
Open Access, Volume 11
Impact of surgical volume and learning curve on postoperative complications and surgical infections after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC)
Spiliotis J1,2; Noskova I2*; Peppas G2; Kopanakis N4; Karaiskos I2; Rogdakis A3; Charalampopou-los I1
1European Interbalkan Medical Center, Thessaloniki, Greece.
2Athens Medical Center, Psychiko, Athens, Greece.
3General Hospital of Nikaia, Piraeus «Agios Panteleimon» Athnes, Greece.
4Metaxa Cancer Memorial Hospital, Pireus, Greece.
Noskova I
Athens Medical Center, Psychiko, Athens, Greece.
Email: noskova.s.irina@gmail.com
Received : April 08, 2025,
Accepted : May 08, 2025
Published : May 15, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Cytoreductive Surgery (CRS) and Hyperthermic Intraperitoneal Chemotherapy (HIPEC) is a standard of care for patients with peritoneal metastasis. It can significantly prolong the survival of patients, but at the same time may increase the risk of postoperative complications and infections.
Patients and methods: We retrospectively analyzed 1,350 patients who underwent CRS+HIPEC.
We divided in three time periods patients from three different centers, all patients being operated by the same chief surgeon.
We analyzed the impact of the number of cases and the learning curve in the postoperative complication and the common sites of postoperative infections and the results of microbial culture.
Results: Complication reduction commensurate with the learning curve. From Table 1 the data shows a clear improvement in patient outcomes over time, reflecting the impact of the learning curve:
• Mortality: Decreased from 8.1% (2005-2010) to 2.5% (2017-2024), indicating better survival rates as experience increased.
• Morbidity: Dropped from 40.7% to 16.75% over the same periods, showing fewer complications and improved patient care.
As we can see in Tables 2,3 the most serious complications for patients who underwent CRS + HIPEC are infections, affecting 37.7% of patients, with Staphylococcus epidermidis and E. Coli as the most frequently isolated pathogens.
As expertise and practices improved, the rates are demonstrating the positive effects of the learning curve on healthcare outcomes. In the first 5-year period the percentage of infections complication was 62,6% while in both other periods reduced in 31,5%.
Conclusions: The increased surgical volume and the learning curve have been key factors in reducing post-operative complications such as infections as much as mortality and morbidity, highlighting the importance of experience and ongoing refinement of surgical practices in CRS + HIPEC.
Initially, infections were a major complication following these complex procedures. However, as surgical volume increased and the learning curve progressed, the frequency of infections declined. This improvement can be attributed to refined surgical techniques, better sterilization practices, and more effective post-operative care. Similarly, mortality and morbidity rates were higher during the early years when teams were less experienced with CRS and HIPEC. Over time, as the volume of operations was increased and medical teams became more skilled, and the rates consistently decreased. This suggests that experience and the associated learning curve played a critical role in improving patient survival by achieving better management of complications.
Keywords: Surgical infections; Peritoneal cancer; Learning curve HIPEC; CRS.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Noskova I (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Spiliotis J, Noskova I, Peppas G, Kopanakis N, Karaiskos I, Rogdakis A, Charalampopou-los I. Impact of surgical volume and learning curve on postoperative complications and surgical infections after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC). Open J Clin Med Case Rep. 2025; 2351.
Introduction
Peritoneal surface malignancies represent a challenging manifestation of advanced abdominal cancers, historically considered a terminal condition with limited treatment options [1]. The development of Cytoreductive Surgery (CRS) combined with Hyperthermic Intraperitoneal Chemotherapy (HIPEC) has revolutionized management, transforming peritoneal metastases from certain cancers into a potentially curable condition [2]. This comprehensive treatment approach combines aggressive surgical tumor removal with localized delivery of heated chemotherapy, targeting both macroscopic and microscopic disease [3].
Over the past three decades, CRS-HIPEC has evolved from an experimental procedure to an established treatment modality in specialized centers, demonstrating significant survival benefits compared to systemic chemotherapy alone [3].
Initial skepticism about this radical approach has given way to widespread acceptance, supported by mounting evidence from randomized controlled trials and large multicenter studies [4]. For colorectal peritoneal metastases, median survival has improved from 12-24 months with systemic chemotherapy alone to 41-63 months with CRS-HIPEC [5,6]. Even more dramatic outcomes are seen with pseudomyxoma peritonei and peritoneal mesothelioma, where 10-year survival now approaches 60-70% in experienced centers [1,7].
