
Open Access, Volume 11
Clinical evaluation and vision of treatment in tibial pilon fractures
Horacio Tabares Sáez1*; Horaio Tabares Neyra2
1Transylvania University of Brasov, Romania.
2Havana Medical University, Cuba.
Horacio Tabares Sáez
Transylvania University of Brasov, Romania.
Email: horacio_tabares@hotmail.com
Received : May 15, 2025,
Accepted : June 10, 2025
Published : June 30, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Tibial pilon fractures are due to an axial load that pushes the talus towards the pylon, resulting in joint impaction of the distal tibia. There are multiple treatment options for these fractures; Excellent results have been reported with open fixation, but with high incidence rates of complications, especially related to the skin and soft tissues. The purpose of this article is to review the data of interest related to clinical evaluation and treatment vision.
Method: References were identified by searching PubMed, Google Scholar and Elsevier for publications between 2013-2025 in English with the terms: ‘treatment of tibial pilon fractures’, ‘treatment of fractures of the distal end of the tibia’ and ‘treatment of metaphyso-articular fractures of the distal tibia’.
Development: An adequate prior clinical evaluation and imaging exams are required to allow the correct vision of the problem. The assessment must be carried out in a systematized way, the condition of the skin is fundamental. Imaging studies are important with lateral AP radiographs and mortise projection. The CT scan is essential for a better understanding of the fracture pattern, it shows the number of joint fragments, their degree of displacement and possible presence of bone impaction. Treatment is conditioned by variables such as type of injury, state of bone tissue, soft tissues and possible technical difficulties and can be conservative or surgical.
Conclusion: Tibial pilon fractures represent a challenge for orthopedic surgeons. The combination of articular cartilage injury, metaphyseal comminution, and soft tissue damage has often resulted in historically unfavorable outcomes.
Keywords: Tibia; Pylon; Fracture; Clinical evaluation; Treatment.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Sáez HT (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Sáez HT, Neyra HT. Clinical evaluation and vision of treatment in tibial pilon fractures. Open J Clin Med Case Rep. 2025; 2359.
Introduction
Tibial pilon fractures affect the distal metaphyseal epiphyseal area of the tibia. They are rare and account for 1% of all fractures and between 7% and 10% of all tibia fractures; The typical patient is a young man between the ages of 30 and 50. They occur most frequently after high-energy trauma or may result from high-velocity injuries and affect the load-bearing surface of the distal tibia [1].
These fractures are due to an axial load pushing the talus into the pilon, resulting in joint impaction of the distal tibia; The position of the foot at the moment of impact, along with the direction and amplitude of the force, produce different fracture patterns and degrees of comminution. Intra-articular fractures of the distal tibia can also be caused by rotational force with minimal axial load [1,2].
The rate of open fractures varies greatly depending on the mechanism of injury, with up to 50% in high-energy trauma [1].
These fractures represent a therapeutic challenge among all orthopaedic traumas due to their extraordinary complexity and the high rate of secondary complications, which can reach up to 50%. Therefore, this distal area of the tibia must be properly managed to preserve the function of the ankle joint. The long-term outcome is often poor, and correct initial management is crucial [3].
There are multiple treatment options for tibial pilon fractures, and none are considered the standard treatment. The evolution of treatment strategies for tibial pilon fractures has seen a shift from conservative management to surgical intervention, with the aim of restoring joint congruence and allow early mobilization [4].
Rüedi has described excellent results with open fixation, with 4% to 16% of pseudoarthrosis, but with high incidence rates of numerous other complications, especially related to the skin and soft tissues. That is why the management of this fracture is also complex due to the thin envelope of soft tissue that surrounds the distal tibia, which predisposes to the risk of complications and wound infection. In fact, another factor is that the cutaneous vascularization of the tibial pilon is precarious, with a high-risk anteromedial area fed only by the anterior tibial artery [5,6].
Since the early years of this century, treatment has evolved into a two-stage protocol, which today is practically the gold standard of care. However, additional new methods for treating soft tissue envelope are currently being researched and have already shown promising results for the future [7].
However, the optimal surgical approach and fixation method remain the subject of debate among the orthopedic community. The aim of this review is to summarize the protocols for the management of these difficult-to-treat fractures, to review the current literature on recent developments, and thereby to provide orthopedic surgeons with a better understanding and ability to manage tibial pilon fractures.
Search strategy and selection criteria
The references were identified by searching PubMed, Google Scholar and Elsevier for publications between 2013-2025 in English with the terms: ‘‘treatment of tibial pilon fractures’’, ‘‘treatment of fractures of the distal end of the tibia’’ and ‘‘treatment of metaphyso-articular fractures of the distal tibia’’. Articles accessible freely or through the Clinical key and Hinari services were also reviewed.
A number of articles were selected that make the necessary requirements to support this review. Articles were added that are more than ten years old, but that are key to the topic. We excluded papers because they were duplicates or the source data was insufficient. Power Point presentations were discarded.
Development
The initial step to be able to plan the type of treatment that is going to be used in the face of tibial pilon fractures, is to carry out an adequate prior clinical evaluation and imaging tests that provide a correct vision of the problem to be faced.
