
Open Access, Volume 11
Radiation induced morphea of the breast following radiotherapy for breast cancer
Shelley Stokes1; Femi E Ayeni1,3*; Michael T Hughes2; Senarath Edirimanne1
1Department of Surgery, Nepean Hospital, Australia.
2 Department of Surgery, Sydney Adventist Hospital Clinical School, Australia.
3Nepean Institute of Academic Surgery, Nepean Clinical School, The University of Sydney, Australia.
Femi E Ayeni
Nepean Institute of Academic Surgery, The University of Sydney, 62 Derby St, Penrith, NSW 2750, Australia.
Email: femi.ayeni@sydney.edu.au
Received : March 16, 2025,
Accepted : April 15, 2025;
Published : April 30, 2025,
Archived : www.jclinmedcasereports.com
Abstract
CentralMorphea, alternatively known as localising scleroderma, is a rare complication of radiotherapy affecting 1 in 500 patients. To date there have been 82 cases reported in the literature however it may be under diagnosed and the prevalence may be underestimated.
We report 3 cases of radiation induced morphea in the radiotherapy field including breast in a cohort of 2000 breast cancer patients who received radiotherapy following breast-conserving surgery. Patients developed combinations of atrophy, contracture and ulceration of the irradiated breast 13, 15 and 30 months after radiotherapy. Punch biopsies showed chronic inflammation. Histopathology and imaging excluded malignancy. The connective tissue disorder screens were negative. Two patients were treated with a course of oral corticosteroids and their ulcerations healed. Morphea remained stable at 1- and 5-year follow-up and in the third patient they resorted to mastectomy and reconstruction for symptomatic relief.
Radiation induced morphea can occur months to up to 32 years after radiotherapy and its pathophysiology is not completely elucidated. Punch biopsy and imaging are important to confirm diagnosis and exclude malignancy. Morphea may resolve spontaneously with 50% of cases moving into a state of abeyance within approximately three years. When diagnosed within the first 6 months topical calcipotriene, tacrolimus, phototherapy and systemic methotrexate or corticosteroids have been used alleviate symptoms and remission may be induced if treated promptly. Once stable inactive disease is present there is minimal evidence for systemic therapy. There are reports of surgical reconstruction for morphea demonstrating good cosmesis.
Keywords: Radiation; Morphea; Localised sclerosis; Breast cancer.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Ayeni FE (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Stokes S, Ayeni FE, Hughes MT, Edirimanne S. Radiation induced morphea of the breast following radiotherapy for breast cancer. Open J Clin Med Case Rep. 2025; 2345.
Introduction
Breast cancer is the most common cancer diagnosed in women worldwide constituting 24.2% of all new cancer diagnoses [1]. Radiotherapy for breast cancer reduces recurrence and breast cancer death [2]. Morphea, also known as localising scleroderma, is a rare complication of radiotherapy reported to effect one in every 500 patients [3,4]. There is limited data pertaining to the propensity of specific patient factors to increase the risk of development of specific types of morphea. In the setting of generalised morphea the prevalence is four times more likely in those with underlying autoimmune disease in their family history [5] yet it is unknown if this extends to those who develop morphea after radiation therapy.
Morphea may occur in months to years post radiotherapy [6], up to 32 years [7] has been reported following treatment effecting areas including and even remote from irradiated tissue [8]. Morphea may resolve spontaneously with 50% of cases moving into a state of abeyance within 2.7 years [9] following onset of disease yet patients may be left with pain, pigment changes, contracture with deformity and atrophy.
The pathogenesis of radiation induced morphea has not been clearly elucidated. Theories of pathogenesis, primarily based on that of generalised morphea, describe a complex interaction of underlying genetic susceptibility, epigenetics and triggering environmental insults such as radiation [10]. It has been proposed that neoantigen production [11] generates an autoimmune reaction which is predominantly a Th2 T cell response [12], likely contributed to by vascular dysfunction, leading to inflammation affecting mesodermal derived tissues [13] with TGF-beta [14] release activating fibroblasts, resulting in dysregulation of collagen deposition, fibrosis, sclerosis and eventually atrophy [15].
We present 3 cases to highlight post-radiotherapy morphea and the importance of early recognition and treatment.