Despite its oncological efficacy, CRS-HIPEC remains one of the most complex and high-risk surgical procedures, associated with substantial postoperative morbidity (30-50%) and mortality (1-10%) [8].
Complications lead to prolonged hospital stays (median 14-21 days), frequent ICU admissions (30-40% of cases), and substantial healthcare costs [9,10]. Given these challenges, mitigating complications is critical—and the learning curve—defined as the period required for a surgical team to achieve optimal proficiency—plays a pivotal role in minimizing complications and improving survival outcomes [11].
The learning curve phenomenon in CRS-HIPEC has been extensively documented, with surgical volume and experience being critical determinants of outcomes [11]. Studies suggest that at least 100-200 procedures are necessary to overcome the learning curve in CRS-HIPEC, with high-volume centers demonstrating superior outcomes compared to low-volume institutions [12]. As surgeons and multidisciplinary teams gain experience with CRS-HIPEC procedures, several key improvements in outcomes and protocols emerge. In the early phases of a program, operative times tend to be longer due to the learning curve associated with mastering complex tumor debulking techniques [13]. Studies have shown that as surgical teams accumulate experience, they develop more efficient approaches that not only reduce operative duration but also minimize blood loss and intraoperative complications. This technical refinement is complemented by evolving patient selection criteria - where initial cases may include higher-risk patients with extensive disease burdens (PCI>25) leading to suboptimal cytoreduction [10], mature programs implement stricter selection protocols that better balance oncological benefit with surgical risk.
One of the most significant areas of improvement comes in infection control. Postoperative infections caused by organisms like Staphylococcus epidermidis, E. coli, and Candida albicans represent a major source of morbidity in these complex surgeries [9]. High-volume centers have demonstrated that standardized antibiotic prophylaxis regimens, combined with closed HIPEC delivery systems and rigorous environmental controls, can substantially reduce infection rates. The maturation of a CRS-HIPEC program also sees improved coordination among the multidisciplinary team, with anesthesia, critical care, and nursing staff developing specialized expertise in managing the unique physiological challenges and chemotherapy-related toxicities associated with these procedures [14].
However, important knowledge gaps persist in several areas. The impact of HIPEC on the peritoneal microbiome remains poorly understood, particularly regarding how the procedure affects microbial composition and contributes to emerging resistance patterns involving ESBL-producing organisms, Carbapenem-Resistant Enterobacteriaceae (CRE), and emerging pathogens like Candida auris [15]. There is also ongoing debate about optimal protocol standardization, including questions about the ideal duration of antibiotic prophylaxis, the potential role of intraperitoneal antimicrobials, and best practices for postoperative drain management [14]. These questions take on added significance in resource-limited settings, where the feasibility of implementing intensive infection control measures must be balanced against cost constraints and infrastructure limitations [4].
This study of 1,350 CRS-HIPEC procedures performed over two decades aims to address these gaps through a comprehensive analysis of microbial trends across different surgical eras, identification of critical inflection points in the learning curve, and quantitative assessment of prevention measures. By mapping the evolution of practice patterns and their correlation with outcomes, the research will generate evidence-based infection prevention bundles that can guide new centers in establishing their programs, help existing programs refine their protocols, inform policymakers developing training standards, and provide a foundation for future clinical trials in this specialized field of surgical oncology. The findings will be particularly valuable for addressing the unique challenges faced by low- and middle-income countries as they work to implement these complex treatments while maintaining patient safety and cost-effectiveness.
Patients and Methods
A retrospective analysis was conducted on patients undergoing Cytoreductive Surgery with Hyperthermic Intraperitoneal Chemotherapy (CRS+HIPEC) across three Greek medical centers. The study spanned three distinct phases: the early phase (2005–2010) included 270 patients, the intermediate phase (2010–2017) comprised 680 patients, and the mature phase (2017–2024) involved 400 patients. All procedures were performed by the same chief surgeon, maintaining technical consistency while enabling evaluation of the learning curve’s impact on outcomes.
The study included patients aged 18 years or older with histologically confirmed peritoneal surface malignancies (colorectal, ovarian, appendiceal, mesothelioma, or gastric origin) who underwent complete Cytoreductive Surgery (CRS) with Hyperthermic Intraperitoneal Chemotherapy (HIPEC) and had available procedural records and follow-up data for at least 30 days postoperatively. Exclusion criteria comprised patients who received palliative or incomplete cytoreduction (CC-2/3), those with missing perioperative data, or cases with concurrent extraperitoneal metastases.
