
Open Access, Volume 11
Primary fixation and soft tissue management of open war injuries in Gaza: A case series
Brandon Lim1; Lina Abu Heen2; Ruba Mussallam2; Mohammed Shaalan3*
1School of Medicine, Trinity College Dublin, Dublin, Ireland.
2School of Medicine, Islamic University of Gaza, Palestine.
3Tallaght University Hospital, Dublin, Ireland.
Mohammed Shaalan
Tallaght University Hospital, Dublin, Ireland.
Email: shalan_6@yahoo.com
Received : March 19, 2025,
Accepted : April 10, 2025
Published : April 15, 2025,
Archived : www.jclinmedcasereports.com
Abstract
War-related injuries due to high-energy trauma from mines, gunshots, and bombs are responsible for many musculoskeletal injuries and disability. Medical missions to war-torn regions provide valuable insight to improve the understanding and practices regarding the management of these injuries. This case series describes 7 cases of open fractures seen by one orthopaedic surgeon (MS) during his volunteer mission to Gaza. Patients often sustained multiple injuries given the mechanism of trauma. Cases were managed with varying methods of primary fixation and soft tissue repair. This case series aims to shed light on the extent of war-related injuries seen in Gaza and share how such injures may be managed in resource-limited environments while ensuring patient safety and maximising positive outcomes.
Keywords: War; Conflict; Trauma; Open fractures; Primary fixation.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Shaalan M (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Lim B, Abu Heen L, Mussallam R, Shaalan M. Primary fixation and soft tissue management of open war injuries in Gaza: A case series. Open J Clin Med Case Rep. 2025; 2342.
Introduction
War-related injuries seen in conflict zones such as the Gaza Strip are a serious public health concern due to management challenges that arise from a lack of resources, infrastructure, electricity, and medical supplies coupled with overburdened healthcare systems [1,2]. Although high-energy war-related injuries often require a collaborative ortho-plastic management strategy with the orthopaedic surgery team managing the initial trauma and stabilizing the fracture, and the plastic surgery team managing debridement, wound closure, skin grafting, or tissue transfer, the scarcity of plastic surgeons in under-resourced conflict zones result in the sole reliance on orthopaedic surgeons in managing war injuries [2]. Herein we present a series of 7 cases of open fractures, often presenting in a polytraumatic picture, seen by one orthopaedic surgeon (MS) during his volunteer mission to Gaza. These were cases of civilian casualties admitted to the Emergency Department (ED) of the European Hospital in Gaza during the Israel-Hamas War.
Case 1
A 23-year-old female was admitted to the Emergency Department (ED) with an isolated Gustilo IIIB open fracture of the right tibia after a neighbouring house was bombed (Figure 1A). She was resuscitated in the ED, given IV Ceftriaxone antibiotics and underwent irrigation and debridement of the wound. She was taken to theatre within 12 hours for proper wound debridement, Intramedullary Nail (IMN) fixation (Figure 1B) and wound coverage with a local flap and Split-skin thickness Skin Graft (SSG). Her post-operative course was uneventful and the wound was found to be healed within three weeks. She was subsequently allowed to mobilise with partial weight-bearing.
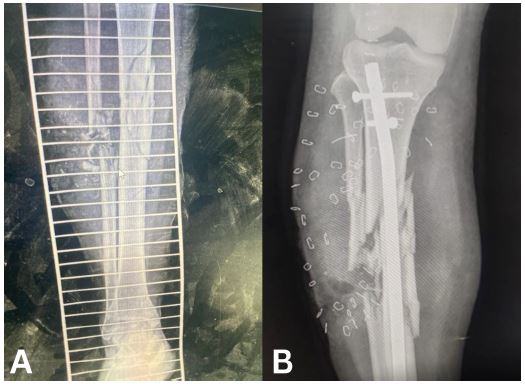
Figure 1: (A) Anteroposterior view radiograph of the right leg showing comminuted fractures of the tibia and fibula. (B) Anteroposterior view radiograph of the right leg with intramedullary nail fixation of the fracture.
