
Open Access, Volume 11
Pattern of distal femur intra-articular fractures and the functional outcome among patients treated with plates and screws at Kilimanjaro Christian medical centre
Denis Nkonge Mbae*; Cuthbert Kawa; Godfrey Lwanyaga; Paul Mwanemile; Godlisten Kawiche; Regnald Shoo; Faiton N Mandari
Kilimanjaro Christian Medical Centre & Kilimanjaro Christian Medical University College, Moshi Tanzania.
Denis Nkonge Mbae
Kilimanjaro Christian Medical Centre & Kilimanjaro Christian Medical University College, Moshi, Tanzania.
Email: denismbae89@gmail.com
Received : April 02, 2025,
Accepted : May 12, 2025
Published : May 15, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Background: Distal femur fractures, particularly those with intraarticular extension, present significant challenges in achieving optimal functional outcomes due to the complexity of the femoral anatomy and the knee joint’s critical role in mobility. The primary goal of treatment is not only to achieve bone healing but also to restore knee function. Despite advances in surgical techniques, particularly the use of internal fixation with plates and screws, complications arose, affecting the functional outcomes. Yet, less is known about long-term functional outcomes and their predictors.
Objective: To assess the pattern and long-term functional outcome of patients with intraarticular distal femur fracture treated by plates at KCMC Hospital from April 2022 to July 2023.
Methods: This was a hospital-based prospective study among patients with intraarticular distal femur fracture treated with plates and screws at KCMC between April 2022 to July 2023. Participants treated with plates and screws at KCMC between April 2022 to July 2023 and met the inclusion criteria were contacted and made an appointment to come to the orthopaedics clinic for assessment of functional outcome. Neers Knee Scoring System assessed functional outcome. SPSS version 25 was used for data analysis.
Results: A total of 59 participants were included in this study, all diagnosed with intraarticular fractures of the distal femur. Majority of them had 33C3 15(25.4%) followed by 33B2 13(22.0%), 33B1 11(18.6%), 33C1 9(15.3%), 33C2 8(13.6%) and 33B3 3(5.1%). Neers Knee Society Score, had a median (IQR) of 85.0(76.0–93.0). Majority of participants had an excellent score (> 85) 28(47.4%), and good score (70–85) 25(42.4%). 4(6.8%) had a fair score (55–69) and 2(3.4%) had a poor score. Age (p=0.046), type of distal femur fracture (p=0.032), and time from injury to surgery (p=0.021) were found to have a significant influence on functional outcome.
Conclusions: Motor traffic crash commonly causes intraarticular distal femur fractures, notably AO Classification type 33C3. Favorable outcomes correlate with age <40, AO type 33B fractures, and early surgical intervention within 14 days.
Keywords: Pattern; Distal femur intra-articular fractures; Functional outcome; Plates and screws.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Nkonge Mbae D (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Nkonge Mbae D, Kawa C, Lwanyaga G, Mwanemile P, Kawiche G, Shoo R, Mandari FN. Pattern of distal femur intra-articular fractures and the functional outcome among patients treated with plates and screws at Kilimanjaro Christian medical centre. Open J Clin Med Case Rep. 2025; 2352.
Introduction
Musculoskeletal (MSK) injuries are the major public health issue worldwide. In general, it is estimated to cause more death and Disability-Adjusted Life Years (DALYs) than HIV/AIDS, TB, and malaria combined [1]. Distal femur is a part of musculoskeletal system known with a complex anatomical structure, with the condyles forming the articular surface of the knee joint. This intricate architecture plays a crucial role in weight distribution, stability, and knee range of motion. Intraarticular fractures disrupt this delicate balance. Distal femoral fractures are defined as fractures up to 15 cm from the distal femoral articular surface [2].
Distal femoral fracture incidence is about 4-7% among all femur fractures [3]. Intra-articular fractures can pose greater treatment challenges due to their impact on the bone’s cartilage surface [4]. Most distal femur fractures result from severe axial load with either varus, valgus, rotational or, most frequently, a combination of these forces. There is a bimodal distribution of these fractures based on age and gender. High-energy distal femur fractures occur in young adults due to motor traffic crash, whereas low-energy fractures occur in the elderly due to simple falls [5-7].