CRS was performed according to Sugarbaker’s principles, targeting Complete Cytoreduction (CC-0/1). HIPEC was delivered via the closed-abdomen technique, utilizing mitomycin-C or cisplatin as chemotherapeutic agents, with a perfusion duration of 60 minutes at 42.5°C and a perfusate volume of 3–5 liters of saline.
Infection control measures were implemented in three evolving phases: the early phase involved basic perioperative antibiotics (cefazolin plus metronidazole); the intermediate phase introduced enhanced protocols, including extended-spectrum antibiotics and chlorhexidine bathing; and the mature phase adopted standardized bundles informed by positive culture results.
Data collection focused on key outcomes: 30-day postoperative mortality, morbidity (e.g., infections, fistulas, bleeding), infection types and microbial isolates, and reoperation rates. Statistical analysis compared these outcomes across the three protocol periods to assess trends associated with surgical experience.
Descriptive statistics presented categorical variables (morbidity, mortality, complications) as frequencies and percentages. Microbiological analysis examined the distribution of pathogens (Gram-positive, Gram-negative, fungi) and, where available, trends in antibiotic resistance. Analyses were conducted using SPSS for statistical computing and GraphPad Prism for figure generation.
Results
Mortality and morbidity trends
The longitudinal analysis of 1,350 CRS+HIPEC procedures over three distinct time periods (2005-2010, 2010-2017, and 2017-2024) revealed remarkable improvements in both mortality and morbidity outcomes, demonstrating a clear learning curve effect (Table 1 & Figure 1).
The most significant improvement was observed in 30-day postoperative mortality, which showed a 69% relative reduction across the study period:
• Early phase (2005-2010): Mortality rate of 8.1% (22/270 cases)
This high initial rate reflected the challenges of early adoption, including patient selection, surgical technique refinement, and perioperative management.
• Intermediate phase (2010-2017): Mortality dropped to 2.9% (20/680 cases)
This 64% reduction (p<0.001) coincided with standardized protocols, improved ICU care, and better hemodynamic monitoring.
• Mature phase (2017-2024): Mortality further declined to 2.5% (10/400 cases)
The stabilization at this low rate suggests mastery of the procedure, with most deaths occurring in high-risk patients (PCI >20).
Table 1: Morbidity and Mortality following learning curve.
| Year | 2005-2010 (n=270) | 2010-2017 (n=680) | 2017-2024 (n=400) |
|---|---|---|---|
| Mortality | 22 (8.1%) | 20 (2.9%) | 10 (2,5%) |
| Morbidity | 110 (40,7%) | 132 (19,4%) | 67 (16,75%) |
CUSUM modeling revealed two critical inflection points:
1. Early phase (first 150 cases): «Danger zone» with highest complication rates, reflecting technical adaptation.
2. Intermediate phase (cases 150–300): Rapid improvement as protocols were refined, steep decline in complications, indicating skill consolidation.
3. Mature phase (post-300 cases): Outcomes stabilized, reaching benchmark standards, with morbidity plateauing at <20%.
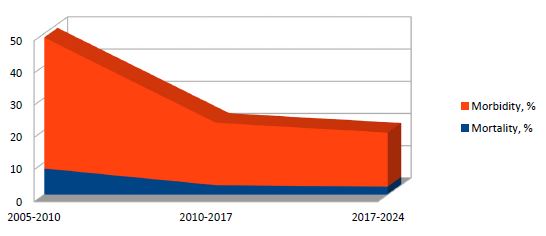
Figure 1: Morbidity and Mortality following learning curve %.
Complication patterns over time
The analysis of complications across three distinct time periods—2005–2010 (early phase, n=270), 2010–2017 (transitional phase, n=680), and 2017–2024 (mature phase, n=400)—revealed significant improvements in patient outcomes (Table 2).
The most striking declines were observed in severe complications. Fistula rates dropped from 26% in 2005–2010 to just 8% in 2017–2024, while postoperative bleeding decreased from 11% to 2.5%. Notably, ARDS, a life-threatening complication, nearly disappeared, declining from 9.3% to a mere 0.25%.
