
Open Access, Volume 11
Surgical management of subscapular abscess: An original case study
Abhishek Mavale1*; Riya Rathor2
1PG Scholar, Department of Shalya Tantra, Salod (H), DMIHER, Wardha (442001), India.
2PG Scholar, Department of Kaumarbhritya, Salod (H), DMIHER, Wardha (442001), India.
Abhishek Mavale
PG Scholar, Department of Shalya Tantra, Salod (H), DMIHER, Wardha (442001), India.
Email: drabhishekmavale@gmail.com
Received : December 27, 2024,
Accepted : January 23, 2025
Published : January 31, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Subscapular abscesses, localized collections of pus beneath the scapula, are uncommon but clinically significant conditions requiring timely intervention to avoid severe complications such as sepsis, chronic pain, and restricted shoulder mobility. These abscesses typically arise from trauma, hematogenous spread, or extension from nearby infections and are commonly caused by pathogens like Staphylococcus aureus and Streptococcus species. The cornerstone of management is surgical intervention, encompassing incision and drainage, debridement of necrotic tissue, and placement of drainage systems to prevent recurrence. Preoperative optimization, including managing comorbidities such as diabetes, is essential for favourable outcomes. Postoperative care involves targeted antibiotic therapy, guided by culture results, and physiotherapy to restore shoulder function and prevent adhesions. Complications such as abscess recurrence, sepsis, and adhesive capsulitis may occur, necessitating further interventions. Advancements in imaging, surgical techniques, and multidisciplinary care have significantly improved prognosis, with most patients achieving complete recovery. However, long-term follow-up remains crucial to monitor for recurrence and address residual functional impairments. This comprehensive review underscores the importance of early diagnosis, meticulous surgical planning, and postoperative rehabilitation in managing subscapular abscesses effectively.
Keywords:Subscapular abscess; Surgical management; Incision and drainage; Debridement; Imaging; Postoperative care; Adhesive capsulitis; Sepsis.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Mavale A (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Mavale A, Rathor R. Surgical management of subscapular abscess: An original case study. Open J Clin Med Case Rep. 2025; 2322.
Introduction
Subscapular abscesses are rare but serious infections characterized by localized pus accumulation beneath the scapula. These infections can result from various aetiologies, including direct trauma, hematogenous spread, or extension from adjacent anatomical structures such as the shoulder joint or ribs. While uncommon, subscapular abscesses pose significant clinical challenges due to their deep-seated location, potential for systemic involvement, and risk of complications such as sepsis, chronic pain, and restricted shoulder mobility [1,2].
The clinical presentation typically includes severe localized pain, swelling, erythema over the scapular area, restricted shoulder motion, and systemic signs of infection like fever and malaise. Accurate and timely diagnosis is critical to prevent morbidity. Imaging modalities, including ultrasound, Magnetic Resonance Imaging (MRI), and Computed Tomography (CT) scans, play a vital role in identifying the abscess, delineating its extent, and ruling out underlying conditions such as osteomyelitis [3,4].
Surgical management remains the cornerstone of treatment, focusing on incision and drainage, debridement of necrotic tissue, and the elimination of infectious foci. Adjunctive therapies, including targeted antibiotic regimens and physical rehabilitation, are essential to optimize recovery and minimize complications [5]. Recent advancements in surgical techniques and imaging technologies have significantly improved patient outcomes, underscoring the importance of a multidisciplinary approach in managing this condition.
This review aims to provide a detailed overview of the aetiology, clinical features, diagnostic strategies, and surgical management of subscapular abscesses, emphasizing evidence-based practices and addressing potential complications for improved patient care.
Case Report
AA 49-year-old Female reported of a wound with pus discharge for two months at our hospital. The patient had no previous medical history of fever, but there was a history of being pricked by an unidentified item while working on the farm, and the wound was extremely poorly cleaned thereafter. A record of discomfort, pus discharge, foul smell, development of slough, and mild oedema was present. There were no exacerbating or aggravating circumstances. She diagnosis of Abcess over back near subscapular region was made based on the patient’s history and a local inspection. The patient’s medical history was not especially significant. The patient was under stress because of the skin discolouration and ongoing itching. which caused insomnia. There was no evaluation of genetic predisposition. No prior surgical experience; no history of medicinal sensitivities. In the past, there were no cases of diabetes, hypertension, cancer, or metabolic problems. Prior to August 2024, the patient was in good condition. However, he later discovered a small pus-filled wound in his right foot’s medial malleolus, along with some minor discomfort and itching. It finally grew large and covered the entire medial ankle area in two months. Most of these lesions broke out at night. However, he declined the advice of a physician. After two months, the wound got worse, so he came to our Ayurvedic Hospital for advice. The patient was encouraged to wear regular dressings and was prescribed oral and topical Ayurvedic remedies (the patient does not recall the names of the medicines). The patient-maintained treatment at the Ayurvedic Hospital for six months after noticing improvements in the first week.