Radiographs of the entire extremity, including the joints proximal and distal to the suspected injury, should be obtained when patients are hemodynamically stable to characterize the injury. Routine X-ray evaluation includes Standard AP and Lateral views and is considered the baseline investigation. Traction views can help characterize the fracture pattern; however, this is very painful for the patient, and pain control is necessary before any manipulation. Contralateral femur films may be considered for pre-operative planning and templating. CT scan is the gold standard that evaluates the intra-articular involvement and aid in preoperative planning [8].
With the increased incidence of high-energy trauma, especially those caused by Motor traffic crush, the occurrence of these difficult-to-treat fractures has increased. Hence there is a growing need for effective management of these injuries. In Tanzania, 59% of all femur fractures were caused by Motor traffic crash [9]. Effective management and timely interventions are essential to minimize the social and economic impact of these injuries, ensuring continued productivity and sports participation [4]. This led to the quest for better surgical techniques which could allow early mobilization of the patient. However, it was observed that some of participants with distal femoral fracture ended up with some disabilities that affected their socio-economical welfare. Long-term disability can occur in patients with extensive articular cartilage damage and marked comminution. Fracture shortening with extension and varus deformities of the distal articular surface is a typical presentation [8].
In developing countries like Tanzania, motorcycle transport is a vital source of income for many young individuals. This sector is prominently linked to a high incidence of motor traffic crash. These accidents often lead to specific injuries, notably distal femur fractures with intraarticular extension. The management of distal femur fractures with intraarticular extension at KCMC Hospital typically involves the use of plates and screws, yet comprehensive data on the functional outcomes of this approach remains limited. This study aims to address this gap by providing crucial insights into the effectiveness of plates and screws in promoting functional recovery post-fracture.
Material and Methods
Study design, area and population
This was a hospital based prospective study involving all adult patients with intraarticular fracture of the distal femur who were managed with plates and screws at KCMC hospital, orthopedics department from April 2022 to July 2023. All patients diagnosed with intra-articular distal femur fractures classified as type 33B and 33C according to the AO classification, who underwent treatment with plates and screws between April 2022 and July 2023 were included. Patients with previous injury or deformity on the same knee, patients with Ipsilateral tibia plateau fracture and polytrauma patients and Patients who did not consent to the study participation were excluded.
Sample size and sampling technique
The sample size was determined by using a Cochran formula for estimation of single population proportion with the assumption of 95% confidence level, an error margin of 5%, statistical correspondence to the level of significance of 1.96 and the prevalence of 3.84% [11]. The minimum sample size was 56 participants. Due to low prevalence, convenient sampling technique was used. All patients with intraarticular distal femur fractures who were treated with plates and screws between April 2022 and July 2023 were enrolled after meeting the inclusion criteria.
Study variables
Dependent variable was functional outcome. This was defined as the patient’s physical ability or recovery to the pre-injury activity level measured after one year. Based on four parameters (pain, stability, knee range of motion, and ability to perform routine daily activities) after internal fixation, the outcome could be excellent, good, fair, or poor. Independent variables were; socio-demographic characteristics, mechanism of injury, type 33B and 33C fracture distal femur and side of injury.
Data collection tools and procedure
A standard structured questionnaire translated into Swahili was used to collect patient information. The questionnaire consisted of socio-demographic information, the cause of injury, the mechanism of injury, the side of the injury, the type of fracture, and the functional outcome assessed by the Neers Knee Score System. This tool is valid and reliable in assessing functional outcomes after distal femur with intraarticular extension surgery [12]. Pain was assessed using a visual analogue pain scale. It has a numerical scale (0-10), and no pain is classified as 0, mild pain 1-3, moderate to severe pain 4-6, very severe pain 7-9, and worst pain possible 10 [13].
Participants with complete information from April 2022 to July 2023 and with eligible criteria were contacted about their participation in the study and given an appointment. Written informed consent was obtained from all participants before enrollment into the study. EHMS files contained information on the duration of the injury to surgery, age, gender, and postoperative physiotherapy participation. Participants completed a questionnaire followed by a physical examination on a bed.
X-ray images were generated and reviewed by both radiologist and researcher to classify patterns of intraarticular distal femur fractures based on the AO classification system. Functional outcome was evaluated using Neers knee Scoring System which consisted of two main grading components: functional and anatomical assessments. The functional aspect of the Neers knee Scoring System evaluated several parameters critical to assessing post-operative recovery. These included the severity of pain experienced by patients, their capacity for walking, the range of motion in both flexion and extension measured in degrees using a goniometer, and their capability to perform work-related activities.