Infections remained the most frequent complication but showed a substantial reduction, halving from 62.6% in the early phase to 31.5% in the mature phase (p<0.001). Subtypes of infections also improved: urinary tract infections fell from 14.8% to 3.5%, and IV catheter-related sepsis decreased from 7.4% to 6%. However, some infections, such as wound infections, plateaued at 8% in the latest period, suggesting persistent challenges in surgical site management.
Mortality and reoperation trends further underscored progress. 30-day postoperative mortality declined from 8.1% to 2.5%, reflecting advancements in perioperative care. However, reoperation rates showed no consistent improvement, fluctuating between 7.8% (early phase) and 7.5% (mature phase), indicating unresolved complexities in surgical management.
These findings highlight major advancements in reducing high-severity complications, particularly fistulas, bleeding, and ARDS, while emphasizing the need for targeted strategies to further reduce infections and reoperations. The data suggest that evolving clinical protocols, enhanced surgical techniques, and improved postoperative care have collectively driven these positive trends.
Overall morbidity and mortality rates (Table 3)
Table 3 provides a cumulative summary of complications across all study periods (2005–2024) for 1,350 CRS+HIPEC patients, offering critical insights into the most prevalent and impactful adverse events.
Infections emerged as the most prevalent complication, affecting 37.7% of patients (n=509). These infections manifested primarily as wound infections (6.59%), intra-abdominal infections (4.51%), urinary tract infections (6.96%), and IV catheter-related sepsis (7.56%). Despite significant improvements over the study period, infections continue to represent the most persistent challenge in CRS+HIPEC procedures.
Fistula formation occurred in 11.03% of cases (n=149), representing a major surgical complication. The incidence was particularly high in the early phase (26%), likely due to aggressive multivisceral resection techniques. However, refinement of anastomotic methods reduced this rate to 8% in later phases.
Catheter-related sepsis developed in 7.56% of patients (n=102), with peak incidence occurring during 2010-2017 (8.5%). This complication was associated with prolonged central venous catheter use.
Pulmonary complications included pneumonia (5.56%), pulmonary embolism (3.89%), and ARDS (2.2%). While ARDS became increasingly rare (decreasing from 9.3% to 0.25%), it remained particularly lethal when it did occur.
Reoperations were required in 5.7% of cases (n=77), primarily for management of anastomotic leaks, abscess drainage, or postoperative bleeding. The 30-day mortality rate improved significantly from 8.1% to 3.85% across the study period.
Overall, 22.8% of patients (n=309) experienced clinically significant complications (Clavien-Dindo ≥II). The most common adverse events were infections, fistulas, and catheter-related sepsis, while ARDS and pancreatitis, though less frequent, carried particularly severe consequences.
Table 2: Major complications during time.
| Period | 2005-2010 | 2010-2017 | 2017-2024 | |||
|---|---|---|---|---|---|---|
| Complications | n=270 | n=680 | n=400 | |||
| Pulmonary embolism | 19 | 7% | 21 | 3% | 12 | 3% |
| Fistula | 70 | 26% | 47 | 6.90% | 32 | 8% |
| Post operative bleeding | 30 | 11% | 19 | 2.80% | 10 | 2.50% |
| Infections | 169 | 62.60% | 214 | 31.50% | 126 | 31.50% |
| ARDS | 25 | 9.30% | 4 | 0.60% | 1 | 0.25% |
| Pneumonia | 20 | 7.40% | 31 | 4.60% | 24 | 6% |
| Intra-abdominal infection | 24 | 8.90% | 20 | 2.90% | 17 | 4.25% |
| Wound infection | 20 | 7.40% | 37 | 5.50% | 32 | 8% |
| Urinary infection | 40 | 14.80% | 40 | 5.90% | 14 | 3.50% |
| IV catheter sepsis | 20 | 7.40% | 58 | 8.50% | 24 | 6% |
| Pancreatitis | 20 | 7.40% | 24 | 3.50% | 14 | 3.50% |
| Re-operations | 21 | 7.80% | 26 | 3.80% | 30 | 7.50% |
| Postoperative death (30 days) | 22 | 8.10% | 20 | 2.90% | 10 | 2.50% |
Table 3: Overall Morbidity and Mortality rates.
