
Open Access, Volume 9
Cytolytic hypertransaminasemia and cholestasis in patients diagnosed with infectious mononucleosis by the Epstein-Barr virus: Review of cases between 2016 and 2023
Iríbar Diéguez Ion Koldobika1*; Muñoz Delgado María Encarnación2; De la Hoz Aizpuru Mikaela1; Juanicotena Gomollón Nekane2; De Alba Iriarte Beñat3
1Family Doctor, Lesaka Health Center, Navarra, Spain.
2Emergency Physician, Emergency Service-Bidasoa Hospital, Hondarribia, Gipuzkoa, Spain.
3Clinical Analyst, Clinical Analysis Service, Emergency Service-Bidasoa Hospital, Hondarribia, Gipuzkoa, Spain.
Ion Koldobika Iribar Diéguez
Lesaka Health Center (Navarra), Koskontako kalea 6, Lesaka 31770, Navarra, Spain.
Tel: 696-700052; Email: ionkiribar@yahoo.es
Received : August 28, 2023,
Accepted : September 26, 2023
Published : September 29, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Infectious mononucleosis can lead to self-limited liver disorders.
The objective is to verify if our patients diagnosed with infectious mononucleosis present these alterations, and their characteristics, in addition to providing a reference that allows a safer management, and a documentary base.
This is a retrospective, observational study of epidemiological, clinical and analytical data from patients diagnosed with infectious mononucleosis in the emergency department of Bidasoa Hospital since 2016.
82 patients have been included. 81.1% had cytolytic hypertransaminasemia, 62.7% cholestasis, 31.5% hyperbilirubinemia, and only one jaundice. Ultrasound was requested in 6 cases, 83.33% pathological. All progressed favorably in 4 weeks without specific treatment.
In conclusion, we can say that our patients diagnosed with infectious mononucleosis and its liver disorders fit the known profile. The analytical and imaging follow-up can be improved, despite which its evolution is favorable spontaneously.
Keywords: Epstein-Barr virus; Infectious mononucleosis; Transaminases; Hepatitis; Cholestasis.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Iríbar DIéguez IK (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Iríbar Diéguez IK, Muñoz Delgado ME, de la Hoz Aizpuru M, Juanicotena Gomollón N, De Alba Iriarte B. Cytolytic hypertransaminasemia and cholestasis in patients diagnosed with infectious mononucleosis by the Epstein-Barr virus: Review of cases between 2016 and 2023. Open J Clin Med Case Rep. 2023; 2122.
Introduction
The Epstein-Barr Virus (EBV) is a DNA (deoxyribonucleic acid) virus, whose only known host is man [1]. Primary EBV infection usually manifests as asymptomatically, indistinguishable from other viral infections, or as “Infectious Mononucleosis” (IMN) [2-7]. IMN is clinically characterized by the triad [1-8]: Fever, lymphadenopathy, and pharyngotonsillitis [3,6,8].
Liver involvement in IMN is found in around 90% of cases [5,7-10], and is normally characterized by a mild and self-limited elevation of transaminases [2-4,9]. Cases of elevated bilirubin are rare, as are those of frank hepatitis [3,4,7,9-11]. It can also present with: Abdominal pain, splenomegaly, hepatomegaly, asthenia, headache, arthralgia and, exceptionally, more serious complications [1,7,8].
The mechanism by which EBV causes liver damage is not known. Neither has the mechanism by which EBV is capable of producing cholestasis been established, coexisting with various theories [2,3,5].
In the case of hepatitis with cholestasis, the differential diagnosis of hepatitis caused by coinfections with other hepatotropic viruses can be considered [12].
In uncomplicated cases, the average duration of fever is two weeks [1,3,6], and the possible transaminase abnormality normalizes spontaneously in 2-4 weeks [2-4] (although there are series that report lasting up to 90 days) [5,8], so treatment is based on support measures [10].
