
Open Access, Volume 9
Impact of malocclusion on oral health-related quality of life in adolescent: Case report
Liviany Katiucy Lins Pinheiro1; Rebeca Cordovil Ferreira1; Lucas Francisco Arruda Mendonca1; Michele Di Benedetto1; Liliam Gusmao da Costa Florenzano1; Priscila Pinto Brandao de Araujo1; Carlos Eduarde Bezerra Pascoal2 ; Silvia Helena de Carvalho Sales Peres2; Gabriela de Figueiredo Meira1,2*
1Department of Dentistry, University Center FAMETRO, Manaus-Amazonas, Brazil.
2Department of Pediatric Dentistry, Orthodontics and Public Health, Bauru School of Dentistry, University of São Paulo, Al Octavio ´Pinheiro Brisolla 9-75, Zip Code, 17012-901, Bauru, São Paulo, Brazil.
Gabriela de Figueiredo Meira
Department of Pediatric Dentistry, Orthodontics and Public Health. Bauru School of Dentistry, University
of São Paulo, Al Octavio ´Pinheiro Brisolla 9-75, Zip Code, 17012-901, Bauru, São Paulo, Brazil.
Tel: +55-92-98141-5813; Email: gabrielameira@usp.br
Received : July 14, 2023,
Accepted : Aug 28, 2023
Published : Aug 31, 2023,
Archived : www.jclinmedcasereports.com
Abstract
This case report aimed to describe the impact of malocclusion in oral health in the quality of life in a patient in adolescence. During the anamnesis, the patient reported being ashamed to smile due to the condition of her teeth and that she was bullying at school. The Child Perceptions Questionnaire (CPQ-11- 14) was applied before and after 7 months of treatment. Treatment consisted of extraction of impacted deciduous canines for traction and distalization of permanent canines and alignment and leveling of dental arches with Rooth prescription metal brackets. After 9 months of treatment, it was possible to observe an improvement in dental crowding and better positioning of the canines in the dental arch, in addition, there was an improvement in the patient’s quality of life, as evidenced by the questionnaire. The patient is undergoing treatment and she and her guardian are satisfied with the results obtained so far.
Keywords: Malocclusion; Quality of Life; Adolescent.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Gabriela de FM (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Gabriela de FM, Liviany Katiucy LP, Rebeca Cordovil F, Lucas Francisco AM, Michele Di B, Liliam Gusamo CF, Priscila Pinto BA, et al. Impact of malocclusion on oral health-related quality of life in adolescent: Case report. Open J Clin Med Case Rep. 2023; 2103.
Introduction
Normal occlusion is one that allows masticatory efficiency without changes in functions, considered by the correct position of the teeth in the dental arch, while malocclusions are considered as deviations of the teeth, jaws and dental arches, which can cause psychosocial problems, troubles with oral functions and greater susceptibility to trauma and dental disease problems in the affected individuals [1]. As a result of the interaction of hereditary, genetic or environmental factors [2]
Quality of life is a subjective, multidimensional concept of physical, psychological and social functions, as well as a sense of subjective well-being [3]. Normally, children and adolescents with exaggerated occlusal discrepancies present a more negative perception compared to individuals without occlusal alterations or those with less expressive alterations [4].
Adequate dental occlusion is important as it promotes a good social and functional life for the patient.
In this sense, the subjective assessment of oral health should be part of clinical routine of professionals who assist children and adolescentes [5,6]. In this study, it was verified through a literature review that oral problems generate anxiety, difficulty in eating, influence self-esteem and relationships with other individuals. The authors also reported that the most used instruments in dentistry are the Child Perceptions Questionnaire (CPQ8-10), (CPQ11-14); o Child -Oral Impacts on Daily Performances; the Child Oral Health Impact Profile and the Early Childhood Oral Health Impact Scale, for age groups of 8-10 years old, 11-14 years old, for ages 11-12 years old, for children aged 8-14 years old and 2-5 years old respectively.
Diagnosis and Etiology
A 14-year-old female patient sought the Pediatric Dentistry clinic at the Fametro University Center, accompanied by her guardian, presenting as her main complaint “crooked teeth”, feeling ashamed to talk and smile around her family and friends and suffering bullying at school. Friends used to call her by nicknames and it bothered her a lot and for that reason she used to isolate herself or avoid smiling so that this kind of thing would not happen again.