Clinical evaluation
The assessment of patients with distal tibia fractures should be carried out in a systematized manner to ensure a complete evaluation and prevent other associated injuries from going unnoticed. Special attention should be paid to the contralateral extremity and the thoracic and lumbar spine, especially when fractures are the result of falls from heights or traffic accidents [8].
In tibial pilon fractures, careful examination of the condition of the skin is essential, since soft tissue injuries of the distal part of the tibia are an important limiting factor in its treatment. The edema of the foot and ankle sets in quickly after injury. Open fractures typically present with traumatic wounds on the inside of the distal tibia or at the level of the fibula fracture. Closed but highly displaced fractures of the distal tibia can cause skin hyper pressure, endangering blood supply and causing skin necrosis [9].
On the other hand, other skin lesions such as abrasions, contusions, bruises or blistering lesions must be identified. Two types of cutaneous blisters have been described that seem to represent different degrees of skin involvement [4].
− Blisters with relatively clear fluid and fluid represent superficial epidermal lesions, Blood-filled blisters involve lesions of the entire thickness of the dermis.
The size, characteristics, and location of these bullous lesions may influence the definitive treatment of the fracture. As with all fractures, the neurovascular status of the limb should be explored. On the other hand, it is important to diagnose early the possible development of complications such as compartment syndrome, so it is necessary to perform periodic examinations, especially in high-energy fractures [4].
Image assessment
The radiological study of these fractures includes ankle radiographs in anteroposterior and lateral views and projection of the tibial shroud, which will allow us to know the fracture pattern [10].
It is very helpful to perform these X-rays by maintaining the fracture with traction at the level of the calcaneus. The projections that include the entire tibia serve to appreciate the extension towards metaphysis and diaphysis of the tibial pilon fracture. Contralateral ankle x-rays may provide a template for preoperative planning or may rule out the presence of less symptomatic associated fractures. The simple radiological study is completed with the evaluation of the spine and the assessment of other symptomatic areas of the musculoskeletal system, especially when the fracture is the result of a fall or high-energy trauma; also, when the patient is unconscious [10].
Computed Tomography (CT) is useful for a better understanding of the fracture pattern, this study shows the number of joint fragments, the degree of displacement of them and the possible presence of bone impaction. For some authors, carrying out this examination is mandatory. Three-dimensional reconstruction of the fracture allows for preoperative planning and serves as a guide for surgical treatment. CT is essential for planning the placement of fixative pins when using hybrid fixatives [11,12].
Traditionally, tibial pilon fractures have been classified according to the AO/OTA and Ruëdi-Allgöwer classification; However, these systems are based on plain radiographs and are not useful tools in terms of preoperative planning or prognostic indicators. Given these limitations, Leonetti and Tigani proposed a new classification system based on displacement, number of joint fragments, plane of the main fracture line, and degree of comminution observed on computed tomography. This is the only CT-based classification system described. In an associated study of 71 pylon fractures, they demonstrated that this new classification system is not only reproducible, but provides a prognostic correlation [12,14].
Regardless of which classification system is used, it is important to recognize that there is a high degree of variation between individual fractures. For this reason, a preoperative CT scan is vital to understanding the fracture and planning both surgical approaches and fixation.
Emergency room management
Since 6% of all tibial pilon fractures are seen in polytrauma patients, the patient should always be evaluated from baseline with the use of Advanced Trauma Life Support (ATLS) protocols in the emergency room. After life-threatening injuries have been ruled out, ankle fractures should be reduced as soon as possible with appropriate pain medication or anesthetic sedation during the procedure. Before and after reduction, a thorough neurovascular examination is essential. Early reduction reduces stress on neurovascular structures, which slows soft tissue inflammation, generally significantly decreases pain levels, and additionally decreases the chances of further joint cartilage damage and tissue necrosis [15].
Achieving a satisfactory anatomical reduction of the fracture can be quite difficult in very comminuted fractures or in those where trapped tissue or bone makes the fracture irreducible. In these cases, the use of temporary external fixation in terms of damage control surgery should be performed as quickly as possible to reduce the risks associated with extensive soft tissue damage [15,16].
After successful reduction, close observation of soft tissues is essential, as vascular injuries around the ankle are commonly seen in high-energy trauma and can lead to the development of compartment syndrome.
In open tibial pilon fractures, the wound should always be thoroughly cleaned, damaged tissues debridedand closed if possible (probably grade I and II open fractures). When soft tissue loss is too extensive or wound contamination is too severe, radical debridement, washing, treatment with a Vacuum-Assisted Closure device (VAC), and temporary external fixation may be necessary [17].
In addition, intravenous antibiotic therapy is essential and should be started as soon as possible.
Treatment
There are currently several therapeutic options available for tibial pilon fractures that are divided between conservative treatment and surgical treatment, the latter with a wide range of surgical techniques. These include external fixation, external fixation associated with internal osteosynthesis, and traditional open reduction and internal osteosynthesis. Given the importance of peri fracture soft tissues, new implants have been developed that include low-thickness plate designs that can be implanted along the inner aspect of the tibia with minimal approaches, almost percutaneously. One of the methods that is gaining popularity in the treatment of severe tibial pilon fractures is the use of the initial external fixator, followed by open reduction and delayed internal osteosynthesis. Regardless of the method used, the purposes of treatment are to achieve adequate joint reconstruction, physiological alignment of the limb, healing of bone and soft tissues, restore function, and avoid possible complications [10].