Based on the case of a patient diagnosed with IMN with severe hypertransaminasemia and acute cholestasis, we proposed to review the IMN cases in our region, with the following objectives: To analyze whether the patients diagnosed with IMN in our area of influence had hepatitis or jaundice, if these varied depending on whether they were pediatric or adult patients, and if they follow the characteristics established in the literature, check if they had been followed up, an imaging test to assess the presence of hepatosplenomegaly and serology to rule out coinfection by other viruses, and check its evolution. And, secondarily: establishing a regional reference based not only on isolated cases but on a larger series, which allows us to deal with the management of these patients with greater safety.
Material and Methods
Retrospective, observational and cross-sectional study carried out in the Emergency Department (ED) of our reference hospital (Hospital Bidasoa, Basque Country). Said hospital cares for a population of 88,066 inhabitants of the gipuzkoan region of Bidasoaldea and navarre of Bortziriak.
Variables
In this work, the epidemiological variables were reviewed: age and sex, and clinical: presence of jaundice, as well as the analytical data referring to cytolytic transaminases: Alanine aminotransferase (GPT) and aspartate aminotransferase (GOT), and cholestatic: Gamma Glutamyl Transferase (GGT) and Alkaline Phosphatase (AP), as well as Total Bilirubin (BRT) values, both at the time of diagnosis and in its evolution in two periods: between weeks 2 and 4, and after the fourth week. The request for ultrasound and serological tests was also analyzed.
To assess the analytical results obtained, it was assumed that the normal range of the different transaminases varies depending on the age of the patient, their sex, as well as the reagent used in the analysis by each laboratory. In the Bortziriak region we work with two different laboratories: The Bidasoa Regional Hospital (HCB) for urgent pathology and the Navarra Hospital Complex (CHN) for routine analysis.
The assessment of the level of transaminases and BRT was made by expressing it according to the number of times that it multiplies the maximum limit of normality: xN.
Sample size and case selection
In order to obtain a valuable sample, taking into account the fact that most of the patients are asymptomatic and do not reach the ED, it was decided to study all the cases registered since we used the computerized registry with the diagnosis code of the International Classification of Diseases ICD 10th. Revision (2016) until May 2023.
To this end, we have reviewed the medical records of patients identified on discharge from the ED with the ICD10 code: B2790 (Infectious mononucleosis).
Statistic analysis
Categorical variables are described with frequencies and percentages (n, %). Continuous variables are presented with means and Standard Deviations (SD). For the contrast of hypotheses, the statistical software IBM SPSS version 26.0 and a confidence level of 95% have been used. As these were qualitative variables, the Chi-square and Fisher test of independence was applied. Results with a p value < 0.05 are considered statistically significant.
Ethical aspects
Approval for this study was obtained from the Gipuzkoa Health Area Research Ethics Committee (Protocol: IID-EPS-2023-01).
Results
After excluding 4 patients due to being displaced or not being able to verify if they had undergone analytical follow-up, we evaluated 82 patients diagnosed with IMN.
Divided 50% by sex, with an age range between 1-52 years, and a mean of 17.1 years (SD 1.04). By age groups, 32.9% (27) of the patients were pediatric (< 14 years) and 67.1% (55) adults.
A liver profile test was not performed on 13 patients. Of the rest, 56 (81.1%) presented elevation of cytolytic enzymes, 25.6% with figures >x10N. By age groups, these alterations were distributed in 15 pediatric patients and 41 adults (71.4% and 85.4% of those analyzed respectively), without finding significant differences (p 0.129), which were not found by analyzing only the cases with >x5N alteration (p 0.483).
In 51 cases, cholestatic transaminases were analyzed. Of them, 32 (62.7%) presented some type of alteration. In no case were these >x10N. In this case, we did find significant differences (p 0.029) between the pediatric and adult populations.
The correlation of the cholestasis transaminase alterations with the cytolysis transaminase alterations is expressed in graph 1, with a significant relationship between both variables (p 0.007) when analyzing the data separating the cases of greater and lesser cytolysis of x5N.
Twelve of the 38 patients analyzed (31.5%) presented elevated BRT. All of them (Table 1) when there were cytolytic alterations >x5N (p < 0.001)*. Only one patient out of the 82 had jaundice.
Ultrasound was performed in 6 cases, presenting splenomegaly in 5 and associated hepatomegaly in one of them (83.33% and 16.66% of those evaluated, respectively).