In the anamnesis, the patient’s mother reported that she had difficulty extracting the patient’s deciduous teeth and, as a result, the teeth ended up in her mouth. There are no reports of hypersensitivity to medication or food, he does not make use of medications and, regarding dental treatments, he has already performed prophylaxis and dental extractions. In this first consultation, the questionnaire applied was the Child Perceptions Questionnaire (CPQ 11-14), to assess the patient’s perception of their oral health conditions, in which the patient’s dissatisfaction was noticeable.
The extraoral examination revealed a slightly convex facial profile, facial asymmetry on the left side, passive lip sealing, absence of the buccal corridor when smiling. On lateral examination, closed gonial angle, lower lip located more forward than the upper lip (Figure 1).
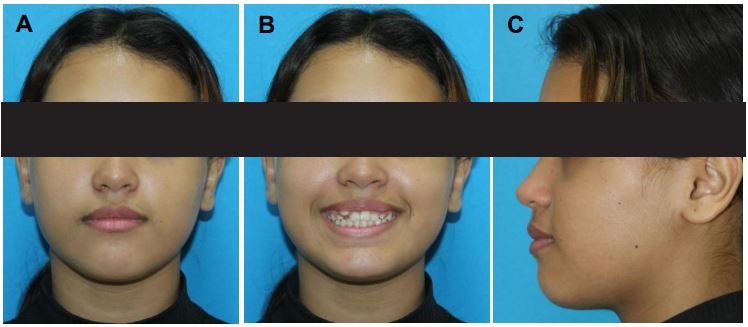
Figure 1: Panoramic X-ray, Cephalometric X-ray and Cephalometric tracing (Source: CIMO, 2022).

Figure 2: (a) Frontal view in maximum intercuspation; (b) Right side view; (c) Left side view; (d) Palatal view; (e) Lingual
view; (Source: CIMO, 2022).
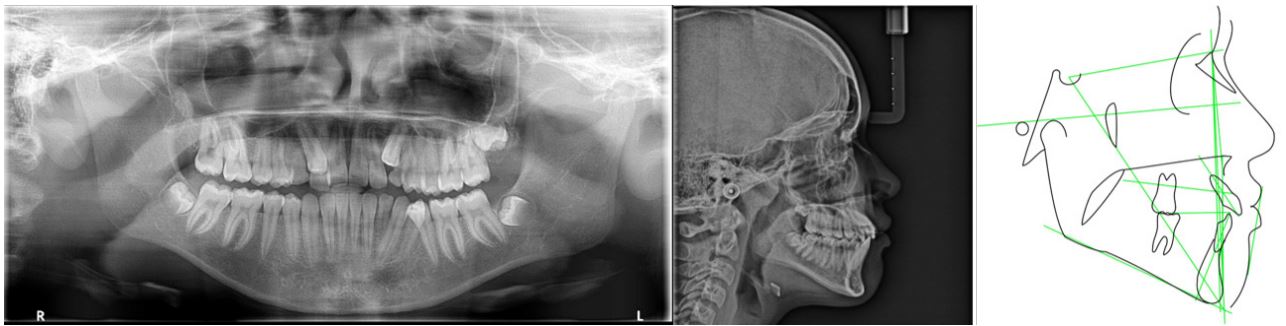
Figure 3: Panoramic X-ray, Cephalometric X-ray and Cephalometric tracing (Source: CIMO, 2022).
Table 1: Cephalometric measurements.
| Standard | Initial values | |
|---|---|---|
| SNA | 82.0 ± 2.0 | 84,556 grams |
| SNB | 80.0 ± 2.0 | 81,421 grams |
| ANB | 2.0 ± 2.0 | 3,135 g |
| FMA | 25.0 | 31.01 g |
| 1-NA | 22.0 ± 5.0 | 27,668 g |
| 1-NA | 4.0 | 5,771 mm |
| 1-NB | 4.0 | 5664mm |
| IMPA | 87.0 | 85,126 grams |
| (SN). (Go-Me) | 32.00 | 36,133 g |
Source: The author himself. Caption: SNA: Anterior and posterior position of the maxilla with the base of the skull; SNB: Anterior and posterior position of the mandible in relation to the skull base; ABN: Interference of bone bases to each other; FMA: Angle formed by the Frankfurt plane and the mandibular plane; NA: Angular positioning of the upper incisor in relation to NA; 1-NA: Linear position of the incisor in relation to NA; 1.NB: Angular positioning of the lower incisor with NB relation; 1-NB: Linear position.
