
Open Access, Volume 11
Hypothalamic hamartoma (HH) as a bystander to epileptogenicity – case study with stereoEEG and RNS
Shamseldin Metwally1; Joanna Fong-Isariyawongse, MD1; Thandar Aung, MD1; Niravkumar Barot, MD2; Anto Bagić, MD, PhD, FAES, FACN1; Jorge Gonzalez-Martinez, MD, PhD1; Alexandra Urban, MD, FAAN, FAES1; Carolina Cuello-Oderiz, MD1*
1University of Pittsburgh Medical Center and University of Pittsburg school of Medicine, USA.
2Beth Israel Deaconess Medical Center, USA.
Carolina Cuello-Oderiz, MD
University of Pittsburgh Medical Center and University of Pittsburg school of Medicine, USA.
Email: carolinacuellooderiz@gmail.com
Received : April 15, 2025,
Accepted : May 06, 2025
Published : May 15, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Rationale: There is discussion about the role of hypothalamic hamartoma (HH) in the epileptogenicity.
Methods: Case report.
Results: 33 year old right handed male with intractable epilepsy since infancy, HH and developmental delay who was evaluated with stereoEEG (SEEG). He had two prior surgeries: a) subtotal resection of hypothalamic hamartoma and mid corpus callosum and b) right-sided hamartoma (HH) ablation. his seizure semiology has evolved from prior gelastic/tonic/atonic, to mostly tonic, along with encephalopathy, depression, and psychosis. SEEG showed multifocal interictal discharges. There were neither interictal nor ictal anomalies in the residual HH. Patient underwent Responsive Neurostimulation Implantation (RNS) in bilateral anterior thalamus. Seizures were captured from both leads, left as predominant side.
Conclusions: We hypothesize that HH is a bystander of epileptogenicity in this group of patients and RNS targeting thalamus is an efficient treatment.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Cuello-Oderiz C (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Metwally S, Fong-Isariyawngse J, Aung T, Barot N, Bagić A, Gonzalez-Martinez J, Cuello-Oderiz C, et al. Hypothalamic hamartoma (HH) as a bystander to epileptogenicity – case study with stereoEEG and RNS. Open J Clin Med Case Rep. 2025; 2350.
Introduction
The role of Hypothalamic Hamartoma (HH) in epileptogenicity remains controversial. Although gelastic seizures characterized by inappropriate and unprovoked episodes of laughter, are considered the hallmark seizure type of HH, other seizure types can be seen [1]. Somatic mutations in Sonic hedgehog (Shh)-related genes found in about a third of nonsyndromic HH patients and some other genetic abnormalities have been described [2]. In patients with epilepsy and HH, the various interictal and ictal scalp patterns described in the literature raise the question of whether there is a single association between HH and epilepsy or a spectrum. Additionally, patients often undergo surgical interventions for HH with variable outcomes, further supporting this question [4]. It remains unclear whether a unique pattern exists, or if the long-standing history of epilepsy in patients with HH leads to independent epileptogenesis that alters the observed patterns.
Case Description
This case report pertains to a 33-year-old, right-handed male with a history of Drug-Resistant Epilepsy (DRE) since infancy, developmental delay, and HH. He had two surgeries during pediatric age: 1) a subtotal resection of an HH and the mid-corpus callosum; 2) a right-sided HH laser ablation. The patient’s seizure semiology has evolved from a combination of gelastic and tonic (and potentially atonic) seizures during childhood to mainly uncontrolled generalized tonic seizures. Furthermore, the patient developed the following neuropsychiatric symptoms: catatonia, delusions, paranoia, depression and encephalopathy. Those symptoms prompted an epilepsy monitoring unit admission and while the patient was confused there were no EEG changes. Due to the nature of drug resistance epilepsy, he underwent phase I of pre surgical evaluation, and it was decided to proceed with stereoEEG.
StereoEEG (sEEG) was implanted with bilateral coverage of the motor/pre-motor areas, corpus callosum and one orthogonal electrode aiming to the residual HH (Figure 1).