Pain severity was assessed using a visual analogue scale, categorizing pain into distinct levels, including mild, moderate, severe, very severe, and worst possible pain. Active Range of motion was measured using a goniometer from 0 to 135 degrees to evaluate flexion and extension movements. In gross anatomy, the Limb was measured using a tape measure while the patient was lying supine on a bed, from the anterior superior iliac spine to the middle malleolus to see if there was any discrepancy; radiological grading was made based on varus or valgus deformity and union of the fracture. Functional outcomes scores, according to the Neers knee Scoring System, were categorized as excellent (<85 points), good (70-85 points), fair (55-69 points), or poor (<55 points).
Data processing and analysis
Information from the completed questionnaire was analyzed using SPSS version 25. It was entered into the database and cleaned in terms of consistency, checking for outliers and lost data. Patients’ data was only accessible to trained research assistants and principal investigator. Data for categorical variables was condensed via proportions, frequencies, and percentages. Calculations for median and inter-quartile range were done depending on the distribution of data. Fisher’s exact test was used to establish a relationship and comparison between functional outcome score, pattern of fractures and set of explanatory variables. Those with a p-value less than 0.05 were considered statistically significant.
Ethical consideration
Permission to conduct this study was obtained from the KCMUCo research ethical committee with number PG 70/2023. Permission to conduct this study at KCMC Hospital was obtained from the head of the Orthopedic department and the Director of hospital services at KCMC Hospital. Written informed consent was obtained from all patients’ prior data collection. All basic principle of ethics was observed.
Results
Enrollment of the study participants
A total of 316 distal femur fracture were recorded from April 2022 to July 2023. Among them, 238 had distal femur fracture type A and were excluded. From the remaining 78 participants, 12 had type B and C but treated with other methods such as Orif with s-nail/conservative. 66 patients were treated with plates and screws, however 4 had incomplete data. From 62 participants with complete data, only 59 consented to participate in the study (Figure 1).
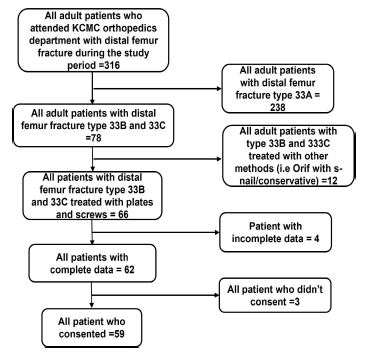
Figure 1: Flowchart showing the selection of study participants.
Characteristics of the study participants
This study included a total of 59 study participants. The median (IQR) age of the study participants was 33.0(26.0–41.0) years. Large proportion of the study participants; 21(35.6%) had a range of 21-40 years of age. Majority of the study participants were males 40(67.8%), and most were residing in Kilimanjaro region 52(88.2%) (Table 1).
Table 1: Socio-demographic characteristics of the study participants (n=59).
| Variable | n (%) | |
|---|---|---|
| Age (years) | ≤ 20 | 4(6.8) |
| 21-30 | 21(35.6) | |
| 31-40 | 17(28.8) | |
| >40 | 17(28.8) | |
| Median (IQR) | 33.0(26.0–41.0) | |
| Sex | Male | 40(67.8) |
| Female | 19(32.2) | |
| Residence | Kilimanjaro | 52(88.2) |
| Otherregions | 7(11.8) |
The pattern of distal femur fractures with intra-articular extension treated by plates and screws
From 59 participants with distal femur fractures with intra-articular extension treated with plates and screws, majority of them had 33C3 15(25.4%) followed by 33B2 13(22.0%), 33B1 11(18.6%), 33C1 9(15.3%), 33C2 8(13.6%) and 33B3 3(5.1%) (Figure 2). Motor traffic crash was the main cause of fractures 48(81.4%) while only 11(18.6%) originated from fall from the height. In general majority of the distal femur fractures patterns were due to Motor traffic crash (Table 2).
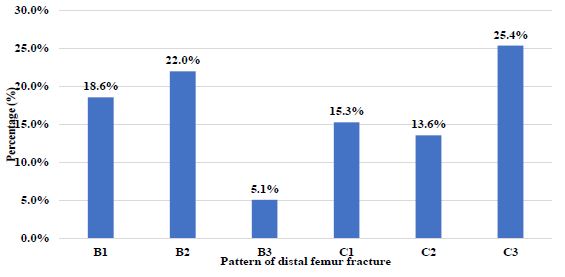
Figure 2: AO classification of distal femur fractures with intra-articular extension treated with plates and screws (n=59).