Local examination
Inspection: The abscess was located over back the left sided sub scapular region. On the first visit, the ulcers measured 5 cm by 4 cm, respectively, and were oval in shape, 10 mm to 12 mm deep, with a sero-purulent discharge that was usually shallow, with irregular slopping edges and fibrotic margins. The floor consisted of fibrinous exudate and unhealthy granulation.
Palpation: On palpation, there was tenderness but no active bleeding. There was no lymphadenopathy. Base had a little induration.
Lab investigations:
HIV-Negative
HbsAg-Nonreactive
Hb- gm%,
TLC-10700/cumm,
DLC-
N-60%
E-03%
L-32%
M-05%
B-00%
RBS-112 mg/dl
LFT-Within normal limit
KFT- Within normal limit (shows a urine examination with glucose present along with mild pus cells and epithelial cells.)
Final diagnosis: Subscapular Abscess
Treatment timeline
Table 1: Timeline.
| Date | Patients’ complaints | Interventions |
|---|---|---|
| 7 Sept to21 Oct 2024 | On the first visit, the ulcers measured 5 cm by 4 cm respectively, and were oval in shape, 10mm to 12 mm deep, with asero-purulent discharge that was usually shallow, withirregular slopping edgesand fibrotic margins. The floor consisted of fibrinous exudate and unhealthy granulation as seen in Figure 1. | Start with surgical management by incision and drainage withcurettage whole puspockets, and formhealthy wound. |
| Ayurvedic internal medications for Vranaprakshalana was done twice aday by Panchawalkalaqwath for 45Days. | ||
| Neem oil used locallyfacilitates the completion of Vranasodhana and Vranaropana activities. | ||
| Dressing was done withsterile gauze andbandage. |
Treatment had been provided by Sthanika and Abyanatara Shodana/Shamana Chikitsa. Vranaprakshalana was done twice a day by Panchawalkalaqwath. Neem oil used locally facilitates the completion of Vranasodhana and Vanaropana activities. Dressing was done with sterile gauze and bandage. This process was continued for 6 months regularly.
Table 2: Treatment protocol.
| Date | Interventions | Dosage | Adjuvant | Duration |
|---|---|---|---|---|
| 7 Sept 2024 | Tab. Cefibact | 200 mg BD | Water | 5 days |
| Tab. Pantop | 40 mg OD | Water | 5 days | |
| Tab. Emanzen DP | 400 mg BD | Water | 5 days | |
| 13 Sept 2024 | Tab. Cefibact | 200 mg BD | Water | 5 days |
| Tab. Pantop | 40 mg OD | Water | 5 days | |
| Tab. Emanzen DP | 400 mg BD | Water | 5 days | |
| 15 Sept 2024-Oct 21 2024 | Tab. Triphala Guggulu | 500 mg BD | Luke warm water | 36 days |
| Tab. Aarogyavardini vati | 500 mg BD | Luke warm water | 36 days | |
| Tab Kaishor guggul | 500 mg BD | Luke warm water | 36 days | |
| Mahamanjistha qwath | 10 ml (4tsp) | Luke warm water | 36 days | |
| 30Sept 2024-21 Oct2024 | Yasti Madhu ghrit | Local application | - | 21 days |

Figure 1: DAY-01ST.
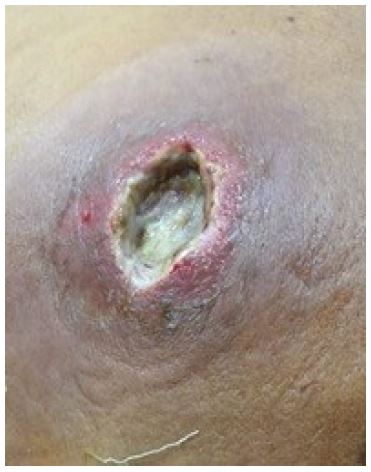
Figure 2: DAY-07TH.

Figure 3: DAY-15TH.

Figure 4: DAY-30TH.

Figure 5: DAY-45TH.
Pathya (dietary and lifestyle changes recommended): The patient was placed on a strict vegetarian diet and instructed to stay away from curds, spicy foods, brinjal, green chiles, puttu, idli, and sambar. Foods that were sour, pungent, or too salted were also forbidden. She was told to include natural, readily digested items in his diet that don’t trigger allergies. Avoiding daytime sleep, eating regularly, staying up late at night, and using irritating cosmetics were among the lifestyle changes advised. This was the recommended diet for both episodes. In contrast, the second episode had improved patient compliance.