Cases Descriptions
Case 1
A 61-year-old female who underwent a right sided wide local excision and sentinel lymph node biopsy for a 30 mm lobular carcinoma grade 3, ER/PR (+) HER2 (-) node negative disease. Her background medical history included hypothyroidism, depression and current smoking. Treated with letrozole then tamoxifen then changed back to letrozole. Adjuvant radiotherapy consisted of 50 Gy in 19 fractions with phase II boost. There was a mild skin reaction at time of radiotherapy (Figure 1). Following radiotherapy, the patient commenced adjuvant endocrine therapy. 15 months after initial radiotherapy morphea of the treated breast was diagnosed. This manifested clinically as atrophy and contracture of the breast. Punch biopsy was performed, and histopathology demonstrated chronic inflammation/fibrosis with no evidence of malignancy (Figure 2). Mammography and ultrasound imaging failed to demonstrate any evidence of cancer recurrence. Connective tissue disorder screens were negative. The patient was treated with oral corticosteroids and morphea was clinically stable at one year
Case 2
A 71-year-old female who underwent a right wide local excision and sentinel lymph node biopsy for a 15 mm invasive ductal carcinoma, no special type grade 3 with 17 mm ductal carcinoma in situ ER/PR/HER2 positive, node negative cancer. Her background medical history included moderate aortic regurgitation, osteoarthritis and gastro-oesophageal reflux. There were no acute surgical complications. The patient received post-operative adjuvant systemic treatment with trastuzumab. Seven months after surgery oedema of the right breast was noted and was found to be due to a seroma of 24 milliliters which was successfully aspirated. Radiotherapy was commenced consisting of sequenced boost radiotherapy with phase I 42.5 Gy/16F and phase II 10 Gy/4F . Followed by anastrozole. Morphea was diagnosed 13 months post operatively. The features were breast contraction, atrophy and axillary ulceration. Investigations consisting of ultrasound, mammography, PDG PET CT and punch biopsies demonstrated no cancer recurrence. The histopathology did demonstrate chronic inflammation with eosinophilia. Following treatment with prednisolone there was resolution of symptoms 6 months later and this is now stable at 5 years.
Case 3
A 50-year-old female who underwent a left wide local excision and sentinel lymph node biopsy for a 22 mm invasive ductal carcinoma Grade 3, triple negative, lymph node negative cancer. Background included depression, mild asthma, gastro-oesophageal reflux, type 2 diabetes mellitus and 70 g ETOH ingestion daily. There were no acute operative complications. Chemotherapy consisted of pacitaxol and Carboplatin. Adjuvant radiotherapy was 50 Gy/25F delivered to the whole breast + 10 Gy/5F local boost. Skin reaction with marked erythema at time of radiation was suspected to be an infection however skin swabs were negative. At 18 months significant lymphoedema developed which then resolved. At 30 months the patient presented with moderate breast fibrosis and marked atrophy and contracture. The estimated volume loss was 80%. There was involvement of the breast tissue only with no extension to the chest wall. Core biopsies of the hardened breast tissue demonstrated fibrosis and no evidence of malignancy. Imaging demonstrated focal scarring on ultrasound, marked skin thickening on mammography but no evidence of recurrence of the cancer. A connective tissue disorder screen was negative. Mastectomy with reconstruction was subsequently undertaken at the patient’s request. The surgical histopathology demonstrated fibrosis and underlying fat necrosis.

Figure 1: Patient (case 1) during treatment.
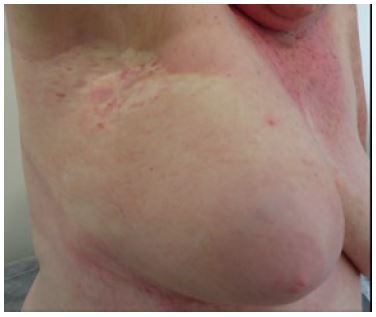
Figure 2: Patient (case 1) with healed axillary ulcerations.
Discussion/Conclusions
Radiation induced breast morphea is a poorly recognised condition that is responsible for unsatisfactory outcomes from breast conservation therapy for early breast cancer. We believe that the reported incidence is underestimated due to lack of reporting. Awareness of the condition, early diagnosis and early intervention may reduce treatment related morbidity in a significant number of patients. Diagnosis with histopathological testing early in the inflammatory phase is preferred as early modulation of this inflammatory response results in improved outcomes [16]. Histopathology features include pronounced thickening of the dermis and fibrosis extending into the underlying fat with panniculitis and pronounced perivascular inflammation [4]. Alternative diagnoses need to be excluded, most importantly recurrence in the form of lymphangiosis carcinomatosa cutis. Another differential diagnosis is late onset radiodermatitis that affects up to 95% of patients following radiotherapy [17] which presents with erythema, dry and moist desquamation, fibrosis (10%), telangiectasia (10%), atrophy (8%) and pain (2%) [18].