Table 2: The pattern of distal femur fractures with intraarticular extension.
| Pattern distalfemur fracture | |||||||
|---|---|---|---|---|---|---|---|
| 33B1 | 33B2 | 33B3 | 33C1 | 33C2 | 33C3 | ||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | Total | |
| 11 (18.6) | 13 (22.0) | 3 (5.1) | 9 (15.3) | 8 (13.6) | 15 (25.4) | n (%) | |
| Injury mechanism | |||||||
| MTC | 6 (54.5) | 9 (69.2) | 2 (66.7) | 9 (100.0) | 7 (87.5) | 15 (100.0) | 48 (81.4) |
| FFH | 5 (45.5) | 4 (30.8) | 1 (33.3) | 0 (0.0) | 1 (12.5) | 0 (0.0) | 11 (18.6) |
MTC: Motor traffic crash; FFH: Fall from Height.
The functional outcome of patients with distal femur fractures with intra-articular extension treated by plates and screws
The median (IQR) of the functional outcome of the distal femur fractures by using the Neer’s knee society score was 85.0(76.0–93.0). However; majority of the study participants; 28(47.4%) had excellent (>85) functional outcome score followed by 25(42.4%) who had good (70–85), 4(6.8%) had fair (55–69) and 2(3.4%) had poor functional outcome score (Figure 2).
Factors influencing the functional outcome of distal femur fractures with intra-articular extension treated by plates and screws
Different factors were compared to the functional outcomes using Fisher’s exact test. Factors such as age (p=0.046), type of distal femur fracture (p=0.032) and time from injury to surgery (p=0.021) significantly influenced functional outcome score (Table 3). A significant number of individuals operated within 14 days had excellent outcome 25(89.3%). Regarding types of fractures, participants with type 33C2 and 33C3 had poor outcome 1(50%) in both cases. Similarly for the participants aged 31-40 years old 2(100%) (Table 3).
Figure 3: The functional outcome of patients with distal femur fractures with intra-articular extension treated with plates and screws (n=59).
Table 3: Factors influencing the functional outcome of distal femur fractures with intra-articular extension treated by plates and screws (n=59).
| Functional outcome | |||||||
|---|---|---|---|---|---|---|---|
| Poor (<55) | Fair (55 - 69) | Good (70 - 85) | Excellent (>85) | ||||
| n (%) | n (%) | n (%) | n (%) | Total | |||
| Factors | 2 (3.4) | 4 (6.8) | 25 (42.4) | 28 (47.4) | n (%) | p value | |
| Age (years) | 18- 20 | 0 (0.0) | 0 (0.0) | 1 (4.0) | 3 (10.7) | 4 (6.8) | |
| 21 - 30 | 0 (0.0) | 0 (0.0) | 6 (24.0) | 15 (53.6) | 21 (35.6) | ||
| 31 - 40 | 2 (100.0) | 1 (25.0) | 8 (32.0) | 6 (21.4) | 17 (28.8) | ||
| > 40 | 0 (0.0) | 3 (75.0) | 10 (40.0) | 4 (14.3) | 17 (28.8) | 0.046 | |
| Sex | Male | 0 (0.0) | 3 (75.0) | 16 (64.0) | 21 (75.0) | 40 (67.8) | |
| Female | 2 (100.0) | 1 (25.0) | 9 (36.0) | 7 (25.0) | 19 (32.2) | 0.499 | |
| Injured side | Right | 2 (100.0) | 3 (75.0) | 18 (72.0) | 16 (57.1) | 39 (66.1) | |
| Left | 0 (0.0) | 1 (25.0) | 7 (28.0) | 12 (42.9) | 20 (33.9) | 0.751 | |
| Injury mechanism | MTC | 2 (100.0) | 2 (50.0) | 20 (80.0) | 24 (85.7) | 48 (81.4) | |
| FFH | 0 (0.0) | 2 (50.0) | 5 (20.0) | 4 (14.3) | 11 (18.6) | 0.312 | |
| Typeof distal femur fracture | |||||||
| 33B1 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 11 (39.3) | 11 (18.6) | ||
| 33B2 | 0 (0.0) | 0 (0.0) | 4 (16.0) | 9 (32.1) | 13 (22.0) | ||
| 33B3 | 0 (0.0) | 0 (0.0) | 1 (4.0) | 2 (7.1) | 3 (5.1) | ||
| 33C1 | 0 (0.0) | 0 (0.0) | 6 (24.0) | 3 (10.7) | 9 (15.3) | ||
| 33C2 | 1 (50.0) | 1 (25.0) | 5 (20.0) | 1 (3.6) | 8 (13.6) | ||
| 33C3 | 1 (50.0) | 3 (75.0) | 9 (36.0) | 2 (7.1) | 15 (25.4) | 0.032 | |
| Time of injury to surgery (days) | |||||||
| ≤14 | 0 (0.0) | 1 (25.0) | 18 (72.0) | 25(89.3%) | 44 (74.6) | ||
| >14 | 2 (100.0) | 3 (75.0) | 7 (28.0) | 3 (10.7) | 15 (25.4) | 0.021 | |
Discussion