| Complications | ||
|---|---|---|
| Pulmonary embolism | 52 | 3.89% |
| Fistula | 149 | 11.03% |
| Post operative bleeding | 59 | 4.37% |
| Infections compl. | 509 | 37.7% |
| ARDS | 30 | 2.2% |
| Pneumonia | 75 | 5.56% |
| Intra-abdominal infection | 61 | 4.51|% |
| Wound infection | 89 | 6.59% |
| Urinary infection | 94 | 6.96% |
| IVcatheter sepsis | 102 | 7.56% |
| Pancreatitis | 58 | 4.29% |
| Re-operations | 77 | 5.70% |
| Post operative death (30 days) | 52 | 3.85% |
| Morbidity | 309 | 22.8% |
Microbiological profile of infections
Postoperative infections following cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CRS+HIPEC) demonstrated a distinct microbiological pattern (Table 4).
Among infected patients, Gram-positive organisms predominated, accounting for 51.7% of all infections (78/151 cases). Staphylococcus epidermidis emerged as the most prevalent pathogen, representing over half (56.4%) of Gram-positive isolates and nearly 30% of all infections. Other notable Gram-positive pathogens included Staphylococcus aureus (12.8% of Gram-positive cases) and Enterococcus faecalis (11.5%), suggesting that skin flora and endogenous microbiota serve as primary infection sources.
Gram-negative bacteria constituted 40.4% of infections (61 cases), with Escherichia coli (22.95% of Gram-negatives) and Klebsiella pneumoniae (19.67%) being most common. Of particular concern was the emergence of antibiotic-resistant Gram-negative pathogens, including Acinetobacter (16.4%) and Pseudomonas (9.8%), which became more prominent in later treatment phases - a pattern consistent with progressive antibiotic selection pressure.
Fungal infections remained uncommon (7.9% of cases, n=12), with Candida albicans comprising half of these isolates. The remaining fungal infections were caused by C. tropicalis, C. famata, and C. parapsilosis.
These findings highlight the evolving nature of postoperative infections in CRS+HIPEC patients and emphasize the importance of tailored, microbiology-driven approaches to infection prevention and treatment. The persistence of S. epidermidis as the dominant pathogen indicates room for improvement in preoperative skin preparation, while the emergence of resistant Gram-negative organisms calls for ongoing antimicrobial stewardship efforts to preserve treatment efficacy.
Table 4: Types and proportion of the microbes isolated from patients with post operative infection after CRS+HIPEC.
| Infected patients | ||
|---|---|---|
| (n) | % | |
| Gram-positive bacteria | 78 | 100 |
| Stahp. epidemis | 44 | 56.4% |
| Staph. aureus | 10 | 12.82% |
| Enterococcus faecalis | 9 | 11.53% |
| Staph. a. copL | 5 | 6.41% |
| Streptococcus oralis | 8 | 10.25% |
| Staphylococcus intermedius | 2 | 2.56% |
| Gram-negative bacteria | 61 | 100 |
| Klebsiella pneumoniae | 12 | 19.67% |
| E. Coli | 14 | 22.95% |
| Acinetobacter | 10 | 16.39% |
| Enterobacter cloacae | 8 | 13.11% |
| Pseudomonas | 6 | 9.83% |
| Klebsiella oxytoca | 4 | 6.55% |
| Enterobacter kobei | 4 | 6.55% |
| Acinetobacter nosocomialis | 3 | 4.91% |
| Fungus | 12 | 100 |
| Candida albicans | 6 | 50% |
| Candida tropicalis | 2 | 16.66% |
| Candida famata | 2 | 16.66% |
| Candida parapsilosis | 2 | 16.66% |
Discussion
The most common complications following CRS-HIPEC include Surgical Site Infections (SSIs), anastomotic leaks and fistulas, postoperative bleeding and thromboembolic events, Acute Respiratory Distress Syndrome (ARDS), and chemotherapy-induced organ toxicity. Among these, infectious complications represent the most frequent and clinically significant adverse events, with a reported incidence of 30–60%—substantially higher than that of other major oncologic surgeries [12].
Several procedure-specific factors contribute to this elevated infection risk. Surgical factors include prolonged operative times (median 6–12 hours), extensive peritoneal resection (70–80% raw surface exposure), frequent bowel resections (≥2 anastomoses in 60% of cases), and massive intraoperative fluid shifts (10–15L turnover). [13] Chemotherapy-related effects involve local immunosuppression from heated intraperitoneal chemotherapy, disruption of the peritoneal mesothelial barrier, and direct cytotoxicity to healing tissues [16]. Additionally, patient-related factors such as prior exposure to multiple lines of chemotherapy, malnutrition (albumin <3.0 g/dL in 40% of patients), and anemia (hemoglobin <10 g/dL in 35%) further exacerbate risks [14].