In the panoramic radiograph, the contours of the floors of the right and left orbits were observed without significant alteration, well-developed maxillary sinuses, inferior nasal conchae with contours and sizes within normal limits, elements 13 and 23 are included/impacted, dental elements 28,38 and 48 are in formation, 53, 63 and 73 have prolonged retention, crowding between teeth 13/12 and 35/34. The patient’s radiography and cephalometric tracing revealed good positioning of the bone bases, configuring skeletal class I (Figure 3) and (Table 1).
Objectives of the treatment
The objective of the treatment reported in this article was: 1. To improve the harmony of the patient’s smile, since it was the main complaint; 2. Improve the patient’s quality of life; 3. Demonstrate the importance of the adolescent’s perception of their malocclusion; 4. Correct crowding and positioning of the canines, thus allowing a functional occlusion.
Alternative treatments
The patient has a class I molar interaction, according to the Angle classification, standard I facial profile and good interaction between the maxillo-mandibular bone bases, with the presence of deciduous canines 53, 63 and 73, which are suggested to have maintained space for the permanent eruption of canines ectopicly on the buccal side, so there was no consideration for orthognathic surgery, opting for the placement of fixed appliances with extraction of deciduous canines and traction of the same without the need to extract premolars to align the upper canines.
Treatment Progress
After analysis of the radiographic exams, a fixed mettalic Roth ligh from Morelli with Niti 12 wire was installed, as shown in (Figure 4). Subsequently, the orthodontic appliance was maintained with Niti 12 wire in the upper arch plus cementation of orthodontic bands in elements 16 and 26 (Figure 5), extraction of the two upper primary canines and lower left primary canine that were in prolonged retention and subsequent maintenance (Figure 6) presenting in A the third maintenance and in B was performed installation of the appliance in the lower arch plus maintenance with Niti wire 16 in the upper and lower arches, conjugated ligature from element 32 to 46, Morelli medium elastic chain from tooth 33 to 32 and bonding of teeth 13 and 23, and in C the fifth consultation with evolution of the lower Niti wire 18 with conjugated ligature of element 32 to 44, elastic chain on tooth 33 to 32, steel wire 16 in the upper arch, open spring between teeth 11 and 14 and between 22 and 24 and in D end E the subsequent maintenance until the present moment (Figure 7)

Figure 4: Installation of the metallic Roth appliance (Source: The authors, 2022).

Figure 5: Second orthodontic maintenance; (a) Front view; (b) Left side view; (C) Right Side View. (Source: The authors,
2022).
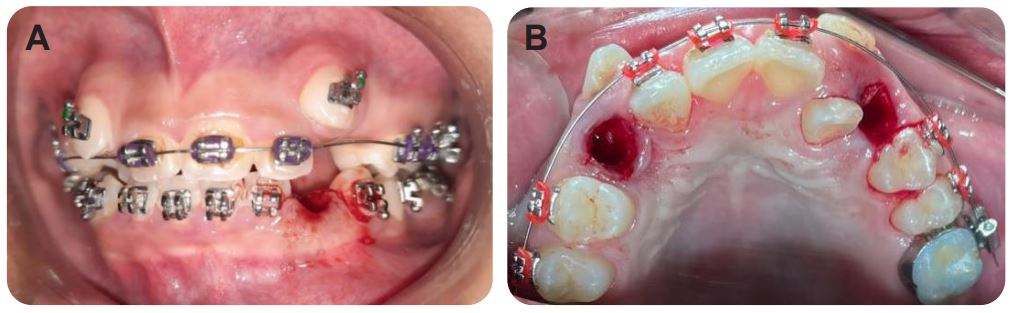
Figure 6: (a) Extraction of element 73, (b) Extraction of elements 53 and 63. (Source: The Authors, 2023).
Results
The results achieved with the treatment can be observed in Table 2, where there was an improvement in the quality of life of the patient in relation to the main complaint with the improvement of the aesthetics of the smile, in addition to that it can be observed dissolution of the dental crowding and better positioning of the canines in the dental arch. The patient is under follow-up and she and the person in charge are satisfied with the results achieved so far.