The recording showed two electroclinical seizures that were poorly localized and showed diffuse attenuation during their onsets, followed by low voltage, fast activity in the Supplementary Motor Area (SMA) and preSMA with rapid spread (Figure 2). Additionally, a run of paroxysmal fast activity during sleep was captured. The seizures and interictal and ictal epileptiform discharges were absent in the residual HH. With the suspicion that the epileptic network involved the anterior cingulate gyrus, the patient underwent responsive neurostimulation (RNS) in the bilateral anteriorthalamus to target the limbic circuit of Papez [5]. Post-implantation seizures were captured from both leads, but predominantly on the left side (Figure 3).
Outcome
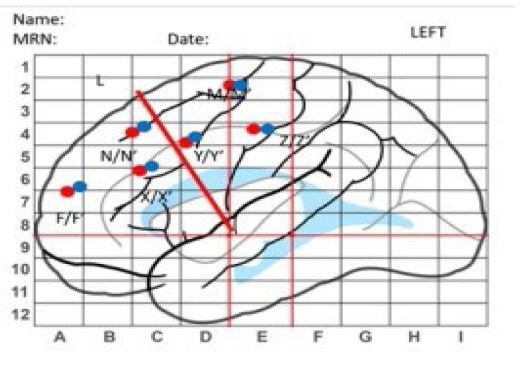
Figure 1: SteroEEG implantation scheme.
This figure illustrates a brain mapping grid overlaid on a schematic representation of a left hemisphere of a human brain. The sEEG electrodes were implanted with bilateral coverage of the motor/pre-motor areas, corpus callosum and one orthogonal electrode aiming to the residual HH.
This figure illustrates a brain mapping grid overlaid on a schematic representation of a left hemisphere of a human brain. The sEEG electrodes were implanted with bilateral coverage of the motor/pre-motor areas, corpus callosum and one orthogonal electrode aiming to the residual HH.
Figure 2: EEG recording during seizure activity.
Electroclinical seizure showed diffuse attenuation at the onset followed by low voltage fast activity at Supplementary Motor Area (SMA) and preSMA with rapid spread.
Electroclinical seizure showed diffuse attenuation at the onset followed by low voltage fast activity at Supplementary Motor Area (SMA) and preSMA with rapid spread.
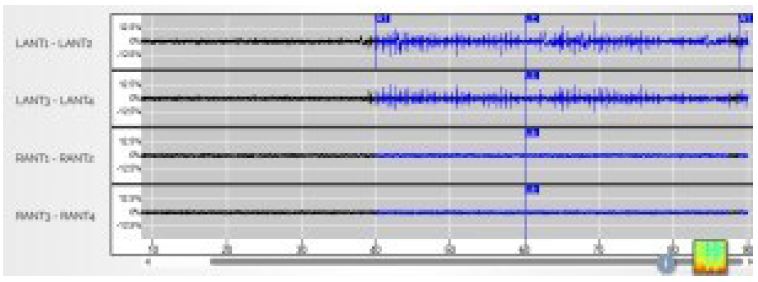
Figure 3: RNS echo. LANT: left anterior thalamus, RANT: right anterior thalamus.
Responsive neurostimulation of both left and right anterior thalamic nuclei showing a seizure arising from left anterior thalamus.
Responsive neurostimulation of both left and right anterior thalamic nuclei showing a seizure arising from left anterior thalamus.
Discussion
HHs are rare brain malformations associated with DRE. Typically, gelastic/dacrystic seizures were described. Other manifestations include rage attacks and cognitive impairment [2]. Recent studies have shed light on potential genetic causes of HH. Somatic mutations in the sonic hedgehog (Shh)-related genes and germline mutations in GLI3 are two potential culprits in HH development [2]. Studies using sEEG have shown the epileptogenic nature of HH, especially in gelastic seizures. sEEG also provided evidence of the lack of involvement of HH in other seizure types like Focal Impaired Awareness Seizures (FIAS), dyscognitive seizures, and tonic-clonic seizures outside its boundaries [6-8].
In our case, we found that seizures can originate from regions outside the HH. We believe that a kindling-like phenomenon is seen in patients with HHs and epilepsy. In prior studies, epileptogenicity has been found in frontal, cingulate gyrus, and temporal lobes [8]. For some patients, surgery fails to alleviate seizures entirely, suggesting also the involvement of distant cortical regions. There's a suggestion of kindling-like interactions between HHs and the neocortex, indicating a dynamic network underlying seizure generation [6].