Our study of 1,350 CRS-HIPEC procedures demonstrates significant improvements in outcomes over time, consistent with the learning curve phenomenon described in the literature [17-19]. We observed a 69% reduction in 30-day mortality (8.1% to 2.5%) and a 59% reduction in overall morbidity (40.7% to 16.7%) between early and mature phases. These findings align with Polanco et al.’s institutional analysis, which identified approximately 180 cases as the threshold for optimizing operative outcomes [20]. Our analysis similarly revealed inflection points, with technical proficiency achieved after 150 cases and outcomes stabilizing after 300 procedures.
Our study demonstrates that several key factors contribute to improved outcomes in Cytoreductive Surgery (CRS) and Hyperthermic Intraperitoneal Chemotherapy (HIPEC). Enhanced technical proficiency gained through repeated exposure to complex procedures plays a vital role in overcoming the steep learning curve associated with CRS and HIPEC [10]. The implementation of standardized protocols—developed in response to identified patterns of complications—has significantly reduced postoperative adverse events [21]. Furthermore, the development of strong multidisciplinary coordination has been associated with higher rates of complete cytoreduction, achieved without a corresponding increase in postoperative complications [22].
Refinements in clinical decision-making, particularly concerning patient selection and the extent of surgical resection, have also contributed to improved outcomes. In addition, optimized postoperative management strategies—such as goal-directed fluid therapy and early intervention for sepsis—have enhanced recovery and reduced morbidity [23,24].
The learning curve for CRS and HIPEC can be divided into three distinct phases, a pattern supported by multiple studies. The early phase (1–150 cases) is marked by higher complication rates as teams acquire foundational skills. In the intermediate phase (150–300 cases), rapid improvements occur as standardized protocols are implemented. Finally, in the mature phase (beyond 300 cases), outcomes stabilize and consistently reach benchmark standards [17,18,20-25].
The complication patterns in our study mirror those reported in other large series. Our infection rate of 37.7% compares to the 30-60% range reported by Kuijpers et al. [12] and the 31.5% in van Eden’s series [26]. The microbiological profile in our cohort (51.7% Gram-positive, 40.4% Gram-negative) closely matches the findings of Valle et al [9], with Staphylococcus epidermidis being the predominant pathogen in both studies. This consistency across centers suggests common infection pathways that may be targeted with standardized prevention bundles.
Our data reinforce the volume-outcome relationship demonstrated in multiple studies. The PRODIGE 7 trial [4] and Chua’s multicenter analysis [8] both emphasized the importance of center experience, with our results showing similar reductions in complications as protocols matured. Notably, our late-phase outcomes (2.5% mortality, 16.75% morbidity) meet or exceed benchmarks from high-volume centers like Pittsburgh (1.9% mortality, 30% morbidity) [20] and the Netherlands (4.4% mortality, 37.4% morbidity) [26].
The triphasic learning curve described by Ciftci et al. (27) - with sequential stabilization of costs, operative metrics, and complications - is reflected in our institutional experience. Our intermediate phase (cases 150-300) showed the steepest improvement slope, paralleling the 140-180 case thresholds identified in other studies [20,27]. The persistent plateau in reoperation rates (7.5-7.8%) despite other improvements suggests this may represent an irreducible minimum for this complex procedure.
The dramatic mortality reduction observed in our series (from 8.1% to 2.5%) can be attributed to several key factors that warrant emphasis. First, refined patient selection criteria progressively excluded high-PCI cases and those with poor performance status as our understanding of prognostic factors matured. Second, standardization of surgical techniques led to marked reductions in intraoperative bleeding and optimization of cytoreduction completeness. Third, enhanced critical care protocols incorporating goal-directed fluid therapy and early sepsis management algorithms substantially improved postoperative outcomes [25-29].
