Pleomorphic adenoma; Intranasal; Benign salivary gland tumors.
Abbreviations: CT: Computed Tomography; NSE: Neuron Specific Enolase; INSM-1: Insulinoma-Associated Protein 1; PLAG1: Pleomorphic Adenoma Gene 1; SRY: Sex-Determining Region Y gene; MRI: Magnetic Resonance Imaging; CXPA: Carcinoma Ex Pleomorphic Adenoma; v-Myb: Avian Myeloblastosis Viral Oncogene Homolog.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © van Biljouw T (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: van Biljouw T, Fries M, Rugnath D, Zheng Z. Rare pleomorphic adenoma in the nasal cavity: A case study. Open J Clin Med Case Rep. 2025; 2364.
Introduction
Pleomorphic adenoma, also known as a benign mixed tumor, is a benign neoplasm and is the most common salivary gland tumors representing approximately 70-80% of all benign growths [1]. Pleomorphic adenomas present most commonly in women and in the middle age of life as a painless, mobile and slow growing tumor with high rates of recurrence, but low risk of malignant transformation [2]. Existing literature reports rare cases of pleomorphic adenomas outside the salivary glands arising from the nasal septal mucosa [3], external auditory canal [4], lacrimal gland [5] and oropharynx [3,6]. We present a case report of a pleomorphic adenoma centered on the anterior head of interior turbinate with extension to the nasal floor and nasal septum.
Case Presentation
A 76-year-old female patient presented to their primary care physician with progressive worsening nasal obstruction on the left side with ipsilateral intermittent epistaxis and nasal crusting. She also reported facial pressure without recurrent sinus infections. The patient denied any tobacco use.
On physical exam, the patient showed normal external nasal landmarks. Anterior rhinoscopy showed intact but deviated nasal septum, and a tan yellowish mass adjacent to the nasal septum with some mucopurulence. Maxillofacial Computed Tomography (CT) scan showed a homogenous 14 mm by 18 mm left anterior nasal cavity mass involving the anterior aspect of inferior turbinate with mass effect on the nasal septum (Figure 1). The patient was then consented and underwent excision of the left nasal mass with concurrent septoplasty and inferior turbinate submucosal resection. Intraoperatively, the mass was found to be solid in consistency, and was removed in piecemeal fashion to gross total resection. During the post operative period, office nasal endoscopy showed irregular mucosal tissue along the anterior inferior turbinate and nasal floor concerning for residual disease. The patient was then referred to tertiary care for complete excision. Additional resection was performed including partial resection of the inferior turbinate and mucosa lining the anterior inferior nasal septum and nasal floor. Further follow-up 12 months post operatively showed no residual disease or recurrence.
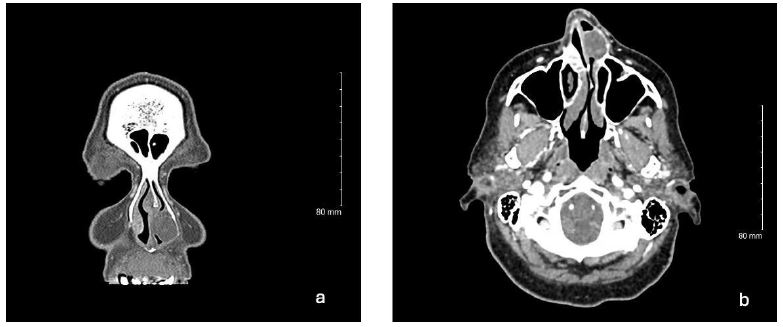
Figure 1: Representative images of coronal (a) and axial (b) Computed Tomography (CT) with contrast Left anterior nasal cavity mass involving anterior inferior turbinate with extension to nasal floor and nasal septum. No gross bony changes.
Histopathological analysis demonstrated the presence of a submucosal lesion comprised of ductal epithelial cells, rare squamous nodules, ovoid to spindled myoepithelial cells and chondromyxoid stroma. Gross examination revealed a mass measuring 2.5×1.9×1.2 cm with bone and cartilage. Immunohistochemical staining was positive for pan-cytokeratin and Cam 5.2 in tubules as well as S100 in myoepithelial cells. The sample was negative for NSE (Neuron Specific Enolase), Synaptophysin and INSM-1. The histomorphological features are compatible with a pleomorphic adenoma without evidence of malignancy (Figures 2-4).
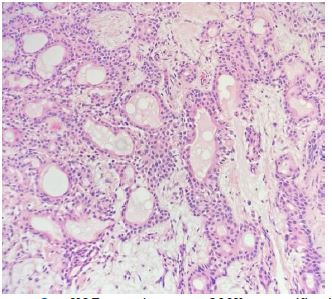
Figure 2: H&E section at 200X magnification demonstrates a benign pleomorphic adenoma. Ovoid to spindled myoepithelial cells and chondromyxoid stroma present.