In general, treatment is conditioned by a series of variables that make it technically difficult and often uncertain results. These variables can be summarized as: [18]
(1) Type of injury and its mechanism.
(2) State of the bone tissue.
(3) Soft tissue condition.
(4) Technical difficulties.
The most important technical difficulties refer to the severe comminution of the articular surface, the impaction of the distal cancellous bone of the tibia, the presence of osteoporotic bone and the possible precarious state of the soft tissues. Tibial pilon fractures occur in a territory (the distal part of the lower limb), which has the worst microcirculation in the entire body [18].
Schatzker, in his book, stated that ‘‘in the face of these fractures, if it is decided to operate, and the specific objectives of anatomical reduction and stable internal fixation are not achieved, the result is disastrous, since the additional trauma of surgery is added to a limb that was already severely injured [19].’’
Therapeutic scheme
Possible treatment methods for these fractures are:
1. Bloodless reduction and plaster.
2. Surgical reduction and internal fixation.
3. Transcalcanealtransarticular stabilization of unstable fractures.
4. Percutaneous interlocking.
5. Skeletal traction and plaster.
6. Reduction with the help of devices such as the L. Böhler frame, and plaster with bipolar anchorage.
7. Osteotaxis or reduction with external fixator.
The decision on the type of treatment to be used in tibial pilon fractures requires the analysis of several important factors:
1. Degree of comminution of the tibial joint surface.
2. Possibility of reconstruction of the tibial metaphysis.
3. Integrity or not of the fibula.
4. Soft tissue condition.
5. Bone quality.
To these must be added general factors, such as the place and local conditions where the treatment is carried out, and importantly, the experience of the acting surgeon if he decides on a surgical treatment, this being fundamental.
Conservative treatment
There is a broad consensus that surgical reduction and fixation is the treatment of choice for pilon fractures. However, in an aging population, surgery may not be performed safely, in which case treatment consists of reduction and immobilization without weight-bearing for 6 to 10 weeks in a cast [19].
Closed reduction and immobilization with plaster casts do not allow adequate reduction of joint fragments and make it impossible to monitor the condition of the skin. In addition, reduction loss is quite frequent with this method.
Therefore, orthopedic treatment should be reserved for non-displaced fractures and for patients who have a high surgical risk and poor medical prognosis. Fracture distraction using calcaneal skeletal traction can achieve satisfactory alignment if the central part of the joint surface is not impacted. This technique allows direct access to soft tissues, elevation of the limb and can be combined with rehabilitation of the joint. For the management of the fracture with calcaneal traction alone, the patient needs to remain in bed until bone healing, usually for a minimum of 6 weeks [20].
Traction through the calcaneus may be the initial treatment in those fractures that require surgical intervention, but must be postponed due to the condition of the soft tissues. In these cases, the ligamentotaxis effect of calcaneal traction can achieve a temporary reduction while maintaining leg length until surgery can be performed safely [20].
Surgical treatment
When deciding on surgical treatment, consideration should be given to whether immediate total or staged management, open reduction and osteosynthesis, external fixation, and treatment protocols will be performed, taking into account general principles such as soft tissue conditions, timing of surgery, and reduction and containment planning (Table 1) [21].
Table 1: Change in clinical parameters from baseline (day of hospital admission): Pre and post use of first and second CytoSorb® device).
| Complex fractures: Surgery |
| Soft tissue status: Determines technique and timing, based on the Individuality of the case |
| Moment: |
| Palpable bony prominences |
| Skinfolds present (wrinkle sign) |
| Skinfolds present (wrinkle sign) |
| Absence of hemorrhagic phlyctena |
| Careful planning and reduction |
| Principles of osteosynthesis "4 steps"? |
| Bone graft contribution? |
| Key fragments? Screws-hinges-position? |
Early management vs. staged management
Until the end of the last century, it was considered that surgical treatment should be carried out as early as possible to reduce the length of hospital stays and the associated complications. Historically, some studies of acute open reduction and internal fixation of pylon fractures have demonstrated an unacceptably high rate of infections and wound complications [10].
Good results were reported when this type of treatment was used for low-energy injuries (Rüedi-Allgöwer I and II), but the results were poor in high-energy trauma, highly comminuted and displaced tibial pilon fractures, and when comorbidities were detected in the patient. Multiple individual studies showed an unacceptably high rate of infections (up to 40%) and wound complications resulting in a high rate of revision surgeries, pseudoarthrosis, osteomyelitis, poor functional outcome, and arthritis in treatments with early open reduction and internal fixation. The high complication rate was mainly attributed to severe iatrogenic trauma during open reduction over an already damaged soft tissue envelope [10].