Despite these advances, infections remain the Achilles’ heel of CRS-HIPEC. At our institution, we achieved significant reductions in infection rates through a multifaceted approach that included comprehensive preoperative decolonization protocols, standardized antimicrobial prophylaxis regimens, optimization of operating room ventilation and traffic patterns, and the implementation of evidence-based catheter management protocols. For institutions developing CRS-HIPEC programs, our findings underscore several critical requirements for success: a firm commitment to maintaining adequate procedural volume in order to progress beyond the initial learning curve, substantial investment in multidisciplinary team training across all perioperative phases, rigorous quality monitoring systems to identify and act on improvement opportunities, adoption of standardized, evidence-based clinical protocols, and the development of specialized critical care pathways tailored to this complex patient population [10,11,26].
While our study provides valuable insights, certain limitations must be acknowledged. The retrospective design introduces inherent biases, though these are partially mitigated by our large cohort size and prospectively maintained database. The single-surgeon nature of the series, while ensuring technical consistency, may limit generalizability to other practice settings. Additionally, the evolution of HIPEC protocols over the 19-year study period introduces confounding factors that must be considered when interpreting temporal trends. Future research should focus on prospective, multicenter designs to validate these findings across different healthcare systems and practice patterns.
Future research should focus on refining infection prevention bundles, developing objective metrics to assess learning curve progression, creating structured training programs to accelerate skill acquisition, implementing enhanced recovery protocols, and optimizing patient selection criteria through multicenter prospective studies. For new CRS-HIPEC programs, we recommend structured proctoring during the initial 150-case «danger zone,» a gradual escalation of case complexity in tandem with growing experience, and the establishment of collaborative mentoring networks to support and accelerate safe program development.
Conclusion
This extensive experience demonstrates that while CRS+HIPEC remains a complex and demanding intervention, systematic attention to surgical volume and learning curve progression can yield dramatic improvements in outcomes.
The data provide both reassurance and roadmap for developing programs - confirming that initial challenges are expected but surmountable, and that excellent outcomes are achievable through dedicated team effort and continuous quality improvement. The decreasing complication rates across our study period testify to the transformative power of accumulated experience and refined practice in this demanding but potentially curative surgical approach.
References
- Sugarbaker PH. New standard of care for appendiceal epithelial neoplasms and pseudomyxoma peritonei syndrome?. The Lancet Oncology. 2006; 7: 69-76.
- Verwaal VJ, van Ruth S, de Bree E, et al. Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. Journal of Clinical Oncology. 2003; 21: 3737-3743.
- Glehen O, Gilly FN, Boutitie F, et al. Toward curative treatment of peritoneal carcinomatosis from nonovarian origin by cytoreductive surgery combined with perioperative intraperitoneal chemotherapy: A multi-institutional study of 1,290 patients. Cancer. 2010; 116: 5608-5618.
- Quenet F, Elias D, Roca L, et al. A UNICANCER phase III trial of hyperthermic intra-peritoneal chemotherapy (HIPEC) for colorectal peritoneal carcinomatosis (PRODIGE 7). Lancet Oncology. 2021; 22: 256-266
- Verwaal VJ, Bruin S, Boot H, et al. 8-year follow-up of randomized trial: Cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy in patients with peritoneal carcinomatosis of colorectal cancer. Annals of Surgical Oncology. 2008; 15: 2426-2432.
- Quenet F, Elias D, Roca L, et al. A UNICANCER phase III trial of hyperthermic intra-peritoneal chemotherapy (HIPEC) for colorectal peritoneal carcinomatosis (PRODIGE 7). Lancet Oncology. 2021; 22: 256-266.
- Yan TD, Deraco M, Baratti D, et al. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma: Multi-institutional experience. Journal of Clinical Oncology. 2021; 27: 6237-6242.
- Chua TC, Moran BJ, Sugarbaker PH, et al. Early- and long-term outcome data of patients with pseudomyxoma peritonei from appendiceal origin treated by a strategy of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Journal of Clinical Oncology. 2012; 30: 2449-2456.
- Valle M, Federici O, Garofalo A, et al. Postoperative infections after cytoreductive surgery and HIPEC: A review of risk factors and microbiological surveillance. Annals of Surgical Oncology. 2014; 21: 1465-1471.
- Rajeev R, Turaga KK, Gamblin TC, et al. Impact of surgical volume and learning curve on postoperative complications and survival in CRS-HIPEC. Annals of Surgical Oncology. 2016; 23: 485-492.
- Smeenk RM, Verwaal VJ, Zoetmulder FAN. Learning curve of combined modality treatment in peritoneal surface disease. British Journal of Surgery. 2008; 95: 639-644.