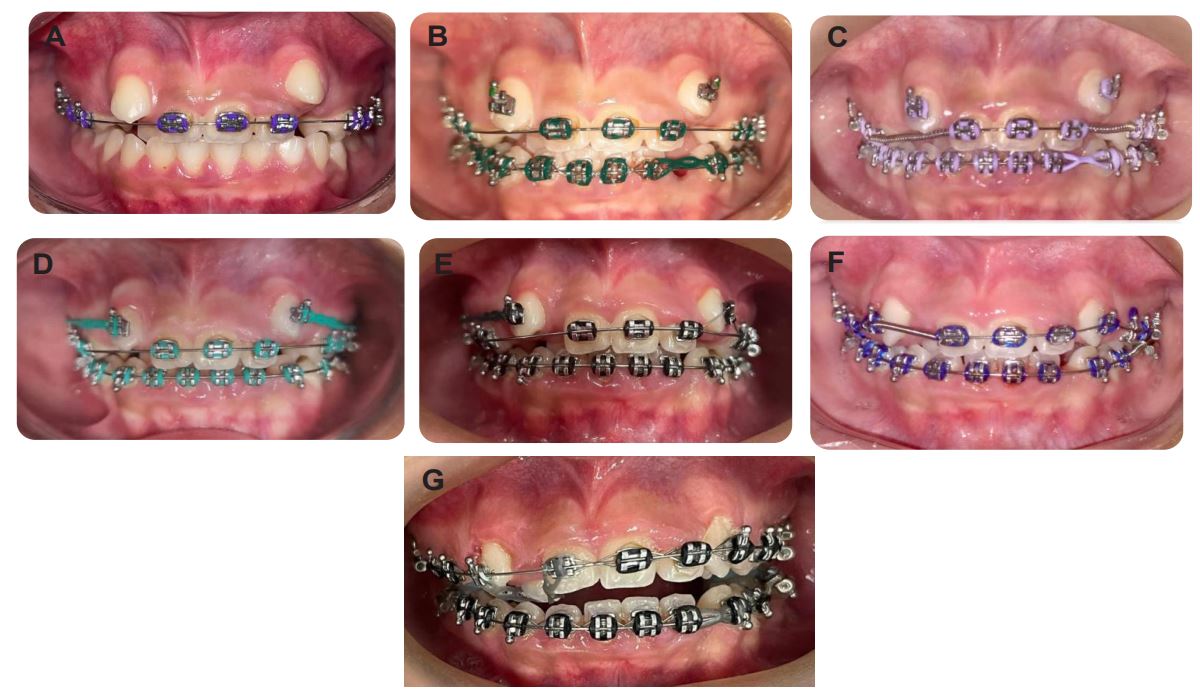
Figure 7: (a) Third visit, maintenance of the Niti 14 wire; (b) Fourth consultation, installation of the apparatus in the lower
arch; (c) fifth consultation; (d) sixth consultation; (e) seventh maintenance; (f) Eighth maintenance and the last maintenances until the presente moment in G. (Source: The Authors, 2023).
Table 2: Questionnaire (CPQ 11-14).