Case 2
A 43-year-old male presented with multiple injuries sustained from a bomb explosion. He had a head injury and a Glasgow Coma Scale (GCS) score of 8, a chest injury with haemopneumothorax, and a Gustilo-Anderson Grade IIIB open fracture of the right proximal humerus with no signs of neurovascular injury of the right upper limb. He was intubated in the ED and subsequently underwent a craniotomy, bilateral intercostal chest tube insertions, and Open Reduction Internal Fixation (ORIF) of the humerus. This ORIF failed due to an inappropriate plate length and was later revised on another occasion with the correct plate followed by soft tissue repair and covering of the bone and plate with a SSG. The intercostal tube was removed after 6 days. He was admitted to the Intensive Care Unit (ICU) for 4 weeks after which weaning from mechanical ventilation was successful and he was transferred to a normal word.
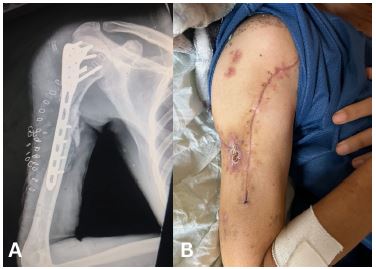
Figure 2: (A) Anteroposterior view radiograph of the fracture and internal fixation. (B) Clinical photograph of the healed wound.
Case 3
A 22-year-old male presented with a traumatic brain injury, a right-sided haemothorax, and a Gustilo-Anderson Grade III open fracture of the right proximal humerus caused by a gunshot injury. The patient received intercostal tube drainage and underwent ORIF (Figure 3A), primary wound closure, and received a course of IV Ceftriaxone. He was admitted to the ICU for 3 weeks and the wound was found to have healed by week 2 (Figure 3B). Unfortunately, the patient failed trials of extubation and passed away on week 4.

Figure 3: (A) Anteroposterior view radiograph of the comminuted fracture of the right proximal humerus with plate and nails visible in situ. (B) Clinical photograph of the healed wound.
Case 4
An 18-year-old female presented with a penetrating gunshot wound, entering her back and exiting from her left axilla, and a Gustilo-Anderson Grade IIIB open fracture of her left humerus. A chest tube was inserted in the ED after resuscitation and she was immediately taken to the operating theatre for a wash out of the wound and soft tissue reconstruction. After primary wound closure, IMN fixation was carried out using a retrograde 4.5 mm elastic nail. Her postoperative course was uneventful and the wound was found to have healed by the time of her 2-week follow-up.
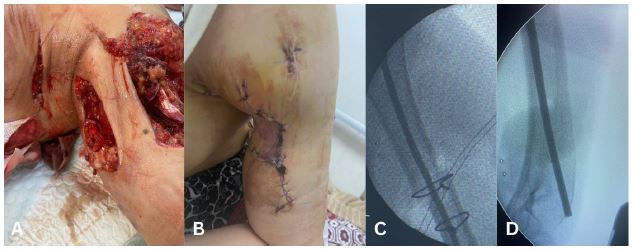
Figure 4: (A) Clinical photograph of the initial soft tissue injuries to the chest and upper arm. (B) Clinical photograph of the healed wound. (C, D) Flexible intramedullary nail visible along the length of the humerus.
Case 5
An 18-year-old male presented with fractures sustained during a bombing. He had been found under the rubble of a collapsed house after the incident. He sustained a Gustilo-Anderson Grade II open fracture of the proximal tibia on the left and a closed fracture of distal tibia on the right. There was also a fibular fracture on the left. At the time of his first presentation, soft tissue was repaired and external fixators were used to stabilise the fractures on both sides. These were in place for 14 weeks during which the patient was non-weight bearing and completely bed-bound. After 14 weeks, there was no sign of bone healing on radiography (Figure 5A). Plans were made for external fixators to be removed. Due to a lack of resources and time constraints, external fixators needed to be removed and IMN fixation inserted immediately afterwards during the same session (Figure 5B). To prepare for this, he was started on a regimen of IV Ceftriaxone 48 hours prior to the removal of the external fixators. The patient began weight-bearing as tolerated 2 days after intramedullary nailing. Wounds were found to have healed two weeks after intramedullary nailing, a total of 16 weeks after his initial presentation.