Several studies suggested that the Anterior Thalamic Nucleus (ANT), due to its important regulatory function in the limbic-striate system, has antiseizure properties and is a potential target for treating DRE [9]. Although previous reports have suggested connections between HH lesions and the ANT using Single-photon Emission Computed Tomography (SPECT), others reported no hyperperfusion in the mammillothalamic-cingulate pathway, which includes the ANT [10] This absence of hyperperfusion could be due to the limited sensitivity of SPECT in detecting seizure activity originating from small HH lesions [2]. Or that the anti-seizure effect of stimulating the ANT is caused by involving areas such as anterior cingulate which has been part of the epileptic network because of secondary epileptogenicity. The brain Responsive Neurostimulation System (RNS) may represent a novel tool to treat patients with DRE and HH [6].
Conclusion
Our case demonstrates that, using sEEG recordings, HH can be shown to be a bystander of epileptogenicity, specifically in long-standing epilepsy and the absence of gelastic seizures. Genetic abnormalities may cause a predisposition to multifocal epilepsy. Encephalopathy, depression, and psychosis have been described in patients with HH and chronic epilepsy, further supporting a diffuse process [9,11]. ANT RNS represents an effective treatment, and it may be considered as the first line of DRE in this group of patients.
References
- Castro LH, Ferreira LK, Teles LR, Jorge CL, Arantes PR, Ono CR, et al. Epilepsy syndromes associated with hypothalamic hamartomas. Seizure. 2007;16(1):50-8.
- Cohen NT, Cross JH, Arzimanoglou A, Berkovic SF, Kerrigan JF, Miller IP, et al. Hypothalamic Hamartomas: Evolving Understanding and Management. Neurology. 2021;97(18):864-73.
- Fujita A, Higashijima T, Shirozu H, Masuda H, Sonoda M, Tohyama J, et al. Pathogenic variants of DYNC2H1, KIAA0556, and PTPN11 associated with hypothalamic hamartoma. Neurology. 2019;93(3):e237-e51.
- Mullatti N, Selway R, Nashef L, Elwes R, Honavar M, Chandler C, et al. The clinical spectrum of epilepsy in children and adults with hypothalamic hamartoma. Epilepsia. 2003;44(10):1310-9.
- Valentin A, Lazaro M, Mullatti N, Cervantes S, Malik I, Selway RP, et al. Cingulate epileptogenesis in hypothalamic hamartoma. Epilepsia. 2011;52(5):e35-9.
- Wang D, Shan Y, Bartolomei F, Kahane P, An Y, Li M, et al. Electrophysiological properties and seizure networks in hypothalamic hamartoma. Ann Clin Transl Neurol. 2020;7(5):653-66.
- Li P, Zhou Y, Zhang Q, Yang Y, Wang M, Zhu R, et al. Frameless robot-assisted stereoelectroencephalography-guided radiofrequency: methodology, results, complications and stereotactic application accuracy in pediatric hypothalamic hamartomas. Front Neurol. 2023;14:1259171.
- Scholly J, Staack AM, Kahane P, Scavarda D, Regis J, Hirsch E, et al. Hypothalamic hamartoma: Epileptogenesis beyond the lesion? Epilepsia. 2017;58 Suppl 2:32-40.
- Roa JA, Abramova M, Fields M, Vega-Talbott M, Yoo J, Marcuse L, et al. Responsive Neurostimulation of the Thalamus for the Treatment of Refractory Epilepsy. Front Hum Neurosci. 2022;16:926337.
- Conde Blanco E, Anciones Martin C, Manzanares I, Gil Lopez F, Roldan P, Donaire A, et al. Hypothalamic hamartomas in adulthood: Clinical spectrum and treatment outcome-A unicenter experience. Brain Behav. 2019;9(11):e01412.
- Veendrick-Meekes MJ, Verhoeven WM, van Erp MG, van Blarikom W, Tuinier S. Neuropsychiatric aspects of patients with hypothalamic hamartomas. Epilepsy Behav. 2007;11(2):218-21.