Hepatitis virus (HV) and Cytomegalovirus (CMV) serology was performed on 10 cases, all 10 cases being VH-negative and one of them (10%) with CMV coinfection.
In none of the three variants: Jaundice, ultrasound result and serological result, statistical significance was found in relation to transaminase levels.
The same evolutionary controls were not carried out in all cases. Before the month after diagnosis, only 3 cases maintained cytolytic transaminase levels >x5N, and beyond 4 weeks, both cytolytic and cholestatic enzymes were normal. Table 1 shows how the 32 patients with cytolytic transaminase levels > x5N have evolved.
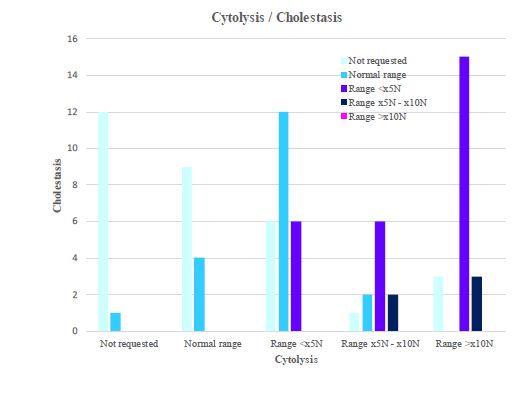
Figure 1: Relationship between cytolysis and cholestasis.
Table 1: Initial and evolutionary analysis of transaminases and bilirubin of patients reviewed in the emergency room of the Bidasoa Regional Hospital between 2016 and 2023 diagnosed with infectious mononucleosis and who initially presented cytolytic transaminase levels, elevated at least more than 5 times the high limit. of normality. Figures of evolutionary transaminases at the time of diagnosis (0), between weeks 2 and 4 after diagnosis (1), and from the first month (2) as a reflection of the recovery of baseline values. GPT (Alanine Transaminase Aminotransferase); GOT (Transaminase Aspartate Aminotransferase); GGT (Gamma-Glutamyl Transferase); AP (Alkaline Phosphatase) and BRT (Total Bilirubin) shown in figures that reflect unit/liter values for all variables, except for BRT whose values express milligrams/deciliter. The normality range from which the figures for each analysis are assessed are those indicated by the respective laboratories for each age and sex. In red letter n, the analytical values multiply by 10 or more the upper limit of the normal range; in orange letter n the analytical values between multiply the figures of the upper limit of normality between 5 and 10 times, in blue letter n the analytical values located between the upper limit of normality and figures that multiply it up to 5 times, and in green bold letter n the analytical values within the normal range. The data indicated underlined (_) have been carried out in the laboratory of the hospital complex of Navarra and therefore evaluated from the reference range established by it; the rest of the values referred to have been obtained from analyzes carried out at the Bidasoa regional hospital.