This study was carried out to evaluate the pattern and functional outcome of intra-articular distal end femur fractures treated with plates and screws. The fractures were classified according to the AO/OTA classification. Functional outcome in patients were assessed using the Neer’s knee score at 1 year. The study involved 59 patients who presented at our hospital with intra-articular fractures of the distal femur. These fractures were treated using plates and screws, and all participants provided informed consent to take part in the study. The median age of 33.0 years (IQR: 26.0 - 41.0) predominated, with 21 participants (35.6%) aged between 21 to 40 years. The majority were male (67.8%). Functional outcomes, assessed by the Neers Knee Society Score, showed a median score of 85.0 (IQR: 76.0-93.0), with 28 participants (47.4%) achieving an excellent score (<85), 25(42.4%) had a good score (70-85), 4(6.8%) a fair score (55-69), and 2(3.4%) a poor score (>55). Factors significantly influencing outcomes included age (p=0.046), type of fracture (p=0.032), and time from injury to surgery (p=0.021).
In this study, the distribution of fracture patterns among participants was categorized according to the AO classification system. The most frequent type observed was 33C3, comprising 315(25.4%) of cases, followed by 33B2 at 13(22.0%), 333B1 at 11(18.6%), 33C1 at 9(15.3%), 33C2 at 8(13.6%), and 33B3 at 3(5.1%). Overall, fractures classified as type 33B accounted for 45.7% of cases, while type 33C fractures constituted 54.3%. The primary mechanism of injury identified in this study was Motor Traffic Crash (MTC), affecting 48(81.4%) of participants, with falls from height (FFH) accounting for 11(18.6%). These findings are in line with the studies conducted in India and Iran [12,14,15].
These studies, in general, reported similar patterns, with the predominant causes of these fractures being traffic accidents and accidental falls. Overall, these findings in patterns highlight the high prevalence of type 33C fracture and the dominant role of MTCs as a cause of such injuries in these studies. They suggest consistent patterns across different geographic locations in terms of injury mechanisms and fracture characteristics. This may be due to rapid industrialization with the increased use of motorcycles and vehicles as a mode of transport. A different finding was observed in a study in Nigeria assessing locking compression plate in distal intraarticular femoral fractures, where it was observed that Type 33B fractures were predominant [16]. The observed variability across the studies can be attributed to differences in sample characteristics. The initial study adopted a hospital-based prospective approach and included a larger sample size, whereas the Nigerian study, also prospective in design, was conducted with a smaller sample size.
Regarding the functional outcome, results revealed that 47.7% of cases (28 out of 59) achieved Neer’s scores of 85 or higher, indicating excellent outcomes. A further 42.4% (25 cases) attained scores in the range of 75-85, denoting good outcomes. Conversely, 6.8% (4 cases) were classified as having fair outcomes with scores falling between 55-74. Notably, only two cases (3.4%) received a score below 55, categorized as a poor outcome. Similarly, studies conducted India and Nigeria also showed less number of participants with poor functional outcomes with prevalence range 0.0%-4% [4,11,16]. Consistence in findings with other studies shows that, plates and screws used in treating intraarticular distal fractures consistently achieve favorable outcomes, as demonstrated by significant proportions of patients attaining excellent or good scores according to Neer’s criteria in the studies above. The low incidence of fair and poor outcomes underscores the reliability and effectiveness of this treatment approach in promoting functional recovery and patient satisfaction.
