
Open Access, Volume 11
A rare case of neural epidermal growth factor-like 1 protein positive membranous nephropathy
Hridya Harimohan1*; Jean Hou2; Sabitha Eppanapally1
1Department of Internal Medicine, Kern Medical, California, USA.
2Department of Pathology, Cedars Sinai, California, USA.
Hridya Harimohan
Department of Internal Medicine, Kern Medical, California, USA.
Email: hridyaharimohan@gmail.com
Received : May 27, 2025,
Accepted : June 16, 2025
Published : June 30, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Membranous nephropathy is a leading cause of nephrotic syndrome in adults, often resulting from immune complex deposition in the glomeruli. In primary cases, antibodies target podocyte antigens, while secondary forms arise from external immune complex deposition. Known antigens in primary disease include PLA2R and THSD7A; however, a novel antigen, NELL-1, has been identified in PLA2R-negative cases and is often linked to cancer.
A 50-year-old woman with dyslipidemia and a history of deep vein thrombosis presented with four months of leg swelling, recently worsened. She had no personal or family history of kidney, autoimmune, or malignant disease but reported 22 years of pesticide exposure. Her labs showed severe hypoalbuminemia, high cholesterol, marked proteinuria, and normal kidney function. Autoimmune and infectious tests were negative. Kidney biopsy confirmed NELL-1 positive membranous nephropathy, with no evidence of malignancy. She was treated with prednisone, losartan, and diuretics, resulting in resolved edema and improved proteinuria over a year, though significant levels persisted.
NELL-1-associated membranous nephropathy is rare and typically linked to malignancy. In this case, no cancer was found, suggesting a possible environmental trigger such as pesticide exposure. Similar associations have been noted with mercury exposure. Further research is needed to understand non-malignant triggers of NELL-1 positive disease.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Harimohan H (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Harimohan H, Hou J, Eppanapally S. A rare case of neural epidermal growth factor-like 1 protein positive membranous nephropathy. Open J Clin Med Case Rep. 2025; 2361.
Introduction
Membranous Nephropathy (MN) is one of the most common causes of nephrotic syndrome in adults, accounting for approximately 30% of biopsy-proven cases in this population. It is characterized histologically by the thickening of the glomerular basement membrane due to subepithelial immune complex deposition. MN can be classified into two major forms: primary (idiopathic) and secondary. Primary MN is typically caused by autoantibodies directed against intrinsic antigens on podocytes, such as the M-type Phospholipase A2 Receptor (PLA2R) and Thrombospondin type-1 Domain-Containing 7A (THSD7A), which together account for the majority of known antigenic targets in primary MN [1].
However, a subset of patients with PLA2R- and THSD7A-negative MN were historically considered idiopathic until recent discoveries identified new antigens. Among these, Neural Epidermal Growth Factor-like 1 (NELL-1) has emerged as a significant target antigen in MN, especially in patients negative for PLA2R and THSD7A. NELL-1-associated MN has shown a strong correlation with malignancies, particularly solid tumors, raising the possibility of a paraneoplastic mechanism in some cases. Nevertheless, NELL-1 positive MN has also been reported in patients without identifiable malignancy, suggesting that other environmental or immunologic triggers may be involved [2].
Interestingly, environmental exposures, such as mercury in skin-lightening creams, have been implicated in NELL-1-associated MN [3]. Such findings have opened discussions about a possible role of environmental toxins or heavy metals in the pathogenesis of this disease. Further research is required to clarify these associations and to understand the mechanisms by which NELL-1 becomes a target antigen in MN, especially in the absence of malignancy [4].
Case Presentation
50-year-old female with past medical history of the dyslipidemia, reported history of deep vein thrombosis on anticoagulation presented to the emergency department because of bilateral lower extremity edema for four months with acute versioning for two days. She denied shortness of breath, cough, chest pain, palpitations, easy bruise, jaundice, abdominal distension or any upper respiratory infection prior to the onset of symptoms. She denied any significant loss of appetite or weight. She denied any past medical history of kidney disorders, autoimmune disorders or cancer. She was treated with Apixaban and furosemide by primary care and was lost to follow up with nephrologist. She had been working in the fields handling pesticide for 22 years. She denied any personal or family history of cancer, autoimmune conditions, cardiac, lung or kidney disorders. She denied smoking, alcohol or drug use. However, she endorsed taking herbal supplements for 3 weeks which was after the initial onset of her swelling of legs. At the initial time of presentation to the hospital, she was hemodynamically stable with heart rate of 78 beats per minute, blood pressure 115/76 mg of Hg, temperature of 36.9°C, respiratory rate of 16 per minute, oxygen saturation of 99% in room air. Physical examination significant for bilateral pitting pedal edema extending up the knees with no significant swelling around the eyelids. Ultrasound duplex was negative for deep vein thrombosis of bilateral legs. Laboratory studies are as follows:
Renal biopsy (Figure 1) showed secondary membranous nephropathy with strong possibility of cancer with PLA 2 R receptor negative and thrombospondin. However, NELL- 2 was positive. Age-appropriate cancer screening was unremarkable. She was treated with Prednisone 40 mg daily with tapering dose with steroid precautions along with lisinopril and Lasix 40 mg daily. She continues to have significant proteinuria, however, proteinuria improved over a period of 1 year. She is continued to be followed up for proteinuria and for further developments of symptoms if any.
