
Open Access, Volume 11
Lung ultrasound in the early diagnosis of an unexpected neonatal pulmonary sequestration
Eugenia Maranella1*; Arianna Mareri1; Monica Sion2; Cecilia Di Natale1; Veronica Pannone1; Ludovica Di Francesco1; Sandra Di Fabio1
1Neonatology and Neonatal Intensive Care Unit, San Salvatore Hospital, L’Aquila, Italy.
2Radiology Unit, University of L’Aquila, Italy.
Eugenia Maranella
Neonatology and Neonatal Intensive Care Unit, San Salvatore Hospital L’Aquila, Italy.
Email: eugenia.maranella@gmail.com
Received : May 05, 2025,
Accepted : May 28, 2025
Published : June 10, 2025,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Maranella E (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Maranella E, Mareri A, Sion M, Di Natale C, Pannone V, Di Francesco L, Di Fabio S. Lung ultrasound in the early diagnosis of an unexpected neonatal pulmonary sequestration. Open J Clin Med Case Rep. 2025; 2355.
Short Report
E.J. term newborn born by C-section due to maternal hypertension and obesity. At 6 hrs of life the newborn was referred to our NICU for transient neonatal tachypnoea needed nCPAP for at least 24 hrs with rapid improvement in respiratory dynamics and oxygenation. During the first days of life the patient developed feeding intolerance. Due to recurrent vomiting and familiar hystory of multicystic displasic kidney we perfomed abdominal ultrasound: no abdominal malformations were found but an incidental finding of bilateral pleural effusion was detected. Chest x Ray confirmed the minimal pleural effusion without other patological signs. To monitor lung parenchima, serial lung ultrasounds were performed. LUS revealed a progressive reduction in pleural effusion but surprisingly a portion of consolidation area in the left basal lobe, suspected for pulmonary sequestration, was detected (Figure 1).
Due to the good clinical conditions, we started a LUS follow-up. At one month of life a CT scan confirmed the pulmonary malformation: an extralobar pulmonary sequestration with abnormal vessel from the thoracic aorta and venous drainage in azygos and emiazygos veins was identified in the lower pulmonary left lobe (Figure 2).
The newborns remain asynmptomatic no respiratory distress neither other symptoms were identified. We referred the patient to a neonatal surgical department, an early intralobar lung resection was performed without postoperative complications. Post-surgical follow-up has been good and serial LUS imaging were started.
Follow up at 9 months of life showed regular growth and neurodevelopment, no others respiratory symptoms neither pulmonary infections appeared during this period.
Lung ultrasound is a new and promising bedside monitoring. Do to non-invasive and easy approach, its use in the NICU is increased during diagnosis, follow up and treatment options (LUS score) in many lung diseases such as pneumothorax and respiratory distress syndorme. No data was reported about ultrasound imaging in pulmonary sequestration during the neonatal period. Our case is an early incidental diagnosis of unexpected extra lobar lung sequestration (ELS). Pulmonary sequestration is a rare congenital disease that comprises a non- functioning mass of pulmonary tissue separated from the bronchopulmonary tree. It receives blood supply from the systemic circulation with or without a separate venous drainage. It comprises from 0.15 to 6.4% of all congenital lung malformations [1]. Intralobar Sequestration (ILS) is abnormal lung tissue surrounded by normal lung pleura, while ELS has its own separate pleura. ELS is less common than the ILS and comprises approximately 25% of all sequestrations. They are predominantly featured in males (4:1), left-sided (65%), and are often associated with other congenital malformations (65%) [2]. It account for 23% of pulmonary anomalies diagnosed in utero [1]. While approximately 70% of congenital lung malformations are detected during fetal life [3], only 10% of ELS are detected incidentally in asymptomatic adults [4]. More of the 60% of ELS manifest clinically within the first six months of life, as respiratory distress, feeding intolerance, malabsorbotion and occasionally pulmonary or pleural haemorrage [1]. Early surgical approach is reccomended to reduce pulmonary complications [5].
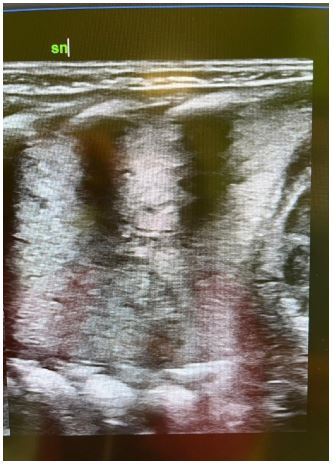
Figure 1: LUS imaging: using a micro-linear ‘hockey-stick’ probe, in the left basal lobe is identified a portion of large consolidation area, suspected for pulmonary sequestration.
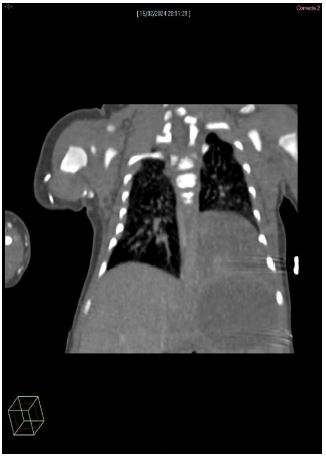
Figure 2: CT scan: At the left basal lobe, a triangular parenchymal consolidation area without continuity with the tracheobronchial tree or the main pulmonary arterial and venous structures. After contrast administration, the venous drainage is identified in the azygos-hemiazygos venous system and arterial vascularization is ensured by a small vessel originating from the descending thoracic aorta.
We would like to highlight the role of lung ultrasound in the early diagnosis and follow up of a perinatal pulmonary sequestration. The widespread use of LUS in the NICU, also in not common lung disease, may allow to delay and customise the use of invasive CT scans in diagnosis, in therapeutic decisions and in follow- up, reducing the cumulative radiation exposure in tiny and susceptible patients.
References
- Cong CV, Ly TT, Duc NM. Intralobar pulmonary sequestration supplied by vessel from the inferior vena cava: literature overview and case report. Radiol Case Rep. 2022; 17: 1345-1353.
- Brown EG, Marr C, Farmer DL. Extralobar pulmonary sequestration: the importance of intraoperative vigilance. Journal of Pediatric Surgery Case Reports. 2013; 1: 74-76.
- Kunisaky SM, Saito JM, Fallat ME, et al Fetal risk stratification and outcome in children with prenatally diagnosed lung malformations: results from a multi-institutional research collaborative. Ann Surg. 2022; 276: e622-e630.
- Walker CM, Wu CC, Gilman MD, et al The imaging spectrum of broncopulmonary sequestration. Curr Probl Diagn Radiol. 2014; 43: 100-114.
- Marinucci B, Maurizi G, Vanni C, et al Surgical tretment of pulmonary sequestration in adults and children: longt term results. Interactive cardiovascular and thoracic surgery. 2020; 31: 71-77.