| CHILD PERCEPTION QUESTIONNAIRE (CPQ 11-14) | QUESTIONNAIRE 1 (2022) | QUESTIONNAIRE 2 (2023) |
|---|---|---|
| 1. How would you describe the health of your teeth, lips, jaws and mouth? | ( ) Excellent ( ) Good ( ) Fair (X) Bad ( ) Terrible | ( ) Excellent ( ) Good (X) Regular ( ) Bad ( ) Terrible |
| 2. To what extent does the condition of your teeth, lips, jaws and mouth affect your life in general? | ( ) Not at all ( ) A little ( ) Moderately ( ) A lot (X) Very | ( ) Not at all ( ) A little (X) Moderately ( ) A lot ( ) Very |
| 3. Pain in your teeth, lips, jaws or mouth? | ( ) Never ( ) Once or twice ( ) Sometimes ( ) Often (X) Every day or almost every day | ( ) Never ( ) Once or twice ( ) Sometimes (X ) Often ( ) Every day or almost every day |
| 4. Food scraps stuck in or between your teeth? | ( ) Never ( ) Once or twice ( ) Sometimes ( ) Often (X ) Every day or almost every day | ( ) Never ( ) Once or twice (X) Sometimes ( ) Often ( ) Every day or almost every day |
| 5. Did it take you longer than others to finish your meal? | ( ) Never ( ) Once or twice (X) Sometimes ( ) Often ( ) Every day or almost every day | ( ) Never ( ) Once or twice (X ) Sometimes ( ) Often ( ) Every day or almost every day |
| 6. Difficulty biting or chewing food such as apples, corn on the cob or meat? | ( ) Never ( ) Once or twice ( ) Sometimes (X) Often ( ) Every day or almost every day | ( ) Never ( ) Once or twice (X) Sometimes ( ) Often ( ) Every day or almost every day |
| 7. Difficulty saying a few words? | ( ) Never ( ) Once or twice ( ) Sometimes ( ) Often (X) Every day or almost every day | ( ) Never ( ) Once or twice (X ) Sometimes ( ) Often ( ) Every day or almost every day |
| 8. Difficulty drinking or eating hot or cold foods? | (X) Never ( ) Once or twice ( ) Sometimes ( ) Often ( ) Every day or almost every day | (X) Never ( ) Once or twice ( ) Sometimes ( ) Often ( ) Every day or almost every day |
| 9. Were you irritated or frustrated? | ( ) Never ( ) Once or twice (X) Sometimes ( ) Often ( ) Every day or almost every day | ( ) Never (X) Once or twice ( ) Sometimes ( ) Often ( ) Every day or almost every day |
| 10. Were you shy or embarrassed? | ( ) Never ( ) Once or twice ( ) Sometimes ( ) Often (X ) Every day or almost every day | ( X ) Never ( ) Once or twice ( ) Sometimes ( ) Often ( ) Every day or almost every day |
| 11. Were you upset? | ( ) Never ( ) Once or twice ( ) Sometimes (X) Often ( ) Every day or almost every day | (X) Never ( ) Once or twice ( ) Sometimes ( ) Often ( ) Every day or almost every day |
| 12. Worried about what other people think about your teeth, lips, mouth or jaws? | ( ) Never ( ) Once or twice ( ) Sometimes ( ) Often (X) Every day or almost every day | ( ) Never ( ) Once or twice (X ) Sometimes ( ) Often ( ) Every day or almost every day |
| Page 7 Vol 9: Issue 29: 2103 13. Avoid smiling or laughing when around other people? | ( ) Never ( ) Once or twice ( ) Sometimes ( ) Often (X) Every day or almost every day | ( ) Never (X) once or twice ( ) Sometimes ( ) Often ( ) Every day or almost every day |
| 14. Have you argued with other people or anyone in your fam- ily? | ( ) Never ( ) 1 or 2 times ( ) Sometimes (X) Fre- quently ( ) Every day or almost every day | ( ) Never ( ) Once or twice (X) Sometimes ( ) Often ( ) Every day or almost every day |
| 15. Have other people teased you or called you nicknames? | ( ) Never ( ) Once or twice ( ) Sometimes ( ) Often (X) Every day or almost every day | ( ) Never ( ) Once or twice (X) Sometimes ( ) Often ( ) Every day or almost every day |
| 16. Have other people asking questions about your teeth, lips, jaws and mouth? | ( ) Never ( ) Once or twice ( ) Sometimes (X) Often ( ) Every day or almost every day | ( ) Never ( ) Once or twice (X) Sometimes ( ) Often ( ) Every day or almost every day |
Source: The author himself. Caption: CPQ questionnaire [11-14] answered by the patient at the time of the anamnesis and after 6 months of orthodontic treatment.
Discussion
Malocclusions are alterations in facial patterns that affect all populations in the world, resulting in aesthetic, functional, social and psychological impairment [7,8]. According to the World Health Organization (WHO), this problem is one of the most important in oral health after caries and periodontal disease [9]. Epidemiological data show a prevalence of 39% to 93% in children and adolescents [10,11,12,7]. In our study, the adolescent patient had dental crowding, transpositions and lack of space that prevented the correct positioning of the upper canines, problems that are related to genetic factors, since the patient had little space in the dental arch associated with prolonged retentions
For Saito et al. [13], crowding, especially in Class I patients, evolves with age when neglected, given that the decrease in the width of the maxillary arch in the anterior region associated with a lingual inclination of the canines of the mandible.