For the factors influencing functional outcome, age distribution revealed a peak incidence among individuals aged 21 to 30 years, comprising 35.6% of the total sample, equivalent to 21 patients. Following closely, the age group of 31 to 40 years accounted for 28.8% of cases, representing 17 patients. These findings highlight a notable concentration of cases among younger adults, with the difference being statistically significant (P=0.094). The differences in outcomes across age groups may stem from various factors. Younger individuals, who were the majority in this study, typically recover better due to faster tissue healing, higher physical activity, and fewer chronic conditions. As age increases, the body’s healing ability declines, leading to poorer functional outcomes, and older patients may also face additional health issues that hinder recovery.
In contrast, cross-sectional studies conducted in India and the Netherlands, age was observed to correlate with functional outcomes. The study populations in both countries predominantly included older patients, with mean ages of 45.78 years and 45 years, respectively. However, these associations were not found to be statistically significant (p=0.094 and p=0.58, respectively). Both studies employed similar methodologies but were limited by small sample sizes. The research concluded that advanced age was associated with poorer outcomes, potentially influenced by factors such as osteoporosis and prolonged hospitalization within this demographic (Saini, Shah, & Sharma, 2018) [17].
This study investigates the influence of fracture type on functional outcomes in patients. The distribution of fracture types was as follows: Type 33B1 accounted for 18.6%, Type 33B2 for 22%, Type 33B3 for 5.1%, Type 33C1 for 15.3%, Type 33C2 for 13%, and Type 33C3 for 25.4%. Notably, complicated fractures (Type 33C), which involve more comminution, made up 54.3% of the cases. Patients with these complicated fractures showed poorer or fair outcomes compared to those with less complicated fractures. The difference in outcomes was statistically significant. In contrast to these findings, study conducted in the Netherlands found no significant difference in outcomes between Type 33B and Type 33C fractures [17]. Similarly, another study from United State demonstrated no statistically significant findings between fracture type and outcome, mostly due to study’s multicenter design, large sample size, and the substantial number of patients presenting with Gustilo-Anderson type III open injuries [18]. The discrepancies in outcomes may be attributed to variations in healthcare systems, patient management protocols, and the specific characteristics of the patient populations. The results of this study align with those of a similar study conducted in India, which, although based on a smaller sample size, excluded all cases of open fractures. However, the Indian study utilized a cross-sectional design, whereas the current study employed a prospective design [4].
In the present study, 74.6% of all patients who underwent surgery within the first two weeks post-injury experienced favorable outcomes, a result that was statistically significant. These findings are consistent with a study conducted in Ivory Coast, which demonstrated that patients operated on within one week had a satisfactory outcome rate of 88.9%, compared to a 33.3% satisfactory outcome rate for those who underwent surgery after two weeks [19]. Both studies suggest that early surgical intervention is a critical factor in achieving optimal functional outcomes.
Conclusion
In conclusion, the study underscores motor traffic crash as the predominant etiology of intraarticular distal femur fractures, with AO Classification type 33C3 being the most frequently observed subtype. The functional outcomes of patients with intraarticular distal femur fractures after treatment with plates and screws, were predominantly favorable, with a significant majority achieving good to excellent results. Younger age (under 40 years), fractures categorized as type 33B according to the AO classification, and prompt surgical intervention (within 14 days) were found to influence functional outcomes positively.
Recommendation
Further studies should be conducted on the clinical management, surgical approaches, and rehabilitation outcomes specific to AO Classification type 33C3 fractures, as this subtype is most commonly observed in the study. Timely surgical intervention is strongly recommended to optimize good functional outcomes following intraarticular distal femur fractures.
Declarations
Authors contribution: Denis Mbae: He developed the research title, proposal, data collection and analysis, and manuscript for publication. Faiton Mandari and Regnald Shoo were the main supervisors who oversaw this research work at every step. Godlisten Kawiche, Cuthbert Kawa, Paul Mwanemile, and Godfrey Lwanyaga were consulted for their expert contributions.
Acknowledgement: I am profoundly grateful to God for His presence and guidance throughout my dissertation preparation journey. His steadfast support has been invaluable.
I extend heartfelt thanks to my parents, my father, Mr. Lucas Mbae and my mother, Caroline Mkwamugo Wallace, for their unwavering support and encouragement during the dissertation writing process. Their belief in me and their constant courage were instrumental in achieving this milestone.
