
Open Access, Volume 11
Innovative surgery to facilitate early lung re-transplantation after pulmonary graft infarction
Vornicu Ovidiu1,3; Buche Michel2; Evrard Patrick1; Bughin François1; Eucher Philippe2; Collard Edith3; Marchand Eric4; Michaux Isabelle1; Bulpa Pierre1*
1Intensive Care Unit, Mont-Godinne University Hospital, CHU UCL Namur, Université Catholique de Louvain, Belgium.
2Department of Cardio-Thoracic Surgery, Mont-Godinne University Hospital, CHU UCL Namur, Université Catholique de Louvain, Belgium.
3Department of Anesthetic, Mont-Godinne University Hospital, CHU UCL Namur, Université Catholique de Louvain, Belgium.
4Department of Pulmonary, Mont-Godinne University Hospital, CHU UCL Namur, Université Catholique de Louvain, Belgium.
Bulpa Pierre
Intensive Care Unit, Mont-Godinne University Hospital, CHU UCL Namur, Avenue Thérasse, 1, 5530 Yvoir, Belgium.
Tel: +32-81-42-38-63, Fax: +32-81-42-38-62;
Email: pierre.bulpa@chuuclnamur.uclouvain.be
Received : May 10, 2025,
Accepted : June 03, 2025
Published : June 10, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Hemorrhagic pulmonary infarction secondary to venous thrombosis is a rare but life-threatening complication after lung transplantation. We describe the case of a 61-year-old man with very severe chronic obstructive pulmonary disease (COPD) who underwent single left lung transplantation. The early postoperative period was marked by pulmonary venous graft infarction, complicated by massive hemoptysis originating from the transplanted lung and hemorrhagic shock. To control the hemorrhage, urgent allograft pneumonectomy was required. However, to facilitate early re-transplantation, the vascular and bronchial stumps of the graft were preserved. A new pulmonary transplant was successfully performed six days later with no further complications.
Keywords: Lung transplantation; Urgent re-transplantation; Pulmonary graft infarction; Innovative surgery.
Abbreviations: COPD: Chronic Obstructive Pulmonary Disease; Peep: Positive End-Expiratory Pressure; ICU: Intensive Care Unit.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Pierre B (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Ovidiu V, Michel B, Patrick E, Francois B, Philippe E, Edith C, Pierre B, et al. Innovative surgery to facilitate early lung re-transplantation after pulmonary graft infarction. Open J Clin Med Case Rep. 2025; 2357.
Introduction
Lung transplantation is a recognized treatment option for several end-stage lung diseases. Although the procedure is well codified, early life-threatening complications still occur. Here we describe the case of a patient with hemorrhagic venous infarction after single lung transplantation.
Case Report
A 61-year-old man with very severe Chronic Obstructive Pulmonary Disease (COPD) (GOLD IV) had single left lung transplantation. The total ischemic time was 2 hours 51 min. At the end of the surgical procedure, there was sudden bleeding from the left atrium leading to severe hypotension requiring temporary vasopressor support. Prompt hemostasis was achieved by auricular suture stopping the hemorrhage. After stabilization, the patient was transferred to the Intensive Care Unit (ICU) and early evolution was uneventful.
Twelve hours after ICU admission, postoperative transesophageal echocardiography was performed as per-protocol and showed a hematoma compressing the left atrium, probably as a result of intraoperative hemorrhage, with abnormal flow in the left superior pulmonary vein. Also per-protocol, bedside lung scintigraphy showed no left pulmonary perfusion (Figure 1). Thirteen hours after ICU admission and within an hour after scintigraphy, the patient developed hemoptysis. Urgent fiberoptic bronchoscopy was performed and massive bleeding originating from the left lung was temporarily controlled by an angioplasty ballon (Fogarty®) introduced into the left lower bronchus. Despite this intervention, the patient developed hemorrhagic shock requiring urgent surgery. To prevent right lung flooding and avoid reintubation with a double lumen tube, we inserted an endobronchial blocker (ARNDT® Cook 7F) in the main left bronchus. The hemorrhage was controlled by clamping arterial and venous vessels. As the transplanted lung being completely filled with blood, graft pneumonectomy was the only therapeutic option. During the surgical procedure, a leak in the atrial cuff suture was identified and sutured. To facilitate the subsequent re-transplantation, arterial, venous, and bronchial anastomoses were preserved, as well as small allograft stumps; the vascular ones were sutured and the bronchial one occluded with a pericardial patch (Figure 2). Histology of the pneumonectomy tissue confirmed a hemorrhagic pulmonary infarction.
In the postoperative period, ventilation was changed to a pressure support mode, with pressures and Peep set as low as possible, to prevent high tracheal pressures and sedation was stopped to facilitate active mobilization. Immunosuppressive treatment was stopped but methylprednisolone was continued due to the presence of some allograft tissue.
Six days later, the patient underwent a further left lung transplant protected by extracorporeal membrane oxygenation. The allograft stumps were first resected together with a small juxta-anastomotic segment of the recipient’s pulmonary artery and bronchus with minimal loss of native tissue length. Thus, the length of the native stumps of the vessels and the bronchus was preserved, allowing the transplantation of the new lung without technical difficulty. The patient’s postoperative evolution was uneventful except for transient renal dysfunction and Enterobacter aerogenes bacteremia treated with appropriate antibiotics. Bedside pulmonary perfusion scintigraphy and transesophageal echocardiography confirmed normal left lung pulmonary flow. The patient was discharged from hospital 30 days after the re-transplant and regular follow-up showed normal graft function.
