
Open Access, Volume 9
Anal squamous cell carcinoma mimicking pyoderma gangrenosum in a patient with crohn’s disease
Aikaterini Mantaka1*; Dimitra Koumaki2; Elena Komini3; Eleni Lagoudaki4; Ioannis E Koutroubakis5
1Department of Gastroenterology, General Hospital of Chania “Saint George”, Crete, Greece.
2Department of Dermatology and Venereology, University Hospital of Heraklion, Crete, Greece.
31st Health Center of Chania, Crete, Greece.
4Department of Pathology, University Hospital of Heraklion, Crete, Greece.
5University Hospital of Heraklion, Gastroenterology Department, Medical School, University of Crete, Greece.
Aikaterini Mantaka
Department of Gastroenterology, “Saint George” General Hospital of Chania, 73300, Crete, Greece.
Tel: +30-28210-22613 & +30-28210-22610; Email: katmant@gmail.com
Received : July 14, 2023,
Accepted : Aug 29, 2023
Published : Aug 31, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Anal neoplasia in Inflammatory Bowel Disease is rare and has been associated with HPV and perianal disease. We report a case of a large perianal ulcer in a patient with a non perianal Crohn’s disease that it was initially misdiagnosed and treated as pyoderma gangrenosum. After a 4-month delay, biopsies of the ulcer’s edge led to the rare diagnosis of squamous cell anal cancer
Keywords: Anal squamous cell carcinoma; Crohn’s disease; Perianal ulcer; Pyoderma gangrenosum; Inflammatory bowel disease.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Mantaka A (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Mantaka A, Koumaki D, Komini E, Lagoudaki IE, Koutroubakis IE. Anal squamous cell carcinoma mimicking pyoderma gangrenosum in a patient with crohn’s disease. Open J Clin Med Case Rep. 2023; 2104.
Introduction
The presence of large perianal ulcers is not such a usual manifestation even in patients with preexisting Crohn’s Disease (CD) [1,2].
Differential diagnosis can be challenging, including infectious etiology, autoimmune, systematic diseases, cancer and less often medications [3].
We report a rare case of anal cancer presented as a large painful perianal wound mimicking Pyoderma Gangrenosum (PG) in a patient with ileal CD and multiple other comorbidities.
Case Presentation
A 77-year-old patient with CD diagnosed on 2014, treated with periodic use of oral budesonide, was referred to our outpatient clinic due to endoscopic relapse with deep ulcers on terminal ileum on July 2019. Patient’s comorbidities included Beta Cell Chronic Lymphocytic Leukemia (BCLL), facial non-melanoma skin cancer and diabetes mellitus.
He had a satisfactory nutritional status [BMI: 27.2 kg/m2 ] and laboratory tests showed Hb: 12.8 g/ dl, MCV: 88fl, B12: 194 pg/ml (187-883)], ESR: 34, CRP:0.7 mg/dl (range 0-0.5 md/dl), ferritin: 61 ng/dl (range 25-377) and alb: 4.3 g/dl. The therapeutic decision after hematological consultation was to increase budesonide to 9 mg.
We were planning to repeat endoscopy but the restrictions due to COVID-19 pandemic led to delayed in-person physical examination. In October 2020 the patient complained of proctalgia and dyschezia. A small 3-4 mm ulceration on the dentate line next to his dilated external hemorrhoids, was noticed. The anal canal was stiff with stenosis, on digital examination. He was prescribed mesalazine suppositories. Colonoscopy was postponed again due to COVID-19 pandemic. In September 2021 he presented with a painful deep ulcerated perianal wound (Figure 1A).
An urgent ileocolonoscopy was performed showing some superficial ulcerations in the terminal ileum, with biopsies typical for CD. Anal canal was stiff, but the patient denied rectal examination under anesthesia. Perianal MRI showed a 4cm ulcerated lesion of the left perianal region extending to the anal verge, with suspicion of a fistula.
A dermatologist after excluding infectious aetiology (RPR, IGRA test, HPV, CMV, HSV, HIV serology, perianal ulcer cultures) concluded to the possible diagnosis of PG. Methyprednisolone (32mg per os) was initiated with a gradual dose tapering of 4mg every two weeks. After 5weeks, there was a 25% reduction in ulcer’s size (Figure 1B). He was then infected by SARS-CoV-2, and regular follow-up was postponed. A month later, the ulcer was again enlarged (Figure 1C). Methylprednisolone was re-increased to 24mg and doxycycline was added for 10 days, without any clinical improvement. Finally, biopsy from the perianal ulcer showed moderately differentiated anal SCC (Figure 2). A new perianal MR did not show any difference in the ulcerated lesion. A chest, upper and lower abdominal CT scan showed stable findings compared to his previous radiological evaluations for BCLL. A fecal diversion with temporal sigmoidostomy was performed before combined chemotherapy plus radiotherapy. After the completion of chemo/radiotherapy the ulcer has been reduced to about 1cm and anal canal stenosis was improved, allowing easier defecation (Figure 1D).
