
Open Access, Volume 11
Electrocardiographic changes related to pneumothorax
Akira Egami, MD1; Hirofumi Kawamata, MD, PhD1; Hikaru Nishikawa, MD2; Tatsuya Kawasaki, MD, PhD1*
1Department of Cardiology, Matsushita Memorial Hospital, Osaka, Japan.
2Department of Respiratory Medicine, Matsushita Memorial Hospital, Osaka, Japan.
Tatsuya Kawasaki
Department of Cardiology, Matsushita Memorial Hospital, Sotojima 5-55, Moriguchi, Osaka 570-8540, Japan.
Tel: +81-66992-1231, Fax: +81-66992-4845;
Email: Kawasaki.tatsuyta001@jp.panasonic.com
Received : March 18, 2025,
Accepted : April 04, 2025
Published : April 15, 2025,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Kawasaki T (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Egami A, Kawamata H, Nishikawa H, Kawasaki T. Electrocardiographic changes related to pneumothorax. Open J Clin Med Case Rep. 2025; 2340.
Short Report
A 78-year-old man presented with intermittent chest discomfort. He had a history of surgery for colon cancer and hypertension and was taking amlodipine 5 mg daily and valsartan 80 mg daily. On presentation, his vital signs and physical examination were normal. Electrocardiography (ECG) was normal (Figure 1A, brown), and echocardiography showed normal chamber sizes and left ventricular function. The patient was scheduled for Holter monitoring and exercise 201-thallium scintigraphy. On the day of the scintigraphy, he reported developing dyspnea on exertion several days earlier, prior to the start of exercise. ECG showed no ST-T segment changes (Figure 1A, green), although it was later confirmed that the R-wave height had decreased, especially in the anterolateral leads (Figure 1A, arrows).
Exercise scintigraphy was canceled, as neither unstable angina nor heart failure could be completely ruled out. The patient was transferred to the outpatient cardiology department. The jugular venous pressure was not elevated, and no abnormalities were observed on cardiac auscultation. However, respiratory sounds were diminished, and there was decreased tactile fremitus on the left side. Chest radiography demonstrated a left-sided pneumothorax (B), and computed tomography (C) revealed total collapse of the upper lobe and partial collapse of the lower lobe. Notably, air retention in the left lung cavity coincided with the leads in which the QRS amplitudes were decreased after the pneumothorax. A chest tube was placed in the left chest cavity, and the ECG returned to previous findings (Figure 1A, blue). A diagnosis of paroxysmal atrial fibrillation was later made based on Holter monitoring for his initial symptoms.
Pneumothorax can cause ECG changes, including alterations in the electrical axis, ST-segment deviations, T-wave abnormalities, and arrhythmias, although these changes vary in severity and location of the pneumothorax [1,2]. The incidence of abnormal ECG findings has been reported as 21% among 57 adolescents who presented with primary spontaneous pneumothorax [2]. Notably, only two patients had abnormal echocardiographic findings, including mitral valve prolapse and minimal mitral and tricuspid regurgitation. However, ECG abnormalities were significant, such as ST-segment elevations in five patients and inverted T waves in two patients. Serum troponin-T levels were normal in all patients.
In the present patient, the main ECG changes after pneumothorax were associated with QRS amplitude. In an ECG analysis of 40 consecutive patients with spontaneous pneumothorax by Krenke and colleagues [3], QRS amplitude in leads V2 to V6 was significantly decreased in patients with left-sided pneumothorax, while right-sided pneumothorax was associated with an increase in QRS amplitude in leads V5 and V6. The underlying mechanism remains to be elucidated, but it is intuitive to consider that QRS amplitude alterations may be attributed to the displacement of the heart within the thoracic cavity due to pneumothorax [1,4]. Given the distributions of decreased QRS amplitudes and air retention after pneumothorax in the present patient, heart displacement is the most likely cause of his ECG changes. This speculation is further supported by the fact that the ECG changes returned to previous findings after treatment for pneumothorax and that echocardiography performed before the pneumothorax was unremarkable.
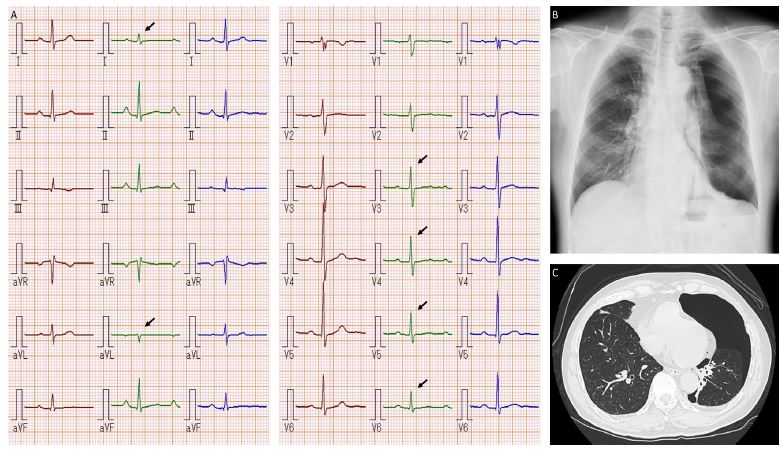
Figure 1: Clinical image.
References
- Arsh H, Iyer N, Ahmed M, Kumari V, Khan UN, Khatri CP, et al. Electrocardiographic changes in pneumothorax: an updated review. Ann Med Surg (Lond). 2024; 86: 3551-3556.
- Klin B, Gueta I, Bibi H, Baram S, Abu-Kishk I. Electrocardiographic changes in young patients with spontaneous pneumothorax: A retrospective study. Medicine (Baltimore). 2021; 100: e26793.
- Krenke R, Nasilowski J, Przybylowski T, Chazan R. Electrocardiographic changes in patients with spontaneous pneumothorax. J Physiol Pharmacol. 2008; 59: 361-373.
- McKnight CL, Burns B. Pneumothorax. 2023 Feb 15. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2025.