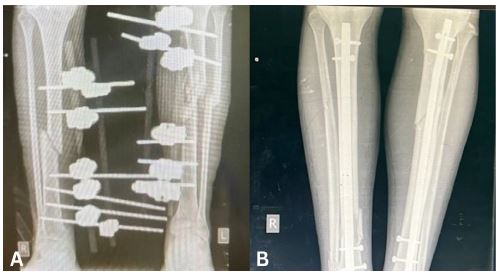
Figure 5: (A) Anteroposterior view radiograph of both legs showing external fixators in situ. (B) Anteroposterior view radiograph of both legs showing intramedullary nails in situ.
Case 6
A 38-year-old male presented with a Gustilo-Anderson Grade IIIB open comminuted fracture of the left femur after a gunshot injury. The wound underwent a washout and this was followed up by ORIF using a Trochanteric Fixation Nail (TFN) (Figure 6). This was followed by primary closure of the wound and application of Vacuum-Assisted Closure (VAC) dressing. His post-operative course was uneventful and the wound healed after 18 days. The patient was allowed to mobilise with partial weight-bearing for 3 weeks followed by full weight-bearing as tolerated.

Figure 6: Anteroposterior view radiograph of the left leg showing the trochanteric fixation nail fixation.
Case 7
A 26-year-old female presented with a Gustilo-Anderson Grade II open fracture of the right femur. She underwent external fixation for 10 weeks. IV Ceftriaxone antibiotics were given for 48 hours before removal of the external fixator. The fracture subsequently underwent closed reduction and fixation with a retrograde nail and the pin site underwent debridement. The wounds healed by week 4 and the patient was started on full weight-bearing 2 days after fixation with the nail.
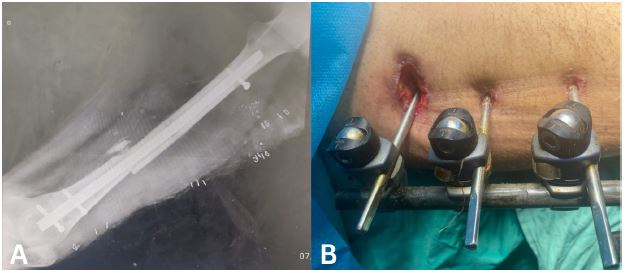
Figure 7: (A) Radiograph of external fixator. (B) External fixator and wound at week 3.
Discussion
External fixation applied within 6 hours is the ideal management of open fractures with heavy soft tissue damage soft tissues because it rapidly stabilizes bone injuries, reduces the risk of soft tissue infection, neurovascular injuries, compartment syndrome, and need for amputation, and enables easier wound and soft tissue management, delayed reconstructive surgery, safe transportation, and early rehabilitation [3]. War-related wounds are also typically treated with operative debridement and washout until wounds are ready for closure to prevent infection which are associated with serious morbidity and mortality [4]. Manojlovic et al. (2006) further emphasizes radical debridement of both the soft tissue and bone with a knife to remove dead and necrotic tissue the same way one approaches an invasive tumour [5]. A study of 41 patients with musculoskeletal blast injuries by Covey et al. (2000) concluded that early debridement, leaving wounds open, and broad-spectrum antibiotics were vital in enabling subsequent successful reconstructive surgery in an austere field setting [6]. Golubovic et al. (2010) discuss an open tibial shaft fracture caused by a shrapnel injury that was stabilised with a Mitkovic-type external fixator for five months, followed by a plaster cast for seven months, and then rehabilitation and full weight-bearing on the injured leg with a functional brace once the cast was removed and external fixator wounds were healed [7]. Maricevic and Dogas (2004) discuss an open comminuted fracture of the distal two-thirds of the tibia and fibula caused by a landmine injury managed with a split-thickness skin graft and a delta-frame external fixator for six months and physical therapy initiated during the same hospitalisation period [3]. This case was further complicated by a superficial infection that developed around a proximal Steinmann nail which was managed with antibiotics according to an antibiogram [3]. Kumar et al. (2012) describe a complex Gustilo-Anderson IIIC distal femur fracture with partial extensor mechanism loss due to a mortar blast injury managed with external fixation and soft tissue debridement followed by an extended gastrocnemius flap with skin graft to repair the wound and extensor mechanism [4]. This case was further complicated with a subcutaneous zygomycosis infection which was managed with a novel combination of local and systemic antifungals with negative pressure wound therapy with silver-impregnated sponges and antibiotic/antifungal beads [4]. However, Clasper and Phillips (2005) warn against the use of external fixation for ballistic injuries, demonstrating a high early failure rate and complication rate due to pin track infection and loosening, and amputation in their study of 18 external fixators during the Gulf conflict [8]. They further recommend plaster or skeletal traction as alternative managements while highlighting a need for multiple pins and bars when external fixation is utilised [8].