| Initial and evolutionary analysis of transaminases and bilirubin of patients diagnosed with infectious mononucleosis | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GPT0 | GOT0 | GGT0 | AP0 | BRT0 | GPT1 | GOT1 | GGT1 | AP1 | BRT1 | GPT2 | GOT2 | GGT2 | AP2 | BRT2 | |
| 1 | 160 | 63 | 25 | 0,2 | 94 | 55 | 13 | 0,4 | 16 | 21 | 8 | 0,3 | |||
| 2 | 648 | 314 | 73 | 140 | 0,4 | 310 | 89 | 55 | 111 | 0,7 | 13 | 18 | 9 | 45 | 0,5 |
| 3 | 301 | 33 | |||||||||||||
| 4 | 186 | 117 | 72 | 318 | 1,4 | 58 | 46 | 22 | 131 | 0,8 | 17 | 11 | 0,6 | ||
| 5 | 196 | 245 | 168 | 540 | 2,1 | 27 | 47 | 32 | 291 | 0,3 | 8 | 12 | |||
| 6 | 576 | 201 | 0,6 | 110 | 58 | 72 | 36 | 34 | 14 | ||||||
| 7 | 467/td> | 171 | 195 | 611 | 3.2 | ||||||||||
| 8 | 426 | 269 | 125 | 0,4 | 20 | 21 | 38 | 14 | 14 | ||||||
| 9 | 317 | 159 | 84 | 153 | 0,4 | 25 | 23 | 13 | 59 | 9 | 14 | 8 | 61 | ||
| 10 | 623 | 555 | 159 | 111 | 94 | 33 | 10 | 10 | |||||||
| 11 | 367 | 196 | 62 | 160 | 20 | 18 | 18 | 9 | |||||||
| 12 | 514 | 459 | 292 | 369 | |||||||||||
| 13 | 480 | 187 | 249 | 364 | 2,2 | 212 | 64 | 106 | 158 | 0,8 | 21 | 20 | 19 | 77 | 0,7 |
| 14 | 480 | 64 | 106 | 158 | 2,2 | 212 | 20 | 19 | 93 | 1,4 | 21 | 15 | 11 | 77 | 0,8 |
| 15 | 230 | 92 | 41 | 140 | 15 | ||||||||||
| 16 | 226 | 207 | 355 | 297 | 0,8 | 15 | 22 | 108 | 111 | 0,7 | 9 | 13 | 77 | 0,4 | |
| 17 | 562 | 49 | 209 | 75 | 64 | 36 | 51 | 50 | 20 | 27 | 21 | 41 | |||
| 18 | 270 | 115 | 466 | 3,4 | 12 | 0,8 | |||||||||
| 19 | 458 | 368 | 213 | 321 | 2,6 | 149 | 86 | 196 | 216 | 0,6 | 51 | 38 | 36 | 82 | 0,5 |
| 20 | 260 | 214 | 81 | 224 | 4,4 | ||||||||||
| 21 | 391 | 251 | 246 | 517 | 2,4 | 32 | 25 | 59 | 191 | 0,6 | |||||
| 22 | 282 | 162 | 259 | 324 | 3,8 | 31 | 27 | 59 | 131 | 0,9 | 15 | 20 | 11 | 116 | 0,9 |
| 23 | 1036 | 133 | 578 | 367 | 1,5 | 52 | 31 | 93 | 184 | 0,8 | 14 | 17> | 17 | 100 | 0,8 |
| 24 | 641 | 48 | 17 | 9 | |||||||||||
| 25 | 548 | 458 | 221 | 239 | 0,8 | ||||||||||
| 26 | 384 | 260 | 328 | 274 | 0,7 | 41 | 161 | 116 | 0,4 | 12 | 14 | ||||
| 27 | 919 | 683 | 289 | 607 | 1 | 50 | 35 | 92 | 134 | 16 | 21 | 22 | 59 | 0,6 | |
| 28 | 249 | 143 | 78 | 86 | 0,8 | 34 | 31 | 21 | 57 | 0,5 | |||||
| 29 | 476 | ||||||||||||||
| 30 | 903 | 25 | 23 | 31 | |||||||||||
| 31 | 211 | 98 | 208 | 500 | 0,6 | 16 | 19 | 51 | 145 | 0,5 | |||||
| CASE | 765 | 353 | 272 | 442 | 2,5 | 207 | 55 | 188 | 281 | 0,9 | 57 | 31 | 95 | 167 | 0,8 |
Table 2: Normal ranges with which the laboratory of the Bidasoa regional hospital works for the variable ‘alkaline phosphatase» based on the sex and age of the patient. U/L: Units/Liter.
| Alkaline phosphatase | ||
|---|---|---|
| Sex | Age | Reference range |
| Man | 0 - 0 days | 40 - 250 U/L |
| 1 - 4 days | 40 - 231 U/L | |
| 5 - 179 days | 40 - 449 U/L | |
| 180 days - 0 years | 40 - 462 U/L | |
| 1 - 2 years | 40 - 281 U/L | |
| 3 - 5 years | 40 - 269 U/L | |
| 6 - 11 years | 40 - 300 U/L | |
| 12 - 16 years | 40 - 390 U/L | |
| 17 - 999 years | 40 - 129 U/L | |
| Women | 0 - 0 days | 35 - 250 U/L |
| 1 - 4 days | 35 - 231 U/L | |
| 5 - 179 days | 35 - 449 U/L | |
| 180 days - 0 years | 35 - 462 U/L | |
| 1 - 2 years | 35 - 281 U/L | |
| 3 - 5 years | 35 - 269 U/L | |
| 6 - 11 years | 35 - 300 U/L | |
| 12 - 16 years | 35 - 187 U/L | |
| 17 - 999 years | 35 - 104 U/L | |
Discussion
Numerous isolated clinical cases evaluate liver alterations in cases of IMN, but few series, and none in our environment.