Hassan et al. [14], add that dental crowding can interfere with an individual's quality of life. This is in line with what was reported by the patient in our study, as she was unhappy with the aesthetics of her smile and was a victim of bullying at school. Data that are aligned with the study of Nansel et al.[15], in which the authors report that adolescents who suffered bullying have anxiety, depression, unhappiness, loneliness and low self-esteem.
Facial musculoskeletal morphology exerts crucial activities in the establishment of human communications, be they oral, expressed by speech, visual, facial expressions, it also helps individuals to feed themselves, regulating, in this way, the functioning of the stomatognathic system, also presenting a role of protection against infectious threats and protection of sensory and encephalic organs [16]. Thus, when there is a growth variation in these facial biologic processes, comes the appearance of a covariance, which generates alterations in facial size, tooth eruption and significant impacts on the social life of its bearers, such as reduced school performance and similar [12]. As an example, in the present study, although the patient has a class I facial pattern, she has dental crowding that made her suffer bullying at school, directly impacting her educational social life and school performance.
Among the various ways of treating each malocclusion through orthodontics, there is the possibility that during treatment changes may occur in the children's quality of life [17,18]. This happens because orthodontic appliances generate speech disorders, difficulty to eat and toothache, given that these therapeutic foreign bodies press the region of the palate and surfaces of the teeth, to generate motility and thus organize the distribution of spaces in the mouth [18,19]. In our report, although the patient reported sensitivity and local pain after installation of the braces, there were no reports of major changes in her quality of life, as these symptoms disappeared after the third day of installation and maintenance of the braces.
In a review of the literature in Saudi Arabia [20] that sought to understand whether the pain triggered by orthodontic appliances could be a barrier for patients not to continue with the treatment, a result was found in agreement with that of our case report. Although starting treatment causes discomfort, this by itself is not a reason to make patients abandon treatment.
According to the Greek researchers Konstantonis et al., [21] any crowding treatment whose occlusion is in class 1 treatment has two therapeutic approaches. The first, more invasive, is tooth extraction associated with the installation of appliances and the second is conservative, adopting only the use of orthodontic appliances. However, care should be taken when indicating tooth extraction, as the authors state that incorrect indications for extractions have the potential to generate unsatisfactory aesthetic effects [22].
For the Brazilian researchers Piassi et al. [23], who aimed to investigate whether there is a relationship between malocclusions in children with mixed dentition and changes in quality of life related to oral health, through an observational study with 70 children of 8 to 10 years, found that malocclusions negatively alter the oral health quality of life of both children in mixed dentition and have a bad impact on the lives of their families.
In line with this, the Finnish researchers Närhi et al. [24], observed from a prospective study, which aimed to investigate the different levels of malocclusion and their associations with quality of life related to oral health in 1786 middle-aged adults who, in addition to the high prevalence of dentofacial alterations, there was a directly proportional association between the severity of malocclusions and quality of life related to oral health, and that women are the most affected ones by this worsening quality of life
In a cross-sectional study with 585 adolescents between twelve and fifteen years of age, which sought to assess the impact of the severity of the malocclusion associated with quality of life, it was observed that although there is an impact on the quality of life and oral health of these adolescents, the malocclusion severity had no impact on worsening quality of life indices [25].
For Prado et al. [26], who aimed to investigate how adolescent orthodontic patients perceived their malocclusions, their motivations and expectations regarding corrective orthodontic treatment through a descriptive qualitative study with 12 adolescents of 12 to 14 years old, found that interviewed patients focused their attention on unaesthetic dental and facial features that they hoped would be corrected by orthodontic management. Added to this, it became evident that many of the motivations that led young people to seek dental care were centered on the perception that friends and colleagues had about their need for treatment, thus the position of the teeth and the harmony of the smile are in close relationship with social and individual aspirations and quality of life in adolescence. These data are in line with the present report, where the patient was able to perceive her dental problem, with the negative opinion of her colleagues regarding her smile being the factor of great weight in the motivation to start and continue the orthodontic treatment.