Because of this extremely high complication rate, two-stage treatment was established, which remains the most commonly used treatment method for tibial pilon fractures. Numerous authors reported a significantly lower rate of complications, such as infections and pseudoarthrosis, and improved functional outcome with a two-stage treatment protocol.
Given the characteristics of the soft tissues surrounding the distal tibia, it is the state of these tissues that determines the timing of surgery and the possible degree of surgical damage that may occur. As a result, staged protocols were introduced, in which fractures are timed by employing calcaneal traction, splints, or external fixators until the soft tissue envelope is amenable to surgery. Unfortunately, there are no definitive clinical signs that determine the timing of definitive fixation. Surgeons frequently use the presence of wrinkles (Figure 1) or epithelialization of fracture blisters, but this is often a subjective idea [10].

Figure 1: Presence of wrinkles and epithelialization of phlyctenas.
Source. Bear J, Rollick N, Helfet D. Evolution in Management of Tibial Pilon Fractures. Current Reviews in Musculoskeletal Medicine. 2018; 11:537-45 doi.org/10.1007/s12178-018-9519-7
Source. Bear J, Rollick N, Helfet D. Evolution in Management of Tibial Pilon Fractures. Current Reviews in Musculoskeletal Medicine. 2018; 11:537-45 doi.org/10.1007/s12178-018-9519-7
In general, most surgeons agree that ‘‘skin wrinkles’’ seem to be the best indicator of the possibility of surgical treatment; which in most cases will occur between 10 and 14 days after the trauma. In fractures with extensive soft tissue damage and subsequent formation of fracture blisters, it has been suggested to postpone the surgical approach until re-epithelialization of the region is achieved. In addition, surgical approaches need to be limited due to the location of the blisters [15,22].
Open fractures need more careful analysis and may require multiple prior soft tissue surgeries with VAC treatment. External fixation may be a viable course of treatment for these open or severely injured soft tissue fractures [23,24].
Current staged protocols resulted in a decrease in wound complications; however, they have recently been questioned by the resurgence of early fixation, given the increased difficulty in achieving the correct reduction and adequate fixation of fragments [10].
Concerns about the quality of reduction, duration of surgery, increased healthcare costs, and infection of the pin insertion site with the use of external fixators have led several surgeons to proceed with definitive internal fixation acutely. Multiple recent studies have shown that fractures treated within 72 hours of surgery have comparable results to staged fixation. However, all these studies are retrospective reviews and the criteria for early fixation depends on the surgeon or the hospital center where they are performed [10,23].
The view of the problem is to determine the timing of surgery and the need for staging based on the condition of the surrounding soft tissues, with the presence of wrinkles in the soft tissue being the main sign of decreased inflammation.
External fixation can be used as a temporary treatment for staging tibial pilon fractures, as well as a method for definitive fixation. It is fundamentally based on the principle of ligamentotaxia to indirectly reduce the fracture by stressing the soft tissues surrounding the ankle [24].
External fixators
External fixation can be used as a temporary treatment for staging tibial pilon fractures, as well as a method for definitive fixation. It is fundamentally based on the principle of ligamentotaxia to indirectly reduce the fracture by stressing the soft tissues surrounding the ankle [24].
When used temporarily for staging, it is important to carefully place the pins outside the area of injury and the planned surgical site, in this way to reduce the risk of infection, as higher rates of infection have been reported when the definitive internal fixation was extended to the area of the provisional external fixator pins. The unacceptably high complication rate in the 1990s prompted the search for new definitive treatment methods.
External fixation as a definitive treatment
The unacceptably high complication rate in the 1990s prompted the search for new definitive treatment methods.
From there, external fixators were not only used as a temporary fixation device, especially in highly comminuted distal tibia fractures with maximum soft tissue damage, open Gustilo type III fractures, highly contaminated wounds, or significant patient comorbidities, open reduction and osteosynthesis is associated with a high risk of failure and complications. Therefore, external fixators may present a satisfactory alternative form of definitive treatment. External fixation methods can also be combined with limited internal fixation or minimally invasive techniques, such as percutaneous Kischner wires, to better reduce the joint surface area [25].
The most common complication associated with the use of external fixators in general is infection of the wire tract, which can also lead to major deep infections, namely septic arthritis and osteomyelitis.
A basic distinction can be made between ankle fixation and ankle extension systems. Ankle preservation systems are beneficial for functional outcome, as movement in the ankle is not restricted. In addition, it is possible to support the full weight, especially in hybrid systems [25].
Papadokostakis compared external ankle fixation systems and found no significant differences in infection rate, lack of union, and time to union, but systems seeking to perform ankle ligamentotaxia had a significantly higher incidence of malunion and functional outcome was also significantly lower compared to ankle preservation systems [26].
Multiple studies have compared the outcomes of treatment using external fixation and open reduction and osteosynthesis. The result appears to be similar in terms of early complications, but a significantly higher rate of superficial infection was observed, mainly due to wire tract infections in the external fixation; however, the rate of deep infections did not vary significantly. The rate of malunion was significantly higher in external fixation, which is probably due to the limited possibility of anatomical reduction with the use of external fixators [27].