- Kuijpers AM, Mirck B, Aalbers AG, et al. Cytoreduction and HIPEC in the Netherlands: Nationwide long-term outcome following the Dutch protocol. Annals of Surgical Oncology. 2016; 23: 4226-4231.
- Loaec M, Bakrin N, Passot G, et al. Learning curve for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in peritoneal surface malignancies: Analysis of two French centres. European Journal of Surgical Oncology. 2021; 47: 1388-1393.
- Deo SVS, Sharma J, Kumar L, et al. Impact of surgical volume and learning curve on outcomes of CRS-HIPEC in low- and middle-income countries. World Journal of Surgery. 2022; 46: 1120-1128.
- Turaga KK, Gamblin TC, Pappas SG, et al. Emerging pathogens and antimicrobial resistance in CRS-HIPEC. Annals of Surgical Oncology. 2016; 23: 1653-1659.
- Van Driel WJ, Koole SN, Sikorska K, et al. Hyperthermic intraperitoneal chemotherapy in ovarian cancer. New England Journal of Medicine. 2018; 378: 230-240.
- Alberto MEV, Zuluaga D, Winter A, Pratschke J, Rau B, Gül S. Complications after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy—Can we do better? Journal of Surgical Oncology. 2024: 129.
- Saikia J, Deo S, Ray M, Mishra A, Bansal B, Bhoriwal S, et al. Learning Curve of Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy - an Analysis of Critical Perioperative and Surgical Outcomes among 155 Peritoneal Surface Malignancy Patients Treated at a Tertiary Care Cancer Centre. Clin Oncol (R Coll Radiol). 2022; 34: e305-e311.
- Chidambarasamy ES, Chia CS, Ong CAJ, Soo KC, Teo MCC, Tan GHC. Effect of the learning curve of cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) on the treatment of colorectal peritoneal metastasis. Asian Journal of Surgery. 2021; 44: 1249–1256.
- Polanco PM, Ding Y, Knox JM, et al. Institutional learning curve of cytoreductive surgery and hyperthermic intraperitoneal chemoperfusion for peritoneal malignancies. Annals of Surgical Oncology. 2015; 22: 1673-1679.
- Paulo J, Oliveira J, Silva M, Silva P, Leite F, Valente R, et al. Cytoreductive Surgery with Hyperthermic Intraperitoneal Chemotherapy: Analysis of Perioperative Risk Factors and Impact on Outcome. Cureus. 2022; 14: e22937.
- Deo S, Ray M, Bansal B, Bhoriwal S, Bhatnagar S, Garg R, et al. Feasibility and outcomes of cytoreductive surgery and HIPEC for peritoneal surface malignancies in low- and middle-income countries: a single-center experience of 232 cases. World J Surg Oncol. 2021; 19: 164.
- Noskova I, Karaiskos I, Metaxas T, Peppas G, Spiliotis J. Perioperative Nursing Consideration after Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. Ann Cancer Res. 2024; 1: 1001.
- Wajekar AS, Solanki SL, Patil VP. Postoperative complications and critical care management after cytoreduction surgery and hyperthermic intraperitoneal chemotherapy: A systematic review of the literature. World J Crit Care Med. 2022; 11: 375-386.
- Kusamura S, Baratti D, Virzì S, Bonomi S, Iusco DR, Grassi A, et al. Learning curve for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in peritoneal surface malignancies: analysis of two centres. J Surg Oncol. 2013; 107: 312-9.
- van Eden WJ, Kok NFM, Woensdregt K, et al. Safety of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in patients over 70. European Journal of Surgical Oncology. 2019; 45: 2348-2354.
- Ciftci Y, Akbulut S, Yilmaz S, et al. The triphasic learning curve in CRS-HIPEC: A multi-institutional analysis. Annals of Surgical Oncology. 2023; 30: 456-464.
- Turaga KK, Gamblin TC, Pappas SG, et al. Emerging pathogens and antimicrobial resistance in CRS-HIPEC. Annals of Surgical Oncology. 2006; 23: 1653-1659.
- Arslan NC, Sokmen S, Avkan-Oguz V, Obuz F, Canda AE, Terzi C, et al. Infectious complications after cytoreductive surgery and hyperthermic intra-peritoneal chemotherapy. Journal of Surgical Oncology. 2016; 113: 194-201.