Observation & Results
Pain from the lesions subsided immediately, which the patient could appreciate. Within a day of using Panchawalkal qwath dhavan and nim oil topically, the pain began to lessen in severity. The patient also noted that after beginning oral Ayurvedic therapy, no new lesions developed. This is a noteworthy outcome. The patient also said that stress was decreased since the skin returned to its typical texture and look (Figures 1-5). New, healthy tissue began to grow at the wound site, reducing the amount of detrimental granulation tissue that had previously formed in the slough. The wound’s size was much diminished. The wound had healed to a normal skin level, leaving the depression region gone.
Discussion
Triphala Guggul: The formulation of Triphala Guggulu has been shown to be effective in treating oxidative stress, hypolipidemia, piles, and inflammation. Amalaki, Haritaki, Vibhitaki, Pippali, and Guggulu make up Triphala Guggulu. The terms Virya, Vipaka, Rasa, Guna, and Karma are used to describe the medicinal advantages. The main ingredients of Triphala Guggulu are Laghu, Ruksha, Ushna, Tikshna Gunas, Tridoshahara, Shothahara karma, Tikta, Kashaya, Madhura Rasa, Ushna Virya, Katu Vipaka, and Laghu. Kapha dosha is lessened by Tikta, Kashaya Rasa, Laghu, and Ruksha Guna. Vata and Kapha doshas are reduced as a result of Ushna Virya. Tikta, Kashaya, and Madhura Rasa in the medication alleviate Pitta dosha. While its Ushna, Tikshna, Laghu Guna, and Ushna Virya decrease Srotorodha, its Laghu, Ruksha Guna, and Ushna Virya stimulate Agni. Guggulu is Arsha (piles), Arbuda (tumours), Shopha (oedema), and Kledahara (removes odding). It is also Kapha Vatahara (relieves Kapha and Vata). Because it is anti-microbial (Jantughna), it is used to treat infections. The main cause of Shotha, the Kapha Dosha, is opposed to the bitter and pungent Rasa in Guggulu. The heat potency of guggulu soothes vitiated Vata, stops Kleda from remaining at the pathogenesis site and generating blockage, or Srotorodha, and promotes wound healing. Additionally, it balances out the dryness and coldness associated with Vata (vitiated air). The bitter taste and scraping texture clear the body’s microchannels of Kleda dosha. As such, it slows down the pathogenic process and harmonises Kapha and Vata. Guggulu has antibacterial, anti-inflammatory, and wound-healing properties; it is used to treat wounds, lymphadenitis, boils, cysts, and other conditions. All the studies on the formulation and individual components of Triphala Guggulu indicate that its contents have anti-inflammatory, anti-microbial, and analgesic properties. These characteristics make this formulation a highly effective analgesic, antibacterial, and anti-inflammatory medication [6].
Aarogyavardini vati: By balancing the three doshas, Arogyavardhini vati enhances general health. The medication has little toxicological effects on the kidneys, liver, or brain. This medicine is often referred to as a fatty liver remedy and natural liver cleansing therapy. It supports equilibrium, preserves liver function, and keeps the digestive tract in good condition. The Shoshan (assimilation) of various surplus Snigdha Dravya’s (unctuous substances) that are present in the body is carried out by Arogyavardhini vati. It also performs the Raktavardhana (blood purification) and the Pathan (digestion) of Drava (liquid) and Kleda (clammy). It diminishes Snigdhatva and Dravatva in Meda Dhatu. Several adjuvants must be used with the medication in order to achieve the desired results. The medicine should never be self-medicated in order to prevent any negative side effects [7].
Kaishor guggulu: The primary uses of Kaishore guggulu are for its blood-purifying, antimicrobial, and antiallergic qualities. Kaishore guggulu helps maintain connective tissue, muscles (in fibromylegia), healthy joints (in gout), and back discomfort. It functions as a natural blood purifier, an anti-ageing skin health enhancer, and a dietary herbal supplement that can help with a variety of medical issues like diabetes and skin disorders. The pharmacological characteristics of Kaishor guggul have been the subject of a modest amount of scientific investigation. In order to further explore this formulation for Kaishor Guggul pharmacological action, this review helps the researcher [8].