The patient died six years later from metastatic colon cancer.
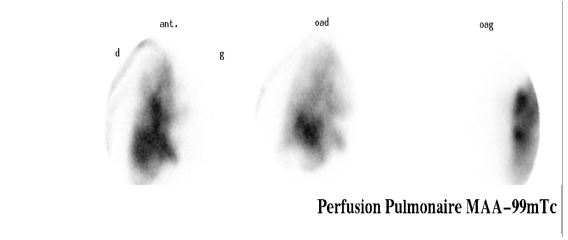
Figure 1: Lung perfusion scintigraphy showing the absence of left lung graft vascularization.
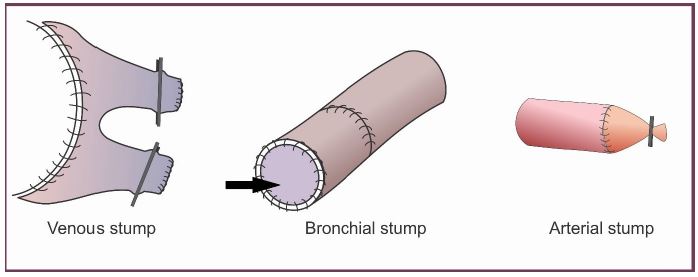
Figure 2: Schematic representation of the surgical technique used to preserve the recipient’s vascular and bronchial stumps. Arrow= pericardial patch.
Discussion
Anastomotic and non-anastomotic venous complications (kinking, twisting, external compression, thrombi) leading to pulmonary vein stenosis or complete obstruction occur in up to 15% of patients after lung transplantation and usually occur early (within 48 hours) [1]. The presentation of these complications is polymorphic and the signs are often misinterpreted as pulmonary edema or rejection. Such complications can range from a simple stenosis observed intraoperatively to a venous infarction complicated by hemorrhage.
Complete obstruction of a pulmonary vein leading to pulmonary infarction and hemodynamic instability has exceptionally been reported after lung transplantation, and systematically leads to death in the absence of an available graft [2].
Diagnosis of venous complications is mainly based on transesophageal echocardiography [3] but can also be made using chest CT angiography or lung perfusion scintigraphy [4]. If such complications are identified during surgery, prompt treatment is usually effective. However, when the diagnosis is delayed, there is no consensus regarding optimal management strategies. Various approaches, including thrombolysis and anticoagulants, revision surgery [5] (thrombectomy, anastomosis reconstruction or resection), and angioplasty and/or stenting [6,7] have been reported to be effective. Urgent pneumonectomy is sometimes needed for uncontrolled hemoptysis or pulmonary necrosis.
If a lung re-transplantation is considered, preserving the length of the recipient’s bronchial and arterial stumps appears important for at least two reasons. First, during the initial pulmonary transplantation the donor bronchi are trimmed as short as possible to minimize the risk of ischemia given their limited blood supply after transplantation. Second, the length of the pulmonary artery in donor lungs is frequently inadequate.
In the present case, the decision to preserve the initial sutures and leave small stumps of the graft in place helped preserve the length of both the recipient’s bronchus and pulmonary vessels. Accordingly, the arterial and bronchial anastomoses could be undone with minimal loss of recipient tissue at the time of re-transplantation.
To our knowledge, this ingenious solution, enabling us to safely wait for a new pulmonary graft and thus facilitating the second transplantation, has not previously been reported.
Conclusion
Although pulmonary infarction is rare after lung transplantation, it is a life-threatening complication especially when complicated by severe bleeding. To control the hemorrhage, sometimes the only therapeutic option is a pneumonectomy. However, to optimize the chances of successful re-transplantation, retaining vascular and bronchial allograft stumps and preserving the recipient’s main bronchus and vascular tissue must be considered at the time of pneumonectomy.
References
- Schulman LL, Anandarangam T, Leibowitz DW, Ditullio MR, McGregor CC, Galantowicz ME, et al. Four-year prospective study of pulmonary venous thrombosis after lung transplantation. J Am Soc Echocardiogr. 2001; 14: 806-812.
- Shah AS, Michler RE, Downey RJ, Leibowitz DW, Homma S, Smith CR. Management strategies for pulmonary vein thrombosis following single lung transplantation. J Card Surg. 1995; 10: 169-178.
- Cywinski JB, Wallace L, Parker BM. Pulmonary vein thrombosis after sequential double-lung transplantation. J Cardiothorac Vasc Anesth. 2005; 19: 225-227.
- Batra K, Chamarthy MR, Reddick M, Roda MS, Wait M, Kalva SP. Diagnosis and interventions of vascular complications in lung transplant. Cardiovasc Diagn Ther. 2018; 8: 378-386.
- Nagahiro I, Horton M, Wilson M, Bennetts J, Spratt P, Glanville AR. Pulmonary vein thrombosis treated successfully by thrombectomy after bilateral sequential lung transplantation: report of a case. Surg Today. 2003; 33: 282-284.
- Jing L, Chen W, Zhai Z, Pan X, Tao X, Cao L, et al. Pulmonary vein stenosis after lung transplantation: a case report and literature review. Ann Transl Med. 2021; 9: 181.
- Loyalka P, Cevik C, Nathan S, Gregoric ID, Kar B, Parulekar A, et al. Percutaneous stenting to treat pulmonary vein stenosis after single-lung transplantation. Tex Heart Inst J. 2012; 39: 560-564.