The findings of Prado et al. [26] converge with those of Saudi researchers Ashky et al. [27] in which most participants perceived their need for orthodontic treatment. Going further, it was observed that women were significantly more aware of the awareness of their malocclusions compared to men, with socioeconomic factors being perceived as an obstacle to maintaining orthodontic treatment.
For Bendo et al. [28] in today's society, where there is consensus on the importance of good physical appearance, significant dental alterations imply emotional impacts for children and adolescents, and may have their self-esteem affected, with repercussions on their personal and social relationships.
Thus, Abreu et al. [29,30] reported that parents or caregivers play a very important role in the perception of their children's health, and this view often has a great influence on the choice of treatment, even when the adolescents themselves are able to inform their dissatisfactions. Both views can lead to different oral outcomes in the QHRSB of these adolescents.
Conclusion
With this report, it is clear that malocclusion has a negative impact on the socio-educational interaction and quality of life of patients during adolescence. Furthermore, the importance of the individuals' perception regarding their dental problem was evidenced and that orthodontic treatment is capable of improving the patient's quality of life, however with an increase in pain due to the wounds caused by the pieces of the buccal mucosa.
Conflict of interest: No potential conflicts of interest relevant to this article were reported.
References
- Pinto EM, Gondim, PPC, Lima N.S. Análise crítica dos diversos métodos de avaliação e registro das más oclusões. R Dental Press Ortodon Ortop Facial, Maringá. 2008; 13: 82-91.
- Anosike AN, Sanu OO, Da Costa OO. Malocclusion and its impact on quality of life of school children in Nigeria. West African Journal of Medicine. 2010; 29: 417-24.
- Oliveira CM, Sheiham A. Orthodontic treatment and its impact on oral health-related quality of life in Brazilian adolescentes. Journal of Orthodontics, Londres, Reino Unido. 2014; 31: 20-27.
- Castro-Cunha AC, Rebouças AP, Abreu LG, Paiva SM, Bendo. Impacto da má oclusão e do tratamento ortodôntico com aparelho fixo sobre a qualidade de vida relacionada à saúde bucal de crianças e adolescentes. Arquivos em odontologia, Belo Horizonte. 2019; 55: 9.
- Tesch FC, De Oliveira BH, Leão A. Mensuração do impacto dos problemas bucais sobre a qualidade de vida de crianças: aspectos conceituais e metodológicos. Cad. saúde pública. 2007; 23: 2555-64
- Barbosa TS, Mialhe FL, Castilho ARF, Gavião MBD. Qualidade de vida e saúde bucal em crianças e adolescentes: aspectos conceituais e metodológicos. Physis Revista de Saúde Coletiva. 2010; 20: 283-300.
- Bakes K, Kuhr K, Ohm C, Baudisch NF, Jordan AR. Does orthodontic treatment need have an impact on oral health-related quality of life?. J Orofac Orthop. 2023; 84: 19-25.
- Barros SE, Heck B, Chiqueto K, Ferreira E. Clinical predictors of potentially impacted canines in low-risk patients: A retrospective study in mixed dentition. Korean J Orthod. 2023; 53: 106-115.
- Dos Santos RR. Prevalência de Má Oclusão e Hábitos Orais Relacionados em Crianças dos 5 aos 6 Anos. Saúde Bucal Prev. Dente. 2022; 10: 311-318.
- Bauman JM, Souza JGS, Bauman CD, Flório FM. Padrão epidemiológico das má oclusões em pré-escolares brasileiros. Ciência & Saúde Coletiva. 2018; 23: 3861-68.
- Rodrigues TCA. Epidemiologia da má-oclusão no Brasil: Revisão dos aspectos etiológico e histórico. Revista Científica Multidisciplinar Núcleo do Conhecimento. Junho de. 2021; 06: 29-52
- Lone IM, Zohud O, Nashef A, Kirschneck C, Proff P, et al. Dissecting the Complexity of Skeletal-Malocclusion-Associated Fenótipos: Mouse for the Rescue. International Journal of Molecular Sciences. 2023; 24: 2570.
- Saito Y, Tanoi A, Motegi E, Sueishi K. Change in anterior crowding over 20 years from third decade of life in untreated Class I crowding. Bull Tokyo Dental College. 2019; 60: 163-76.
- Hassan AH, Hobani SM, Almokri NM, Alotibi FG, Alshouibi EN. Effect of anterior crowding or spacing on oral health-related quality of life: a crosssectional study, Patient Preference and Adherence. Jeddah. 2018; 12: 461-465.