Liver involvement is normally characterized by a mild (x2N or x3N) and self-limited elevation of cytolytic transaminases (GPT and GOT), and cases of cholestasis (GGT x3N, FA x2N) have also been published [2,3,5,7]. Finding transaminase elevation figures greater than x5N is not so common [3], although there are series with elevations of x10N in 60% of cases [7]. It is more rare to find cases of frank elevation of bilirubin, although there are series that report discrete increases in up to >40% of patients [1,9].
A sample of the variability of the normal ranges provided by the laboratories with which we work in our basic health area, and which mainly affects the AF variable, is shown in Table 2.
The percentage of patients who presented cytolytic (81.1%) and cholestatic (62.7%) enzymatic alterations, as well as their distribution based on the number of times that the value multiplies the high range of normality, situates our sample in the values of mild or medium hypertransaminasemia established in most of the bibliographic references [2,3,5,7,8], being far behind, with 25.6%, the percentage of patients (61.5%) with figures of cytolytic hypertransaminasemia >x10N expressed by Prieto de Paula et al. [7].
The values of hyperbilirubinemia (31.5%), and the fact that when it occurs it is mild, and practically always without jaundice, groups our patients together with the figures expressed by other authors [5], although slightly lower in percentage than those of series such as the by González SN et al. [1].
Our isolated case of jaundice aligns our series with the values described [2,3,7-11].
According to different authors [1,6,7] the presence of splenomegaly (36-87%) and hepatomegaly (15-46%) varies greatly. The cases found in our series (83.3% and 16.6%) fall within these ranges, but with a low number of ultrasound scans requested.
From what we have observed, in most cases (87.8%) the professional is confident that the patient will not be coinfected and the results seem to confirm this impression with a single CMV coinfection in the cases in which it was evaluated.
If we observe the evolution, we verify how its evolution also corresponds to that expected according to the literature [3,7,8], even in cases with cytolytic hypertransaminasemia >x10N or moderate cholestasis.
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) are a pharmacological group implicated in toxic hepatitis (necroinflammation and cholestasis), although rare at recommended doses [2]. The “case” patient had not taken NSAIDs, although he had taken paracetamol. However, paracetamol can be excluded as an etiological agent for liver disorders in our patient, since it only causes cytolysis and damage in the form of central necrosis when its dose is excessive, and this was not the case.
The diagnosis of hepatitis may require a biopsy [13]. if there are etiological doubts or the evolution is unfavorable, something that did not occur in any of the cases reviewed.
Conclusion
Our patients diagnosed with IMN present hepatic alterations compatible with expectations, significantly more related to adulthood in the case of cholestatic ones, as well as the minimal presence of clinical jaundice.
From the low rate of imaging tests requested, despite the fact that the percentage of pathological tests falls within the expected range, we cannot draw any more conclusions from our sample than to confirm, as in the rest of the bibliographical references, that splenomegaly is more frequent than hepatomegaly.
The percentage of requested serologies is too low to confirm that the trend we see (minimum coinfection) is definitive.
The analytical and image monitoring can be improved. In both aspects, we think that professionals assume that our patients with IMN will do well regardless of whether or not they present splenic and/or hepatic abnormalities or coinfection. In this sense, although the analytical follow-up we do can be improved, the evolution of all cases is spontaneously good within the estimated period of approximately 4 weeks, even in cases with significant cytolytic or cholestatic changes.