Also, the functional outcome seems to be lower in treatments with external fixation than in open reduction and osteosynthesis, which is attributed to the lower possibility of anatomical reconstruction of the joint surface. However, studies showed that external fixation with fine wires and open reduction and osteosynthesis offer an equivalent functional outcome in highly comminuted and severely displaced pylon fractures.
The Ilizarov external fixation method presents new possibilities in external fixation treatment. The use of tensioned transfixiating wires offers the possibility of securely fixing small bone fragments and achieving stable bone reconstruction, while promoting bone consolidation as it allows axial micromovement based on relative biomechanical stability. Its circular configuration means that the ankle joint does not need to be pierced, which allows early mobility, improving blood flow to the injured cartilage. When there is significant bone loss, the Ilizarov fixation system can provide a valuable tool for distraction osteogenesis [26].
Hybrid fixator systems consist of at least three tensioned wires, which are placed in the distal fragments of the fracture site and connected through a circular frame (Figure 2). Mostly, hybrid external fixation systems can be used in the ankle ligamentotaxy technique, where it is possible to support the entire weight load [4].
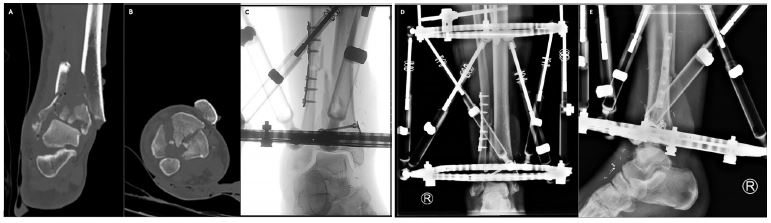
Figure 2: Primary hybrid external fixation in combination with plate osteosynthesis and lag screws in an open tibial pilon IIA fracture. We present the case of a 55-year-old man with an open fracture IIA of the tibial pylon AO type 43-C3, who came through the trauma room. After preoperative CT scans in the emergency [(A) coronal plane, (B) axial plane] temporary fixation and soft tissue conditioning were performed. The extensive soft tissue defect on the anteromedial side was covered with a microvascular radial artery free flap. Subsequently, the length and rotation of the fibula conminuto were restored and the articular surface of the tibial pylon was reconstructed using minimally invasive plates and lag screws, (C) intraoperative fluoroscopy]. Finally, we stabilized the tibial pilon fracture using a hybrid circular frame with Kichner wires tensioned in the distal fragments and Schanz screws in the proximal tibia, [(D) Postoperative AP radiograph, (E) Postoperative lateral radiograph.
Source: Mair O, Pflüger P, Hoffeld K, Braun K, Kirchhoff Ch, Biberthaler P, Crönlein M. Management of Pilon Fractures—Current Concepts. Front. Surg. 2021; 8:764232. doi: 10.3389/fsurg.2021.764232.
Source: Mair O, Pflüger P, Hoffeld K, Braun K, Kirchhoff Ch, Biberthaler P, Crönlein M. Management of Pilon Fractures—Current Concepts. Front. Surg. 2021; 8:764232. doi: 10.3389/fsurg.2021.764232.
The exact indication for external fixation methods as definitive primary treatment is mainly in tibial pilon fractures, where the risk of serious complications is elevated due to poor soft tissue coating, grade IIb, IIc, and III open fractures, or patients with severe comorbidities [24,27].
Open reduction and internal fixation
Currently, the mainstay of treatment for the vast majority of pylon fractures remains open reduction and internal fixation. This provides direct visualization for joint reduction and allows for direct reduction of the metadiaphyseal segment.
Proper reduction and fixation begin with a careful evaluation of the preoperative CT scan to determine the optimal approach and position of the material. While they share commonalities, each fracture should be approached as an individual entity and the surgical plan should be tailored to the particularities of each particular fracture. The main objectives are the anatomical reconstruction of the articular surface and the restoration of correct rotational alignment to achieve the best functional results [28].
Goals of surgical treatment
In 1979, Rüedi and Allgöwer proposed four sequential principles for the treatment of tibial pilon fractures. These principles include: [28]
1. Restoration of fibula length
2. Anatomical reduction of the joint surface
3. Filling of the residual bone defect with cancellous autograft
4. Stabilization of the medial spine.
Conceptually, these principles still apply, but they have evolved over time.
The three main columns, the anterolateral (Chaput), the posterolateral (Volkmann), and the medial column, should be evaluated consecutively. Therefore, the approaches chosen should allow direct visualization of the main fracture zone and joint block, while the soft tissues should be preserved as best as possible.
Surgical approaches
Numerous approaches have been described for the treatment of pylon fractures. Careful analysis of X-rays and preoperative CT scans are critical in deciding which approach to use. CT scans are also extremely useful for evaluating soft tissue structures that may become trapped in the fracture, particularly posteromedial structures, including the posterior tibial neurovascular bundle. Trapped structures are often overlooked by the radiologist, so the analysis should focus specifically on their location [4].
Approaches include anterolateral, anteromedial, direct anterior, direct lateral, direct medial, posterolateral, and posteromedial (Figure 3). All of these approaches have their own advantages and disadvantages. The anterior approaches allow direct visualization and reduction of joint fragments, while the posterior approaches are based on the indirect reduction of the joint surface by fluoroscopic imaging [4].