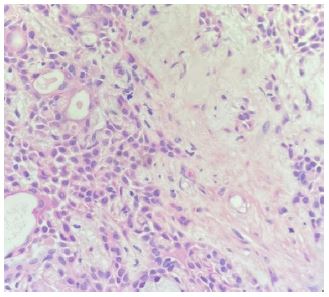
Figure 3: H&E section at 400X magnification emphasizing the chondromyxoid stromal tissue.
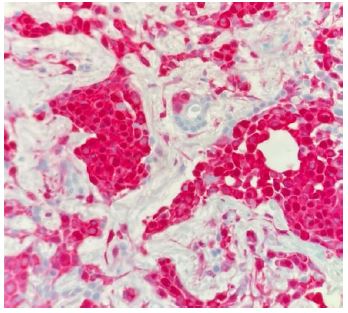
Figure 4: S100 at 400X magnification staining the myoepithelial cells.
Discussion/conclusions
Pleomorphic adenomas are the most common benign neoplasms found in salivary glands, but rarely present in the oral cavity, oropharynx, and nasal cavity [3,7]. Based on a review of literature, intranasal pleomorphic adenomas have an incidence of 0.4% and more commonly present in female patients over the age of 50, with variable presentations including nasal obstruction, epistaxis, facial dysmorphia, and headache [8-10]. Vento et al. (2016) reported ten cases of nasal cavity pleomorphic adenomas with symptoms such as epistaxis, unilateral obstruction, and nasal deformity [10]. Six originated from the nasal septum and three from the anterior inferior turbinate. Similarly, Compagno and Wong (1977) described 40 intranasal myxoid tumors, predominantly arising from the nasal septum [11].
Pleomorphic adenomas are diagnosed through biopsy and histopathologic analysis which reveals chondroid and myoepithelial cells in a myxoid stroma. However, histological presentations of pleomorphic adenomas exist on a spectrum due to the varying predominance of mesenchymal stroma, myoepithelium, and epithelium in any given mass [2]. Based on a review of literature, several oncoproteins are involved in the formation of these benign salivary gland tumors including pleomorphic adenoma gene 1 (PLAG1), SRY-related HMG-box 10 (SOX10), avian myeloblastosis viral oncogene homolog (v-Myb). Staining for these markers can aid in diagnosis when there is unclear histology [12].
Other diagnostic methods include fine-needle aspiration cytology but cannot reliably exclude adenoid cystic carcinoma and polymorphous adenocarcinoma, which require histopathological analysis [2]. CT with contrast is frequently used for evaluation and surgical planning. Magnetic Resonance Imaging (MRI) provides more accurate soft tissue resolution and architecture, with T2-weighted imaging highlighting hyperintensity due to the chondroid stromal tissue. However, definitive diagnosis can only be made based on histology, and no imaging findings are diagnostic.
Complete surgical excision with negative margins is the primary treatment for pleomorphic adenomas [13]. Gross total resection may miss all the microscopic pseudopodia of the mass, which may lead to recurrence months to years later [14-16]. The risk of recurrence also increases with larger masses, as reported in 3 cases by Compagno and Wong where surgical excision may have exposed the normal tissue to tumor stroma [11]. Existing literature suggests that adjuvant post operative radiation therapy poses a risk for malignant transformation of pleomorphic adenomas but may be considered in cases of positive surgical margins [17,18]. Pleomorphic adenomas arising from the nasal mucosa typically have a favorable prognosis due to early detection prompted by their mass effect and symptomatic presentation [19]. However, 2.4% of intranasal pleomorphic adenomas can become malignant known as Carcinoma Ex Pleomorphic Adenoma (CXPA) [8]. To our knowledge, only five cases of intranasal CXPA have been reported in the literature [11,20,21,22]. In contrast, pleomorphic adenomas of the parotid gland have a higher risk of transformation into CXPA, 1.5% at 5 years and 10% at 15 years respectively, rising with greater mitotic activity and hyalinization in the tissue [23]. Prolonged presence of the tumor also increases the risk of malignant transformation [24]. Further research into intranasal pleomorphic adenomas and CXPA could improve patient counseling, surgical planning especially when adjacent to important anatomic structures, and surveillance for recurrence.
Conclusion
We present a case of an intranasal pleomorphic adenoma involving the inferior turbinate and septum managed by complete surgical excision. We reviewed available literature to provide a comprehensive review of current evaluation and management of nasal pleomorphic adenoma. Early diagnosis and complete surgical excision with negative margins ensure good prognosis and reduced risk of recurrence. Nasal pleomorphic adenoma should be considered in evaluation of nasal masses and can be confirmed with histologic analysis of biopsy or surgical excision specimen. Risk of recurrence could be reduced by proper surgical technique and vigilant post operative surveillance. To our knowledge, there have been only a few reported cases of malignant transformation of nasal pleomorphic adenoma. This may be related to early diagnosis and continued surveillance of endoscopic mucosal surface.
References
- Zhan KY, Khaja SF, Flack AB, Day TA. Benign parotid tumors. Otolaryngol Clin North Am. 2016; 49: 327-42.