| Value | Reference Range | ||
|---|---|---|---|
| Urinary studies (unit) | Urine albumincreatinine ratio (mcg/mgCr) | 10,813 (HIGH) | 0-30 |
| Urine creatinine (mg/dl) | 209 | 29-226 | |
| Urine microabumin (mg/L) | 22,600 (HIGH) | 0-30 | |
| Urinalysis | Urine ketones | Trace (<10) | Negative <5 |
| Blood | Moderate | Negative | |
| Protein | >600 (HIGH) | Negative | |
| RBC | 22-50 (HIGH) | <2 | |
| WBC | 10-20 (HIGH) | <2-5 | |
| Dysmorphic RBC | Present | Absent | |
| Granular cast | 2 | Few or none | |
| Hyaline casts | >20 (HIGH) | 0-5 | |
| Lipid panel | Cholesterol(mg/dl) | 352 (HIGH) | <200 |
| Triglyceride(mg/dl) | 131 | <150 | |
| LDL(mg/dl) | 210 (HIGH) | <100 | |
| HDL(mg/dl) | 116 | >60 | |
| Laboratory Studies | Albumin(g/dl) | 0.9 (LOW) | 3.4-5.4 |
| Total Protein(g/dl) | 4.2 | 6.0-8.3 | |
| Creatinine (mg/dl) | 0.9 | 0.6-1.1 | |
| Effective Glomerular Fraction Rate (ml per minuteper 1.73 m²) | 186 | >120 | |
| Anti-nuclear antibody | Negative | ||
| c-Anti nuclear cytoplasmic antibody | Negative | Negative | |
| p-Anti nuclear cytoplasmic antibody | Negative | Negative | |
| Atypical-Anti nuclearcytoplasmic antibody | Negative | Negative | |
| Sjogrens Antibody | Negative | Negative | |
| Sm RNP | Negative | Negative | |
| Centromere B antibody | Negative | Negative | |
| Complement C3 | 164 | 83-93 | |
| Complement C4 | 45 | 15-57 | |
| Cryoglobulins | Negative | Negative | |
| Phospholipaseantibody | Negative | Negative | |
| SPEP Protein | 3.7 (low) | 6.1-8.1 | |
| SPEP albuminlevel | 1.5 (low) | 3.8-4.2 | |
| SPEP alpha-1 globulin | 0.2 | 0.2-0.3 | |
| SPEP alpha-2 globulin | 1.2 (slightly high) | 0.5-0.9 | |
| SPEP beta-1 globulin | 0.2 (low) | 0.4-0.6 | |
| SPEP beta-2 globulin | 0.3 | 0.2-0.5 | |
| SPEP gammaglobulin | 0.3 (low) | 0.8-1.7 | |
| Hepatitis B surface Ag | Negative | Negative | |
| Hepatitis C antibody | Negative | Negative | |
| HbA1c(%) | 5.3 | 4-5.6 |
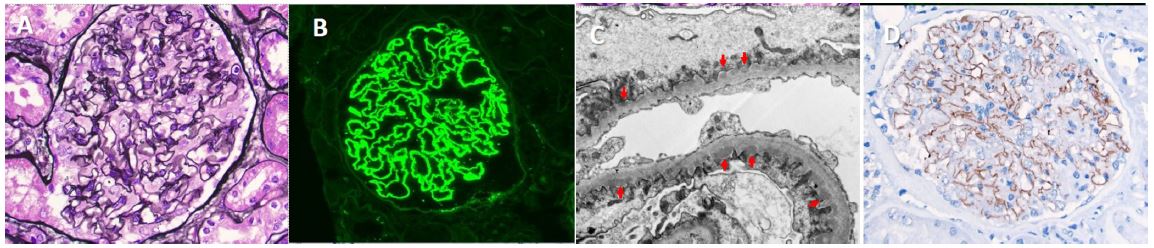
Figure 1: Renal Biopsy: (A) Electron microscopy showing normal glomeruli; (B) Immunofluorescence microscopy showing deposits of NELL-1 protein along basement membrane; (C) Electron microscopy showing subepithelial deposits of immunoglobulin complexes; (D) Immunohistochemistry imaging showing glomerulus with fine granular positivity along basement membrane.