Discussion
Anal cancer accounts for 1-2% of digestive cancers, with SCC in 85% of cases, mainly associated with female gender, HPV, anal intercourse and smoking [4].
Annual incidence of anal SCC has been reported in 0.9/100,000 for Ulcerative Colitis and 2.0/100,000 for CD, with perianal phenotype in 85% of CD cases. IBD patients have a higher incidence of anal SCC, earlier age at diagnosis and worst outcomes [1].
PG is a rare ulcerating skin disease, associated with IBD in 30% of cases, with the anogenital region being affected less commonly [5,6].
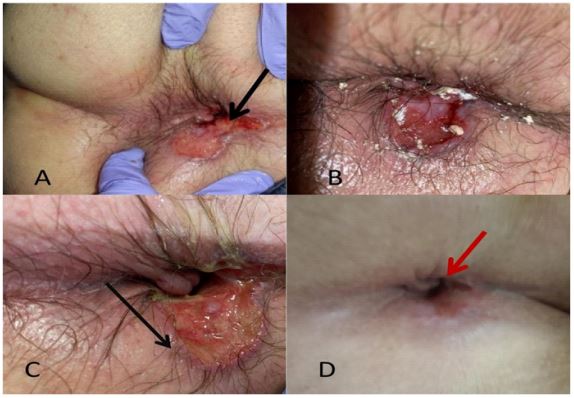
Figure 1:
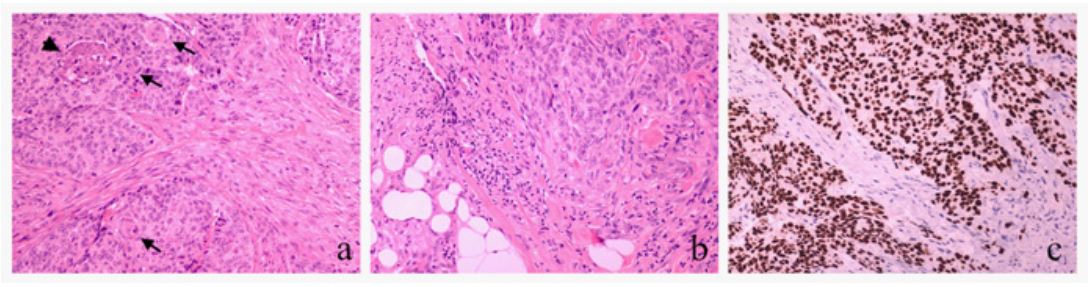
Figure 2:
Considering that PG is a diagnosis of exclusion, misdiagnosis has been reported up to 10% of cases [7]. Unperformed or non-diagnostic biopsy of the ulcer’s edge is the main reason.
In our case the unusual location of a perianal ulcer without any history of perianal CD, no HPV infection, the fear for pathergy and the initial atypical response to steroids misguided us.
“An anal fissure” or a chronic perianal fistula could have led to cancerous transformation. Alternatively, it could be a perianal SCC with extension to the anal canal [8].
Conclusions
In clinical practice, perianal region should be routinely examined in IBD patients, especially in case of pain and difficulty to defecation. A biopsy of any perianal ulcer should always be obtained to exclude even those rare cases of malignancy.
Declarations
Authors have no conflict of interest to declare
Institutional written informed consent was obtained from the patient: (including consent for social media publication)
References
- Slesser AA, Bhangu A, Bower M, Goldin R, et al. A systematic review of anal squamous cell carcinoma in inflammatory bowel disease. Surg Oncol. 2013; 22: 230-7.
- Beaugerie L, Carrat F, Nahon S, et al. Cancers et Surrisque Associé aux Maladies Inflammatoires Intestinales En France Study Group. High Risk of Anal and Rectal Cancer in Patients with Anal and/or Perianal Crohn’s Disease. Clin Gastroenterol Hepatol. 2018 ; 16: 892-899.e2.
- Egal A, London J, Lidove O, et al. Manifestations ano-rectales des maladies systémiques [Anorectal manifestations in systemic diseases]. Rev Med Interne. 2019 ; 40: 729-732.
- Wisniewski A, Fléjou JF, Siproudhis L, et al. Anal Neoplasia in Inflammatory Bowel Disease: Classification Proposal, Epidemiology, Carcinogenesis, and Risk Management Perspectives. J Crohns Colitis. 2017 ; 11: 1011-1018.
- Plumptre I, Knabel D, Tomecki K. Pyoderma Gangrenosum: A Review for the Gastroenterologist. Inflamm Bowel Dis. 2018; 24: 2510-2517.
- Ahn C, Negus D, Huang W. Pyoderma gangrenosum: A review of pathogenesis and treatment. Expert Rev Clin Immunol. 2018; 14: 225-233.
- Weenig RH, Davis MDP, Dahl PR, et al. Skin ulcers misdiagnosed as pyoderma gangrenosum. N Engl J Med. 2002; 347: 1412-8.
- Maverakis E, Ma C, Shinkai K, et al. A Delphi consensus of international experts for diagnostic criteria of ulcerative pyoderma gangrenosum. JAMA Dermatol. 2018; 154: 461-466.