- Lingam RK, Daghir AA, Nigar E, Abbas SA, Kumar M. Pleomorphic adenoma (benign mixed tumour) of the salivary glands: its diverse clinical, radiological, and histopathological presentation. Br J Oral Maxillofac Surg. 2011; 49: 14-20.
- Sciandra D, Dispenza F, Porcasi R, Kulamarva G, Saraniti C. Pleomorphic adenoma of the lateral nasal wall: case report. Acta Otorhinolaryngol Ital. 2008; 28: 150.
- Lahoz MT, Valerio J, Royo J, Yus C, Camora F. Tumor mixto de conducto auditivo externo. Acta Otorrinolaringol Esp. 1990; 41: 53-6.
- Suzuki K, Moribe K, Baba S. A rare case of pleomorphic adenoma of lateral wall of nasal cavity, with special reference of statistical observation of pleomorphic adenoma of nasal cavity in Japan. Nippon Jibiinkoka Gakkai Kaiho. 1990; 93: 740-5.
- Campos A, Bagan JV, Zapater E, Martorell M, Basterra J. Adenoma pleomorfo de glandula salivar accessoria. Acta Otorrinolaringol Esp. 1995; 46: 331-4.
- Almeslet AS. Pleomorphic adenoma: a systematic review. Int J Clin Pediatr Dent. 2020; 13: 284-7.
- Mead K, Kuhar H, Ibrahim N, Adelman M, Zehr B, Schoenfield L, et al. Pleomorphic adenoma of the nasal cavity: a case study. Otolaryngol Case Rep. 2022; 23: 100408.
- Cimino-Mathews A, Lin BM, Chang SS, Boahene KD, Bishop JA. Carcinoma ex pleomorphic adenoma of the nasal cavity. Head Neck Pathol. 2011; 5: 405-9.
- Vento SI, Numminen J, Kinnunen I, Rautiainen M, Tarkkanen J, Hagström J, et al. Pleomorphic adenoma in the nasal cavity: a clinicopathological study of ten cases in Finland. Eur Arch Otorhinolaryngol. 2016; 273: 3741-5.
- Compagno J, Wong RT. Intranasal mixed tumors (pleomorphic adenomas): a clinicopathologic study of 40 cases. Am J Clin Pathol. 1977; 68: 213-8.
- Lee JH, Kang HJ, Yoo CW, Park WS, Ryu JS, Jung YS, et al. PLAG1, SOX10, and Myb expression in benign and malignant salivary gland neoplasms. J Pathol Transl Med. 2019; 53: 23-30.
- Henriksson G, Westrin KM, Carlsöö B, Silfverswärd C. Recurrent primary pleomorphic adenomas of salivary gland origin: intrasurgical rupture, histopathologic features, and pseudopodia. Cancer. 1998; 82: 617-20.
- Kumar V, Abbas AK, Aster JC. Robbins and Cotran pathological basis of disease. 9th ed. Philadelphia: Elsevier. 2015: 744-5.
- Bokhari MR, Greene J. Pleomorphic adenoma [Internet]. Treasure Island (FL): StatPearls Publishing. 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430829/
- Aryal GR, Shrestha N, Basnet M, Shrestha O, Sharma P. Pleomorphic adenoma of nasal septum, an unusual site: a case report from Nepal. Oxf Med Case Rep. 2023; omac152.
- Saksela E, Tarkkanen J, Kohonen A. The malignancy of mixed tumors of the parotid gland: a clinicopathological analysis of 70 cases. Acta Otolaryngol. 1970; 70: 62-70.
- Bradley PJ. The recurrent pleomorphic adenoma conundrum. Curr Opin Otolaryngol Head Neck Surg. 2018; 26: 134-41.
- Golz A, Ben-Arie Y, Fradis M. Pleomorphic nasoseptal adenoma. J Otolaryngol. 1997; 26: 399-401.
- Freeman SR, Sloan P, Carpentier J. Carcinoma ex-pleomorphic adenoma of the nasal septum with adenoid cystic and squamous carcinomatous differentiation. Rhinology. 2003; 41: 118-21.
- Cho KJ, el-Naggar AK, Mahanupab P, Luna MA, Batsakis JG. Carcinoma ex-pleomorphic adenoma of the nasal cavity: a report of two cases. J Laryngol Otol. 1995; 109: 677-9.
- Yazibene Y, Ait-Mesbah N, Kalafate S, Yahi-Ait Mesbah N, Abdennebi A, Bouzid H, et al. Degenerative pleomorphic adenoma of the nasal cavity. Eur Ann Otorhinolaryngol Head Neck Dis. 2011; 128: 37-40.
- Lobo R, Hawk J, Srinivasan A. A review of salivary gland malignancies: common histologic types, anatomic considerations, and imaging strategies. Neuroimaging Clin N Am. 2018; 28: 171-82.
- Seethala RR, Barnes EL. Common malignant salivary gland epithelial tumors. Surg Pathol Clin. 2011; 4: 1177-215.