This case series brings to light the nature of injuries sustained by civilians in Gaza and the steps taken by surgeons to manage the war-related open fractures often caused by blast injuries. Although there are similar case reports/series discussing open fracture injuries in various other warzones such as Jordan [9], Kosovo [7], Croatia and Bosnia and Herzegovina [3], and former Yugoslavia [6], there has yet to be a published case report/series regarding the management of open fractures in Gaza, making this case series the first to discuss open fractures managed in the current Israel-Hamas conflict.
This case series is not without limitations. Due to the conflict, surgeons in Gaza face a shortage of appropriate instrumentations and facilities. Patients were thus treated in suboptimal conditions compared to modern Western standards. The images presented in this case series may not be the most ideal but are the best quality pictures available. Similar cases published in the literature attribute the suboptimal standard of care in the field and delayed fracture care to a lack of appropriate antibiotics, dressings, and instruments, as well as inadequate personnel training [3,9]. War injuries are complex injuries, mostly presenting as Gustilo-Anderson Grade III open fractures with significant soft tissue loss. Given the low availability of operating theatre rooms due to the high volumes of injured patients, the destruction of hospitals, and personnel being put out of work as a result of the conflict, the fix and flap is the most effective definitive management for patients who are only given a single theatre session. Furthermore, it is difficult to allocate theatre time for the further management of patients on external fixators due to new injury presentations exceeding the hospital capacity on a daily basis. This leads to a higher risk of pin loosening, pin site infections, and hypertrophic or hypotrophic non-union of the bone. Surgeons operating in conflict zones like Gaza have to thus minimise the risk of these negative outcomes in the management of open war injuries.
Ethics statement: Written informed consents for publication of the research details and clinical images was obtained from the patients or their families.
References
- Mosleh M, Dalal K, Aljeesh Y, Svanström L. The burden of war-injury in the Palestinian health care sector in Gaza Strip. BMC Int Health Hum Rights. 2018; 18: 28.
- Farhat T, Moussally K, Nahouli H, et al. The integration of ortho-plastic limb salvage teams in the humanitarian response to violence-related open tibial fractures: evaluating outcomes in the Gaza Strip. Confl Health. 2024; 18: 35.
- Maricevic A, Dogas Z. Land Mine Injury: Functional Testing Outcome. Mil Med. 2004; 169: 147-150.
- Kumar AR, Hunt P, Ritter EM, Howard R. Successful Knee Extensor Mechanism Reconstruction in a Warfare-Related Open Lower Extremity Injury Complicated by Mucormycosis Infection: A Case Report. J Orthop Trauma. 2012; 26: e7-e10.
- Manojlovic RD, Vuckovic C, Tabakovic D, Nikola G, Bumbasirevic M. Free Fibula and Corticocancellous Bone Grafting for Salvage of a War-injured Forearm. J Orthop Trauma. 2006; 20: 495-498.
- Covey DC, Lurate RB, Hatton CT. Field Hospital Treatment of Blast Wounds of the Musculoskeletal System During the Yugoslav Civil War. J Orthop Trauma. 2000; 14: 278-286.
- Golubovic Z, Vidic G, Trenkic S, et al. Treatment of open tibial shaft fracture with soft tissue and bone defect caused by aircraft bomb: Case report. Srp Arh Celok Lek. 2010; 138: 510-514.
- Clasper JC, Phillips SL. Early Failure of External Fixation in the Management of War Injuries. J R Army Med Corps. 2005; 151: 81-86.
- Pierce TP, Issa K, Rifai Y, Szczech B, Rifai A. Medical Missions in the Middle East: An Orthopaedic Surgeon’s Experience of a Series of Lower Extremity Cases. Surg Technol Int. 2017; 30: 329-335.