Disease severity, persistence and progression dictates treatment with new lesions. When morphea is diagnosed, initial treatment with topical calcipotriene, a Vitamin D derivative, or tacrolimus, a topical immune modulator is recommended. Phototherapy has also been suggested, however as yet robust data is lacking [19]. If initial local treatments do not prove effective in halting the process, then systemic immunosuppression with methotrexate or systemic corticosteroids is recommended [14]. Once the inflammatory phase has settled there is no evidence for systemic therapy. Reports of surgical reconstruction for morphea demonstrates good cosmesis [20] but it is unknown if in the setting of radiation induced disease that this has the potential to reactivate the inflammatory phase [14]. This case report has aimed to highlight a poorly recognised and probably undertreated condition that has a long-lasting impact on patients. We believe that with early recognition and intervention outcomes be improved. Further prospective research of pathophysiology and treatment is required.
Declarations
Data availability: The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Consent: Written informed consent was obtained from the patients for publication of this case report and any accompanying images.
Conflict of interest: The authors have no conflicts of interest to declare.
Funding statement: No funding was received for conducting this study.
References
- World Health Organisation - International Agency for Research on Cancer. Latest global cancer data. GLOBOCAN database. 2018: 263.
- Fruchter R, Mazori D, Femia A. Epidemiology and treatment of post irradiation morphoea: A retrospective analysis from a large tertiary care center. Journal of the American Academy of Dermatology. 2016; 74: AB81.
- Partl R, Regitnig P, Tauber G. Pötscher, M. Bjelic-Radisic, V and Karin S. Radiation-induced morphea—a rare but severe late effect of adjuvant breast irradiation. Case report and review of the literature. Strahlenther Onkol. 2018; 194: 1060–1065.
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), Darby S, McGale P, Correa C, Taylor C, Arriagada R, et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet. 2011; 378: 1707-16.
- Leitenberger J, Cayce R, Haley R, Adams-Huet B, Bergstresser P, Jacobe H. Morphea subtypes are distinct autoimmune syndromes: A review of 245 adult and paediatric cases. Arch Dermatol. 2009; 145: 545-550.
- Dyer B, Hodges M, Mayadev J. Radiation-Induced Morphea: An Under-Recognized Complication of Breast Irradiation. Clinical Breast Cancer. 2016; 16: e141-e143.
- Schaffer J, Carroll C, Dvoretsky I, Huether M. Postirradiation morphea of the breast presentation of two cases and review of the literature. Dermatology. 2000; 200: 67-71.
- Colver G, Rodger A, Mortimer P, Savin J, Neill S, Hunter J. Post-irradiation morphoea. Br J of Dermatology. 1989; 120: 831-5.
- Peterson LS, Nelson AM, Su WP, Mason T, O’Fallon WM, Gabriel SE. The epidemiology of morphea (localized scleroderma) in Olmsted County 1960-1993. J Rheumatol. 1997; 24:73-80.
- Saracino A, Denton C, Orteu C. The molecular pathogenesis of morphoea: from genetics to future treatment targets. British Journal of Dermatology. 2016: 177.
- Ardern-Jones M, Black M. Widespread morphoea following radiotherapy for carcinoma of the breast. Clin Exp Dermatol. 2003; 28: 160-2.
- Ihn H, Sato S, Fujimoto M, Kikuchi K, Takehara K. Demonstration of interleukin-2, interleukin-4 and interleukin-6 in sera from patients with localized scleroderma. Arch Dermatol Res. 1995; 287: 193.
- Fett N, Werth V. Update on morphea: part I. Epidemiology, clinical presentation, and pathogenesis. J Am Acad Dermatol. 2011: 64: 217-28.
- Spalek M, Jonska-Gmyrek J, Gałecki J. Radiation-induced morphea - A literature review. J Eur Acad Dermatol Venereol. 2015; 29: 197–202.
- Ardern‐Jones M, Black M. Widespread morphoea following radiotherapy for carcinoma of the breast. Clinical and Experimental Dermatology. 2003; 28: 160-162.
- Zwischenberger B, Jacobe H. A systematic review of morphea treatments and therapeutic algorithm. J Am Acad Dermatol. 2011; 65: 925-41.
- Singh M, Alavi A, Wong R, Akita S. Radiodermatitis: A Review of Our Current Understanding. Am J Clin Dermatol. 2016; 17: 277.
- Harper J, Franklin L, Jenrette J, Aguero E. Skin toxicity during breast irradiation: Pathophysiology and Management. Southern Medical Journal. 2004; 97: 989-993.
- Hassani J, Feldmann SR. Phototherapy in Scleroderma. Dermatology and Therapy. 2016; 6: 519-553.
- Dancey, A. Waters, R. Morphea of the breast. Two case reports and discussion of the literature. J Plast Reconstr Aesthet Surg 2006, 59: 1114-1117.