Limitations
The fact of analyzing only the data from our referential SU, belonging to a small area, and in relation to a pathology for which patients usually do not consult at the hospital level can cause a selection bias and make the results not extrapolated to all patients with infectious mononucleosis, although we believe that the importance of this bias is less since the results of our analysis are comparable to those of other studies.
*The p-value of the chi-square test of independence is significant (p< 0.05), therefore, with a confidence level of 95% we can accept the hypothesis of dependence between the variables. However, in this case we should not do it because the assumption in which there should not be more than 25% of the cells in the crosstab with a frequency less than or equal to 5 is not met.
Declarations
- Thanks to the case patient for giving his consent and to the OSI-Bidasoa hospital assistance information service for facilitating the collection of histories.
- This work has not been financed in any way.
- The authors of this work have no conflicts of interest.
- All the co-authors have participated in the different phases of care and follow-up of the case patient, as well as in the preparation of this work.
- Partial content of the work has been sent for a possible poster type communication to the VII SEMFyC Conference on Rural Medicine.
- The work has been carried out with patients from the Lesaka Health Center and the Bidasoa Hospital emergency department, having obtained the written consent of the «case» patient and the approval by the Research Ethics Committee of the Gipuzkoa Health Area (Protocol: IID-EPS-2023-01) to carry out this analysis.
References
- González SN, Monroy CVA, Piña RG. Clinical and paraclinical characteristics of infectious mononucleosis due to Epstein-Barr virus in 162 patients at the National Institute of Pediatrics, 1970-2011. Rev Enfer Infec Pediatr. 2011; 24.25: 50-56.
- Barreales M, Pérez-Carreras M, Meizoso T, Garrido M, Masedo A, Colina F et al. Epstein-Barr virus infection and acute cholestatic hepatitis. An. Med. Interna. 2006; 23: 483-486.
- Maradiaga-Montoya RY, Izaguirre JD, Sánchez E. Epstein-Barr virus hepatitis. Med Int Méx. 2021; 37: 135-139.
- Fernández Fernández S, Centeno Jiménez M, Cilleruelo Pascual ML. Cholestasis as an atypical form of presentation of Epstein-Barr virus infection. An Pediatr (Barc). 2006; 64: 284-292.
- Losavio AD, Te HS. Epstein-Barr virus: An unusual cause of cholestatic hepatitis in older adults. Gastroenterol Hepatol (NY). 2007; 3: 101-105.
- Hernández Estrada S, Aguilar DC, Lizardi CJ. Epstein-Barr virus hepatitis: A case report. Med Sur. 2005; 12: 177-179.
- Prieto de Paula JM, Mayor Toranzo E, Franco Hidalgo S. Description of 8 cases of acute hepatitis due to Epstein-Barr virus. GastroenterolHepatol. 2012; 35: 103-105.
- Teniente Urbina ME, Casas Castañeda J, Ortiz Saavedra PJ. Pancreatitis, myocarditis and interstitial nephritis associated with acute Epstein-Barr virus infection. Rev. Gastroenterol. Perú. 2009; 29(4): 367-373.
- Modesto Dos Santos V, Da Costa Arruda Z Jr, De Farias Polcheira M, Da Silva De Souza DW, Rodrigues Oliveira Santos AM, et al. Acute hepatitis due to infectious mononucleosis in a 21-year-old man. Rev Med Chil. 2013; 141: 917-921.
- Khoo A. Acute cholestatic hepatitis induced by Epstein-Barr virus infection in an adult: A case report. J Med Case Rep. 2016; 10: 75.
- Hinedi TB, Koff RS. Cholestatic hepatitis induced by Epstein-Barr virus infection in an adult. Dig Dis Sci. 2003; 48: 539-541.
- Gómez Aldana AJ, Tapias M, Lúquez Mindiola AJ. Cholestasis in the adult: Diagnostic and therapeutic approach. Theme review. Rev Colomb Gastroenterol. 2020; 35.
- Román IV, Portocarrero GC, Ancassi AP, Silva Diaz J. Severe acute hepatitis due to coinfection by Epstein-Barr virus and Cytomegalovirus - Case report and review of the literature. Rev. Fac. Med. Hum. 2020; 20: 158-161.