I want to express my special gratitude to my supervisor, Dr. Faiton N. Mandari, and my co-supervisor, Dr. Regnald Shoo, as well as to all the specialists from the Department of Orthopaedic and Traumatology. Their support, guidance, and invaluable advice were essential in shaping this dissertation.
Finally, I would like to thank my fellow residents in the Orthopaedic and Traumatology department for their moral support and insightful contributions, as well as everyone else who played a part in making this dissertation a reality.
References
- Institute for Health Metrics and Evaluation (IHME). GBD compare. 2016.
- Agunda M, Gakuu LN, Museve gk. early functional outcome of distal femoral fractures at Kenyatta National Hospital and Kikuyu Hospital. East African Orthop J. 2013; 7: 57–63.
- Borthakur B, Hanse B, Haque R, Jindal S, Talukdar M. Orthopaedic Thesis Journal of Medical Thesis. 2016; 4: 31-36 Results of Locking Compression Plate fixation in Distal Femur Fractures: A Prospective Study. 2016; 4: 31–6.
- Saini DRA, Shah DN, Sharma DD. Functional outcome of distal femoral fractures treated with DF-LCP [Distal femur locking compression plate]. Int J Orthop Sci. 2018; 4: 439–44.
- Court-brown CM, Caesar B. Epidemiology of adult fractures: A review. 2006.
- Hoskins W, Sheehy R, Edwards ER, Hau RC, Parsons N, Griffin XL. Nails or plates for fracture of the distal femur? data from the victoria orthopaedic trauma outcomes registry. 2016: 846–50.
- Jones-quaidoo SM, Kahler D, Hurwitz S. Distal Femoral Fractures: 2010; 18: 597–607.
- Imam MA, Torieh A, Matthana A. Double plating of intra-articular multifragmentary C3-type distal femoral fractures through the anterior approach. Eur J Orthop Surg Traumatol. 2018; 28: 121–30.
- Hollis AC, Ebbs SR, Mandari FN. The epidemiology and treatment of femur fractures at a northern tanzanian referral centre. Pan Afr Med J. 2015; 22: 1–6.
- Analysis AP, Functional OF, Of O, Distal D, Fractures F, Fixed I, et al. outcome of displaced distal femur fractures internally fixed with distal femur locking. 2013.
- Bandaru H, Shanthappa AH. Plating for Intra-articular Fractures of the Distal Femur: Functional and Radiological Outcomes. Cureus. 2023; 15: 1–6.
- Suveriya DP, Ojha DA. Assessment of functional outcome of distal intra-articular fracture of femur treated with distal femoral LCP by Neer’s score. Int J Orthop Sci. 2020; 6: 681–8.
- Breivik H, Borchgrevink PC, Allen SM, Rosseland LA, Romundstad L, Breivik Hals EK, et al. Assessment of pain. Br J Anaesth. 2008; 101: 17–24.
- Zade SS, Sonawane R, Pangavane S, Harkar V, Devasthali K, Chudasama VD. Functional Outcomes of Intra Articular Distal End Femur Fractures Treated with Locking Compression Plating. MVP J Med Sci. 2022; 8: 199–208.
- Bagherifard A, Majdi S, Motaghi P, Heidarikhoo MR, Khayyami K, Sattari SA, et al. Evaluation of the Outcome of Different Surgical Techniques in the Treatment of Distal Femur Intra-articular Fractures: A Retrospective Study. J Res Orthop Sci. 2021; 8: 1–8.
- Obiegbu O, Ndukwu C. Locking compression plate in distal intra-articular femoral fractures: The swashbuckler’s approach. Niger J Surg Sci. 2018; 28: 23.
- Rademakers MV, Kerkhoffs GMMJ, Sierevelt IN, Raaymakers ELFB, Marti RK. Intra-articular fractures of the distal femur. A long-term follow-up study of surgically treated patients. J Orthop Trauma. 2004; 18: 213–9.
- Hoffmann MF, Jones CB, Sietsema DL, Iii PT, Koenig SJ. Clinical outcomes of locked plating of distal femoral fractures in a retrospective cohort. 2013: 1–9.
- Sié EJB, Mobiot CA, Traoré A, Lambin Y. Distal femoral fractures treated with condylar buttress plate in a West African hospital. J Clin Orthop Trauma. 2012; 3: 98–102.