- Nansel TR, Overpeck M, Pilla RS, Ruan WJ, Simons-Morton B, et al. Bullying behaviors among US youth: Prevalence and association with psychosocial adjustment. JAMA. 2001; 285: 2094-100
- Katz DC, Aponte JD, Liu W, Verde RV, Mayeux JM, et al. Forma Facial e Alometria Quantitative Trait Locus Intervalos na Diversidade de Camundongos Outbred São Enriquecidos para Conhecidos Genes de Desenvolvimento Esquelético e Facial. PLoS ONE. 2020; 15: e0233377.
- Jaeken K, Llano-Pérula MC, Lemiere J, Verdonck A, Fieuws S, et al. Reported changes in oral health-related quality of life in children and adolescents before, during, and after orthodontic treatment: A longitudinal study. Eur J Orthod. 2019; 41: 125-32.
- Sun L, Wong HM, McGrath CP. Association between the severity of malocclusion, assessed by occlusal indices, and Oral Health related quality of life: a systematic review and meta-analysis. Oral Health Prev Dent., 2018; 16: 211-23.
- Brouns VE, Waal AL, Bronkhorst EM, Jagtman AMK, Ongkosuwito EM. Oral health-related quality of life before, during, and after orthodontic-orthognathic treatment: A systematic review and metaanalysis. Clin Oral Investig., 2022; 26: 2223-35.
- Alrwuili MR, Alwaznah FJ, Ahmed R, Anwar S, Omar FAZ, et al. A Detailed Correlation of Oral-Health-Related Quality of Life of Patients Undergoing Fixed Orthodontic Therapy. Cureus. 2023; 15: e33854.
- Konstantonis D, Anthopoulou C, Makou M. Extraction decision and identification of treatment predictors in Class I malocclusions. Prog Orthod. 2013; 14: 47.
- Freitas BV, Rodrigues VP, Rodrigues MF, Melo HVF, Santos PCF. Soft tissue facial profile changes after orthodontic treatment with or without tooth extractions in Class 25 I malocclusion patients: A comparative study. Journal of Oral Biology and Craniofacial Research. 2018: 1-5.
- Piassi E, Antunes LS, Graça TCA, Antunes LAA. The Impact of Mixed Dentition Malocclusion on the Oral Health-Related Quality of Life for Children and Their Families: A Case-Control Study. J Clin Pediatr Dent. 2019; 43: 211-217.
- Närhi L, Talvanem M, Pirttiniemi P, Silvola AS. Malocclusion severity and its associations with oral health-related quality of life in an adult population. Eur J Orthod. 2022; 44: 377-384.
- Lacerda JA, Borges TMD, Meneguim MC, Filho MV, Júnior MS, et al. Impact of malocclusion severity on the quality of life of non-white adolescents. Cien Saude Colet. 2021; 26: 5233-5240.
- Prado LH, Previato K, Delgado RZR, Filho PN, Segato RAB, et al. Adolescents’ perception of malocclusion, their motivations, and expectations concerning the orthodontic treatment. Is it all about attractiveness? A qualitative study. Am J Orthod Dentofacial Orthop. 2022; 161: e345-e352.
- Ashky RT, Althagafi NM, Alsaati BH, Alharbi RA, Kassim SA, et al. Self-Perception of Malocclusion And Barriers To Orthodontic Care: A Cross-Sectional Study In Al-Madinah, Saudi Arabia. Patient Prefer Adherence. 2019; 13: 1723-32.
- Bendo CB, Martins CC, Pordeus IA, Paiva SM. Impacto das condições bucais na qualidade de vida dos indivíduos. Revista da Associacao Paulista de Cirurgioes Dentistas. 2014; 68: 189-93.
- Abreu LG, Melgaço CA, Abreu MHNG, Lages EMB, Paiva SM. Agreement between adolescents, and parents/caregivers in rating the impact of malocclusion on adolecents’quality of life. Angle Orthodontist. 2015; 85: 806-811.
- Hamdan AM. A relação entre a necessidade percebida do paciente, dos pais e do clínico e a necessidade normativa de tratamento ortodôntico. Eur J Orthod. 2004; 26: 265-271.