Mahamanjistha qwath: This research aims to offer comprehensive details about the most popular species of medicinal plant known as Rubia cordifolia (Manjishtha). Research on modern pharmacology has shown that this plant possesses remarkable biological potential. It is firmly believed that the information provided in this paper about the usage of the plant Rubia cordifolia (Manjishtha) in Ayurvedic and folk cultures may encourage researchers to include this plant in contemporary medical treatments. This plant’s variety of phytochemicals may provide a potential source of antimicrobial, hepatoprotective, cardioprotective, and nephroprotective medications. Manjishta (Rubia cordifolia) hydrogel and alcoholic extract both have the ability to cure wounds. The ability of Rubia cordifolia to cure wounds was established in research using an excision wound model in mice. Ethanolic extract made a major contribution to the wound’s healing [9].
Panchavalkala Qwatha: Many other properties of Panchavalkala Qwatha include antiseptic, antiinflammatory, antioxidant, antibacterial, and antimicrobial properties. In Ayurveda, these properties are also said to include the capacity to facilitate Vrana ropana, or wound healing. The purpose of this research is to confirm the traditional Ayurvedic use of Panchavalkala Qwatha (PVK) in wound treatment and explore its antibacterial properties. Carefully crafting Panchavalkala Qwatha and Panchavalkala Arka is one aspect of the research. The antibacterial efficacy of Panchavalkala Qwatha and Panchavalkala Arka against Staphylococcus aureus and Escherichia coli was evaluated using the well diffusion test. Panchavalkala Qwatha possesses a significant zone of inhibition against E. Coli and S. aureus, measuring 25 mm and 28 mm, respectively. The antimicrobial efficiency is equivalent to that of ciprofloxacin, indicating strong antibacterial action. These results show that Panchavalkala Arka has little activity while Panchavalkala Qwatha has strong antibacterial activity against S. aureus and E. coli. This study provides primary evidence for Panchavalkala Qwatha’s antibacterial properties against S. aureus and E. coli. [10]. Nyagrodha (Ficus bengalensis Linn.) is said to possess the qualities of Varnya, Visarpa-daahagna, Yonidoshhruta, Vyanga Naashanama, and Raktapittavinashana by Guna Karma. Udumbar, also known as Ficus glomerata Roxb., has traits with Raktapittaghna, Ropana, and Vranashodhana. Ashvathha, whose scientific name is Ficus religiosa Linn., is a shaman who is related to Varnya, Yonivishodhana, and Raktadaaha. The traits of Raktadoshahara, Raktapittahruta, Plaksha (ficus lacor), and Murcha-pralaap-bhramanaashana. This suggests, according says traditional knowledge, that medications such as Teekshna Guna, Ushna Veerya, Katu Vipaka, Tikta, Kashaya Rasa, Laghu, Ruksha, and Kaphapittaghna have characteristics that break the Samprapti of ailments. In contrast to current beliefs, Panchavalkala contains phytochemically dominant phenolic group components, such as tannins and flavonoids, which are principally in charge of the plant’s remarkable healing and astringent capabilities, as well as immune-modulatory, antioxidant, antibacterial, and wound-purifying effects [11].
Neem oil: Sulphur is a component of nigmidin, the main ingredient in neem oil, and it possesses keratolytic, antifungal, and antibacterial qualities. In addition, it is very bitter. Neem extract has been shown to have antimicrobial action against both Streptococcus mutans and Streptococcus faecalis. Because of its various biological properties, such as those of an antioxidant, anti-inflammatory, antibacterial, antifungal, and antiparasitic, neem oil has been utilised in traditional medicine since ancient times [12]. Furthermore, because of its moisturising, anti-ageing, and regenerative qualities—properties mostly linked to it is known for its lipophilic makeup, fatty acid composition (especially oleic, palmitic, and stearic acids), and antioxidant capacity utilised in traditional Indian medicine. It’s believed to be a helpful and efficient plant-derived oil for healing animal and human wounds. For this reason, it has been demonstrated that using neem oil topically is advantageous for treating persistent wounds that refuse to heal [13].
Yasti Madhu Ghrit: Some of the primary constituents in Yashtimadhu include glabridin, hemileiocarpin, formononetin, glycyrrhizin (glycyrrhizic acid, glycyrrhizinic acid), isoliquiritigenin, hydrophobic flavonoids, hispaglabridin B, 4’-O-methylglabridin, and paratocarpin B. Compounds such as 18 B-glycyrrhetinic acid, Licochalcone A., isoliquiritin, liquiritigenin, glyciram, and others have properties that support learning and memory, fight inflammation, stimulate the immune system, reduce fibrosis, soothe allergies, lessen depression, prevent mutagenesis, and inhibit ulcerative neuropathy [14]. Yastimadhu also has the Tridoshaghna influence, indicating his potential as Vrana Ropana because of his status as Madhura Rasa, Guru Snigdha Guna, and Madhura Vipaka Dravya. Here, the main causes of Yastimadhu’s Vrana Ropana Karma are its Madhura Rasa and Guru Sangdha Guna, as the Rasa and Guna described above contain Karma in the form of Jivaniya, Vrushya, and Balya, which are all regenerable and therefore beneficial in the Vrana Ropana [15].