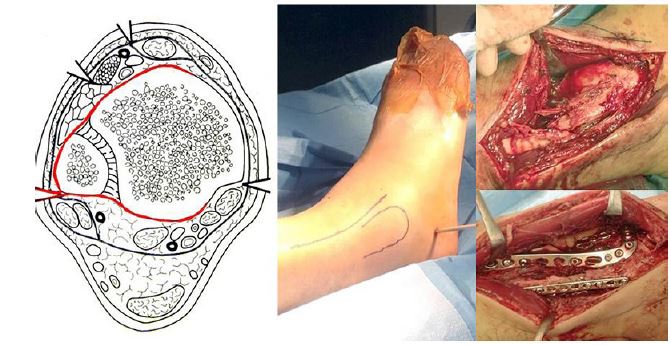
Figure 3: Several accesses can be used to approach the distal tibia. The red line in the image represents our preferred approach when access to the anterolateral and posterolateral aspects of the tibial ceiling is needed. An incision is made along the anterior border of the fibula, and both anterior and posterior dissection of the fibula is performed, providing access to the fibula and anterolateral tibia.
Source: Mair O, Pflüger P, Hoffeld K, Braun K, Kirchhoff Ch, Biberthaler P, Crönlein M. Management of Pilon Fractures—Current Concepts. Front. Surg. 2021; 8:764232. doi: 10.3389/fsurg.2021.764232.
Source: Mair O, Pflüger P, Hoffeld K, Braun K, Kirchhoff Ch, Biberthaler P, Crönlein M. Management of Pilon Fractures—Current Concepts. Front. Surg. 2021; 8:764232. doi: 10.3389/fsurg.2021.764232.
The incisions can be used alone or together, but they must be determined based on each patient’s individual fracture pattern. When using double incisions, surgeons advocated a minimum skin bridge of 7 cm between them; This minimizes the risk of soft tissue involvement and wound complications. However, this principle has recently been the subject of analysis. Howard demonstrated few soft tissue complications despite the fact that 83% of patients had skin bridges of less than 7 cm between the incisions. In small incisions, such as those used in minimally invasive techniques, the distance between the incisions can be even smaller. It is important to respect the soft tissue envelope with precise handling; Skin flaps should be full-thickness, regardless of the incisions used, and a meticulous soft tissue manipulation technique should be employed, with gentle retraction of the skin edges to prevent wound necrosis [4].
It is important to recognize that no one approach is the absolute choice for all patients. Surgeons treating these complex fractures should become familiar with the various approaches to the distal tibia and be prepared to use the appropriate approach depending on the condition of the soft tissues and the configuration of the fracture.
Perone longitude restoration
Metaphyseal comminution is common and can make it difficult to estimate tibial length. Often, the fibula has less comminution and a more precise reduction can be obtained. Stable fibula fixation provides lateral support and thus facilitates coronal and translational alignment [29].
Although recent studies have questioned the need for fibula fixation, what is clear is that fibula stabilization is imperative in the presence of a syndesmotic injury, as its ligamentous insertions are important for syndesmotic stability. The fibula is not only an important ankle stabilizer, ‘‘the ankle key’’ according to Weber, but also contributes to the reduction of the pylon. When properly reduced and fixed, the fibula acts as a strut and contributes to length, alignment, and translation. If the ligaments of the syndesmosis are intact, specifically the anterior inferior tibiofibular ligament and the posteroinferior tibiofibular ligament, fibula reduction may also contribute to the reduction of Volkmann and Chaput fragments [28,29].
The time of fibula fixation depends on when the surgery is performed, if it is performed in stages, some are the criterion that the fibula should be reduced and fixed initially, at the time of placing the external fixator. This provides greater stability to the structure while waiting for the soft tissues to improve and also reduces the operating time at the time of definitive fixation of the pylon. It is imperative to obtain an anatomical reduction of the fibula, as otherwise, a poor reduction may prevent an accurate reduction of the tibia, it is also important to carefully consider the incision to address the fibula, leaving a proper cutaneous bridge between additional incisions that may be needed. A posterolateral or lateral incision is usually used, depending on the access needed for the future approach to the pylon.
Other traumatologists, on the other hand, are of the opinion of not stabilizing the fibula until the moment of definitive fixation of the pylon.
Anatomical reduction of the joint surface
The AO principles establish the need for anatomical reduction and absolute stability of the joint surface in any intra-articular fracture. Restoring the joint surface is thought to decrease the risk of post-traumatic arthritis, ultimately leading to better outcomes [30].
The joint surface area should be reduced sequentially, usually starting from lateral to medial and from posterior to anterior. Often, the Volkmann fragment is first reduced and used as a stabilizer so that the rest of the joint block can be reduced around it. The reduction can be temporarily maintained using Kischner wires until the entire bonding block is congruent. Final reduction is possible using traction screws, small fragment screws, and anatomically molded compression plates, which can be locking or non-locking, with a low thickness to preserve the soft tissue as much as possible [30].