Discussion
NELL-1 associated membranous nephropathy is a rare and unique variant of membranous nephropathy, predominantly associated with malignancy. Consequently, our case appears even more distinctive, as a comprehensive evaluation for malignancy-including imaging, tumor markers, and age-appropriate cancer screenings-yielded unremarkable results. This is notable given that NELL-1 associated membranous nephropathy has a strong and increasingly recognized association with malignancy. It has been demonstrated that cancer cells can express NELL-1 antigen, and antibodies generated against these antigens contribute to the pathogenesis of membranous nephropathy [5]. Despite this established link, our patient exhibited no clinical signs, laboratory findings, or imaging suggestive of underlying malignancy.
The patient’s history of Deep Vein Thrombosis (DVT) may instead be attributable to complications associated with nephrotic syndrome, particularly given the absence of malignancy. Thromboembolic events, including DVT and pulmonary embolism, are well-documented complications of nephrotic syndrome, especially in patients with membranous nephropathy. This hypercoagulable state is thought to result from urinary loss of anticoagulant proteins such as antithrombin III and increased hepatic synthesis of procoagulant factors [6].
Infectious causes of secondary membranous nephropathy, including HIV, Hepatitis B Virus (HBV), and Hepatitis C Virus (HCV), were systematically ruled out. Although HIV-associated NELL-1 positive membranous nephropathy has been previously reported, our patient tested negative for these viral infections. Additionally, there have been reports of mercury-related NELL-1 positive membranous nephropathy, particularly linked to the use of mercury-containing skin lightening cosmetics. In such cases, NELL-1 was identified as the antigenic target of mercury-induced immune responses responsible for membranous nephropathy [7].
In our patient’s case, there was no known use of mercury-containing products; however, she reported a prolonged history of pesticide exposure due to occupational and environmental factors. Although the specific chemical compounds involved were not identified, environmental toxins including certain pesticides have been implicated in renal injury and glomerular diseases. Pesticides such as organochlorines and organophosphates have been associated with immunomodulatory effects and renal tubular toxicity, and may conceivably contribute to an antigen-antibody mediated glomerular injury, although direct links to NELL-1 expression or antibody formation remain speculative [8]
Given the absence of malignancy, infection, or overt toxin exposure with known NELL-1 antigenicity, this case highlights the need for further investigation into the environmental and idiopathic triggers of NELL-1 associated membranous nephropathy. Additionally, the identification of NELL-1 as a target antigen in a subset of apparently idiopathic membranous nephropathy cases underscores the expanding spectrum of this disease and necessitates a broader search for potential environmental and occupational contributors.
Conclusion
Given that one third of individuals with NELL -1 associated membranous nephropathy have underlying cancer, prompt and detailed evaluation of malignancy is recommended. Nonetheless, the relationship between NELL 1 titers and malignancy risk remains uncertain. Additionally, further investigation is required to ascertain the etiology of NELL -1 positive membranous nephropathy, particularly its association with heavy metal exposure. Additionally, HIV associated, lipoic acid supplementation, hematopoetic supplementation have been reported to play a role in pathogenesis of NELL 1 positive membranous nephropathy. Moreover, further research is needed exploring the pathogenesis behind NELL 1 associated membranous nephropathy which would be beneficial for identifying specific therapy options for NELL 1 specific membranous nephropathy.
References
- Sethi S, Debiec H, Madden B, Charlesworth MC, Morelle J, Gross L, et al. Neural epidermal growth factor-like 1 protein (NELL-1) associated membranous nephropathy. Kidney Int. 2020; 97: 163-174.
- Alsharhan L, Beck LH Jr. Membranous Nephropathy: Core Curriculum 2021. Am J Kidney Dis. 2021; 77: 440-453.
- Sharma Y, Jain A, Gupta P, Tiwari V, Gupta A, Bhargava V, et al. NELL-1 Associated Membranous Nephropathy - A Case Series from India. Indian J Nephrol. 2024; 34: 654-656.
- Ronco P, Plaisier E, Debiec H. Advances in Membranous Nephropathy. J Clin Med. 2021; 10: 607.
- Mohamed Jiffry MZ, Pitts K, Munir M, Khan A, Josephs M. A Rare Case of Neural Epidermal Growth Factor-Like 1 Protein (NELL-1) Antigen-Associated Membranous Nephropathy. Cureus. 2023; 15: e34713.
- Nassar R, Kadhem SA, Shakir M. Lipoic Acid as a Trigger for NELL-1 Positive Membranous Nephropathy. Kans J Med. 2023; 16: 297-298.
- Alsharhan L, Beck LH Jr. Membranous Nephropathy: Core Curriculum 2021. Am J Kidney Dis. 2021; 77: 440-453.
- Sultan A, Mamankar D, Thakare S, Rojekar A, Jamale T. Mercury-associated Neural Epidermal growth factor-Like 1 protein (NELL-1) positive membranous nephropathy after use of skin lightening creams. Clin Toxicol (Phila). 2023; 61: 387-391.