Conclusion
All symptoms and clinical aspects were evidently relieved by Prakshalan by Panchawalkalqwath, local neem oil application, and oral Triphala Guggulu, Arogyavardini vati, Kaishor Guggul, and Mahamanjistha qwath taken. Due to this understanding, Dusta Vrana is effectively controlled. Based on this case study, we may infer, at best, that Ayurveda holds promise for treating ulcers and varicose veins. During the course of the therapy, no serious bleeding, wound infection, or hypersensitivity occurred. The following case has been followed up for a period of 4 months with no recurrence.
Declarations
Informed consent: The patient gave their informed agreement for the publication of their de-identified medical records.
Declaration of competing interest: According to the study’s authors, there were no commercial or financial relationships that would have increased the risk of a conflict of interest. Since every clinician who worked on the case in both episodes is named as an author, there is no conflict of interest. Furthermore, the treating physician in both cases was the same chief physician.
Author contributions: Dr. AM. worked in software, methodology, and conceptualization. Dr. RR. is curating data and preparing original drafts of her writing. Dr. AM. worked in investigation and visualisation. The supervising doctor was Dr. RR. Programmes and Verification Dr. AM. is the author, and he has reviewed and edited the work.
References
- Brook I. Microbiology and management of abscesses. Infectious Disease Clinics of North America. 2008; 22: 896-900.
- Kao HK, et al. Subscapular abscesses: A retrospective study. Journal of Shoulder and Elbow Surgery. 2012; 21: 564-568.
- Long B, et al. Diagnostic ultrasound in musculoskeletal infections. Ultrasound Quarterly. 2020; 36: 234-241.
- Fritz J, et al. MRI findings in musculoskeletal infections. Radiology. 2009; 253: 681-690.
- Adams JE, et al. Surgical approaches to scapular infections. Clinical Orthopaedics and Related Research. 2012; 470: 1645-1651.
- Giannoudis PV, et al. The role of imaging in musculoskeletal infections. Injury. 2005; 36: 15-23.
- Neelam Rawat, Shuchi Mitra, Usha Sharma, Khem Chand Sharma. An overview of triphala guggulu and its ingredients. An International Journal of Research in AYUSH and Allied Systems. 2023: 10.
- Santosh Pal, A Ramamurthy, Bidhan Mahajon, Arogyavardhini Vati. A theoritical analysis. Journal of Scientific and Innovative Research. 2016; 5: 225-227.
- Amit Lathervikas Gupta, Parveen Bansal, Meeta Sahu, Kamal Sachdeva, Pankaj Ghaiye. International Journal of Pharmaceutical & Biological Archives. 2011; 2: 497-503.
- Karodi R, Jadhav M, Rub R, Bafna A. Evaluation of the wound healing activity of a crude extract of Rubia cordifolia L. (Indian madder) in mice. International Journal of Applied Research in Natural Products. 2009: 12-8.
- G Harikrishnan, Mohan S, Arunmohanan NV, Ramesh EN, Prajeesh Nath. Exploring the Antimicrobial Efficacy of Panchavalkala Qwatha and Arka, A Comprehensive Study JNR. 2024.
- Gajarmal Amit, Shende DS, Chothe. A clinical evaluation of panchavalkala-a review article, Gajarmal et al. UJAHM. 2014: 2.
- Cesa S, Sisto F, Zengin G, Scaccabarozzi D, Kokolakis AK, Scaltrito MM, et al. Phytochemical analyses and pharmacological screening of Neem oil. 2019; 120: 331–337.
- Bwala DG, Elisha IL, Habu KA, Dogonyaro BB. Kaikabo A.A. Management of surgical wounds using crude neem oil in one year old ram, A successful report. J Vet Med Anim Health. 2011; 3: 75–78.
- Korhalkar Anagha, et al. Pharmacological studies of Yashtimadhu (Glycyrrhiza glabra Linn.) in various animal models, GJRMI. 2013; 2: 2.
- Bhavamisra, Bhavaprakashanighantu. commentary by Padmashri Prof. Krushnachand Chunekar, edited by Late Dr. G.S. Pandey, Varanasi Chaukhambha Bharati academy. 2012; 62: 1–146.