Fractures with valgus deformity often require an anterolateral neutralization plate, while varus deformities require medial neutralization. Placement of posterior plates to treat the posterior tibial spine and prevent tibial shortening should be achieved by posteromedial or posterolateral approaches.
In very comminuted fractures with multiple fragments, it may be necessary to address the fracture in conjunction with anterior and posterior approaches; very rarely doing two separate surgeries. Significant bone loss and comminution may require bone grafting from autologous or benched bone material. Bone transport may also present a viable option when using circular frames. Primary arthrodesis only serves as a salvage procedure in a very selected group of patients [30].
Use of cancellous graft for bone defects
Bone deficit often occurs after joint segment reduction due to the high energy associated with injuries and the significant impaction that often accompanies them. To support the joint segment and prevent its sinking, various methods have been used, such as autologous bone grafts, spongy and structural allografts, calcium-based cements and demineralized bone matrix products. Although each has its advantages and disadvantages, there is no evidence to demonstrate a clear advantage of one graft material over another [4].
Medial spine fixation
The original study by Ruedi and Allgower advocated independent fixation of the medial spine with a neutralization plate as the fixation pillar. In recent years, many surgeons have opted for anterolateral block plates instead of anterolateral block plates. However, a recent study with three commercially available plates of this type showed that the distal screw configuration frequently does not reach or adequately fix the medial major fragment. A thorough analysis of the preoperative CT scan should be done to determine the likelihood that anterolateral plate fixation will provide adequate fixation of the medial segment and consider additional medial fixation, either with a low-profile plate or with medial spine screws. It is often useful to place a medial plate subcutaneously through minimally invasive incisions to reinforce and correct any varus deformities [26-28].
Exposed fractures
Open fractures are common and should be treated initially with adequate surgical lavage and debridement, as well as early initiation of intravenous antibiotics. Thorough debridement with excision of nonviable bone is vital to creating an environment that promotes healing and decreases the risk of infection. However, care should be taken to preserve bone fragments containing joint surfaces. In high-energy fractures with significant comminution, contamination, or periosteal detachment, adequate debridement of nonviable bone may result in significant bone loss; If the wound can be closed primarily, it is critical that the skin is not sutured under tension [26].
Given the risk of infection, recent studies have evaluated the use of adjuvants in the context of these exposed fractures. In a pilot study conducted by O’Toole, preoperative supplemental oxygen was used in the context of exposed plateau, pilon, and calcaneal fractures. Vancomycin in local powder is also used during surgery to reduce infections [28].
Exposed fractures in this area usually require soft tissue flap coverage, and multiple studies have correlated early flap coverage with lower infection rates. Recently, a study of exposed tibia fractures showed that the time to flap coverage was an independent risk factor for complications, even controlling for the severity of the injury. While no increased risk was seen if coverage was done within the first 7 days, there was a significant increase in complication rates for each day after seven.
Conclusions
Tibial pilon fractures are rare, but they pose a major challenge for orthopedic surgeons. Preoperative evaluation and planning include X-rays and CT scans, as well as a thorough investigation of the patient’s history to identify potential risk factors, which is key to treatment success. The combination of articular cartilage injury, metaphyseal comminution, and soft tissue damage has often resulted in historically unfavorable outcomes.
Special consideration and care should be taken in the management of the soft tissues surrounding tibial pilon fractures. Choosing the right approach for each fracture pattern is important to get the best possible visualization and therefore be able to anatomically reduce the articular surface of the tibial pilon. Respecting the soft tissue envelope is the first step to minimizing complications.
Open reduction and internal fixation remain the mainstay of treatment for most of these fractures; Additional treatment modalities, such as external fixation and primary arthrodesis, are emerging and should be considered for more complex cases. While advances in surgical techniques and implants have improved outcomes over time, the overall prognosis for these injuries is often poor.
Recommendation
More research and innovation are needed to further improve outcomes and quality of life for patients affected by tibial pilon fractures.
References
- Murawski CD, Mittwede PN, Wawrose RA, Belayneh R, Tarkin IS. Management of high-energy tibial Pilon fractures. J BoneJoint Surg Am. 2023; 105: 1123-37.
- Coello García BE, Fernández Ordoñez DW, Iza Román AE, Loor Martínez LC, Ordóñez Ramos ML, Granizo Jara JL, et al. Fractures of the tibial pilon -horizontal articular surface of the tibia. EPRA International Journal of Multidisciplinary Research. 2023; 9: 14399.
- Hill DS, Davis JR. What is a tibial pilon fracture and how should they be acutely managed? A survey of consultant British Orthopaedic Foot and Ankle Society members and non-members. Ann R Coll Surg Engl. 2023.
- Mair O, Pflüger P, Hoffeld K, Braun KF, Kirchhoff C, Biberthaler P. Management of Pilon Fractures-Current Concepts. Frontiers in Surgery. 2021; 8: 764232.
- Rüedi TP, Allgöwer M. The operative treatment of intraarticular fractures of the lower end of the tibia. Clin Orthop Relat Res. 1979; 138: 105-10.
- Rüedi TP, Algower M: Fractures of the lower end of the tibia into the ankle joint: results after 9 years after open reduction and internal fixation. Injury. 1973; 5: 130.
- Rodriguez Castells F. Fracturas del pilón tibial. Rev. Asoc. Arg. Ortop. y Traumatol. 2020; 61: 312-21.
- Zelle BA, Dang KH, Ornell SS. High energy tibial pilon fractures: an instructional review. International Orthopaedics (SICOT). 2019; 43: 1939-50.
- Saad BN, Yingling JM, Liporace FA, Yoon RS. Pilon Fractures: Challenges and Solutions. Orthop Res Rev. 2019; 11: 149-57.
- Bear J, Rollick N, Helfet D. Evolution in Management of Tibial Pilon Fractures. Current Reviews in Musculoskeletal Medicine. 2018; 11: 537-45.
- Palma J, Villa A, Mery P, Abarca M, Mora A, Peña A. A new classification system for pilon fractures based on CT scan: An independent interobserver and intraobserver agreement evaluation. J Am Acad Orthop Surg. 2020; 28: 208-13.
- Rüedi TP, Allgower M: Fractures of the lower end of the tibia into the ankle joint. Injury. 1969; 1: 92-9.
- Topliss CJ, Jackson M, Atkins RM. Anatomy of pilon fractures ofthe distal tibia. J BoneJoint Surg Br. 2005; 87: 692-7.
- Leonetti D, Tigani D. Pilon fractures: A new classification system based on CT scan. Injury. 2017; 48: 2311-2317.
- Hebert-Davies J, Kleweno CP, Nork SE. Contemporary strategies in pilon fixation. J Orthop Trauma. 2020; 34: S14-20.
- Daniels NF, Lim JA, Thahir A, Krkovic M. Open pilon fracture postoperative outcomes with definitive surgical management options: a systematic review and meta-analysis. Arch Bone Joint Surg. 2021; 9: 272-82.
- Faber RM, ParryJA, Haidukewych GH, Koval KJ, Langford JL. Complications afterfibula intramedullarynail fixationof pilonversus ankle fractures. Journal of Clinical Orthopaedics and Trauma. 2020: 75-9.
- Bastias C, Lagos L. New Principles in Pilon Fracture Management: Revisiting Rüedi and Allgöwer Concepts. Foot Ankle Clin. 2020; 4: 505-21.
- Luo TD, Pilson H. Pilon Fracture. PubMed. Treasure Island (FL): StatPearls Publishing. 2022.
- Lineham B, Faraj A, Hammet F. Outcomes of Acute Ankle Distraction For Intra-Articular Distal Tibial And Pilon Fractures. Orthop Procs. 2024; 106-B: 11-11.
- Das M, Pandey S, Gupta H, Bidary S, Das A. Clinical characteristics andoutcome oftibial pilonfractures treated with open reduction and plating in a tertiary medical college. Journal of Gandaki Medical College. 2023: 16.
- Mogileesh M, Abdul A, Chetan C, Babu CS. Study of complex tibial Plafond Fractures treated by Delayed Single stageprocedure -prospective study. PARIPEX INDIAN JOURNAL OF RESEARCH. 2024: 29-31.
- Garay JCG, Mendoza KBT, Briones WJN, Mendoza JCP. Lesiones músculo tendinosas asociadas afracturas depilón tibial y complicaciones. Uct. 2019; 1: 8-8.
- Amigo Castañeda P, Rodríguez Díaz M, Reguera Rodríguez R. Evaluación de los resultadosen eltratamiento de los pacientes confracturas depilón tibial. RevMéd Electrón. 2021: 43.
- Legallois Y, Baudelle F, Lavignac P, Garcia M, Meynard P, Cadennes A.Tibial pilonfractures treatedwith a periarticular external fixator: Retrospective study of 47 cases. Orthop Traumatol Surg Res. 2022; 108: 103148.
- Mehta N, Graham S, Lal N, Wells L, Giotakis N, Nayagam S, Narayan B. Fine wire versus locking plate fixation of type C pilon fractures. Eur J Orthop Surg Traumatol. 2021.
- Vicenti G, Bizzoca D, Nappi VS, Carrozzo M, Delmedico M, Solarino G. The impact of lag screw in the healing time of distal tibia fractures treated with minimally invasive plate osteosynthesis: a randomized clinical trial. Injury. 2020; 51: S80–5.
- Giordano V, Boni G, Godoy-Santos AL, Pires RE, Fukuyama JM, Koch HA, Giannoudis PV. Nailing the fibula: alternative or standard treatment for lateral malleolar fracture fixation? a broken paradigm. Eur J Trauma Emerg Surg. 2020; 47: 1911-20.
- Kho DH, Cho BK, Choi SM. Midterm outcomes of unstable ankle fractures in young patients treated by closed reduction and fixation with an intramedullary fibular nail vs open reduction internal fixation using a lateral locking plate. Foot Ankle Int. 2021; 42: 1469-81.
- Gutiérrez Fernández F, López Angulo D, Ramírez Perera Sh. Fracturas de pilón tibial, clasificación y tratamiento. Revista Médica Sinergia. 2023; 8: e1070.
