
Open Access, Volume 9
Medial branches block at the lateral and posterior long axis articular pillar plane for chronic cervical facet joint pain: A new puncture approach?
Hongwei Fang1#; Xiuqin Yu2#; Bing Tang2; Yan Kong3 ; Zhonghua Ji2; Jinyuan Zhang2; Hao Fang1*
1Department of Anesthesiology, Zhongshan Hospital, Fudan University, Shanghai, China.
2Department of Pain and Anesthesiology, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, China.
3Department of Anesthesiology (High-Tech Branch), The First Affiliated Hospital of Anhui Medical University, Hefei, China.
#These authors contributed equally to this work
Hao Fang
Department of Anesthesiology, Zhongshan Hospital, Fudan University, No.180 Fenglin Road, Shanghai
200032, China.
Email: drfanghao72@126.com
Received : July 13, 2023,
Accepted : Aug 25, 2023
Published : Aug 31, 2023,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Fang H (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Fang H, Yu X, Tang B, Kong Y, Ji Z, Zhang J, Fang H. Medial branches block at the lateral and posterior long axis articular pillar plane for chronic cervical facet joint pain: A new puncture approach?. Open J Clin Med Case Rep. 2023; 2102.
Case Series
Cervical facet (also known as zygapophysial or zygapophyseal) joints have been concerned as the major origin of chronic posterior neck pain in approximately 26-70% cases [1,2]. Studies reported that chronic neck pain is mainly caused by C2-3 and/or C5-6 joint lesions [3], while pain in the C3 to C5 segments is affected by radiation referred pain [4,5]. Therapeutic benefit for facet joint pain has been reported with three types of interventions [6], including intraarticular injections, Medial Branch Nerve Blocks (MBBs), and neurolysis of medial branch nerves by means of radiofrequency [6-9]. Interventional therapy for joints is increasing rapidly, with 0.5% annual growth of MBBs and Intra-Articular (IA) joint injections, and 8.7% of Cervical Medial Branches (CMBs) Radiofrequency Ablation (RFA) [10]. Significant debate surrounds the appropriate management of cervical facet joint pain. However, studies showed that CMBs block may provide benefit to well-selected individuals than IA joint injections, which has also been consistent with other researches [10].
Clinically, the effect of single segment block sometimes is not satisfactory due to more than one joint segment involved in patients with chronic cervical facet joint pain [11]. This requires to block multiple articular segments from C3 to C6 according to patient’s physical examination and imaging data [11]. Anatomically, the cervical facet joints, C2-3 to C7-T1, are innervated by the medial branches derived from the dorsal rami of the cervical spinal nerve roots [12,13]. For complete block, physician need to respectively block the CMBs from C3 to C6 on the cross-section. Owing to the course of the C3 to C6 medial branches passed through the midpoint of articular pillar [14], studies have demonstrated that this correlates best with longitudinal axis ultrasound image of the vertebra where both the zygapophyseal joint and articular pillar are real-timely seen monitoring during the procedure [15,16].
We hypothesized that one-point puncture and multiple-site injections among different articular segments in the longitudinal section by moving the ultrasound probe at this level would get satisfactory block effect for patients with chronic cervical facet joint pain. We named this new puncture approach, lateral and posterior long axis articular pillar plane medial branches (LP-APMBs) puncture.
Patients who suffered from chronic cervical facet joint pain and presented to the operating room for MBBs were included in this study. Approval from the Ethics Review Committee of Shanghai East Hospital ([2021] Pre-study No. 270) and informed written consent from patients were obtained. We performed LP-APMBs puncture approach. Patients were kept in the prone position, peripheral intravenous access and routine monitoring were established. A low resolution (2-5 MHz) was selected on the linear array transducer probe (S Nerve, Sonosite, Bothell, WA, USA), a coupling agent was applied and covered with a sterile film. The marked segment was scanned in the sagittal plane. The ultrasound probe moved from the midline to the lateral image plane, namely the spinous process plane, the lamina plane and the facet plane, until the image showed the beginning of the joint column plane. We moved the probe slightly to show the clear posterolateral long axis plane of the cervical spine.
Ultrasonically guided, images of articular pillar plane segments of cervical spine 2-6 can be recognized and confirmed through cervical spine 2 joint. Prior to needle insertion, the skin was infiltrated with 2 ml of 1% lidocaine (production batch number C20A038, Shandong Hualu Pharmaceutical Co. Ltd.). A 22-gauge Tuohy needle (ASA, Shanghai, China) was inserted into the surface of the articular pillar after being guided by ultrasound. When the needle penetrates the skin, the puncture path avoids blood vessels, and the puncture process of the needle is clearly observed on the screen in real time. To verify the accuracy of puncture position, physician used 0.2 ml contrast dye and X-ray to evaluate the position of the needle tip, and considered as gold standard.
Then, 3 ml of the nerve block mixture was injected into the target position, mixture liquid 10 mL= Diprospan 1 mL (containing 5 mg of betamethasone dipropionate and 2 mg of betamethasone sodium phosphate) (production batch number 0001162870, Shanghai Schering-Plough Pharmaceutical Co. Ltd.)+0.75% ropivacaine 3 mL+0.9% NaCl 6 mL. Following, physician adjusted the probe slightly and moved the needle to the next segment keeping the needle under skin for another segment injection. We used this puncture route to avoid shoulder interference in the lateral approach, nerve block mixture was severally injected at one puncture point on the C3 and C6 longitudinal axis plane to achieve the therapeutic effect of multilevel block (Figure 1).
A total of 10 chronic cervical facet joint pain patients were followed up for the entire 3 months period. General preoperative characteristics of enrolled patients were in Table 1. In all the patients included, ultrasound-guided puncture was performed to the target by the new puncture method, and fluoroscopic imaging confirmed the accuracy of the puncture location. The Numerical Rating Scale (NRS) was seen as the primary parameter to evaluate the treatment effectiveness of this therapy. All the ten patients were asked to indicate the level of pain immediately before the session and follow-up was performed at different time points, Postoperative Day (POD), postoperative 1 week, 1 month, 3 months. Results showed that compared with the baseline scores, NRS scores were significantly decreased at different time points during the 3 months follow-up, especially at POD, PO-1 week and PO-1 month after the intervention (P<0.001, Table 2). All patients reported that discomfort symptoms such as neck distension and pain were obviously relieved, and the range of motion of cervical vertebra was greatly improved. Furthermore, no serious adverse complications were observed in all patients.
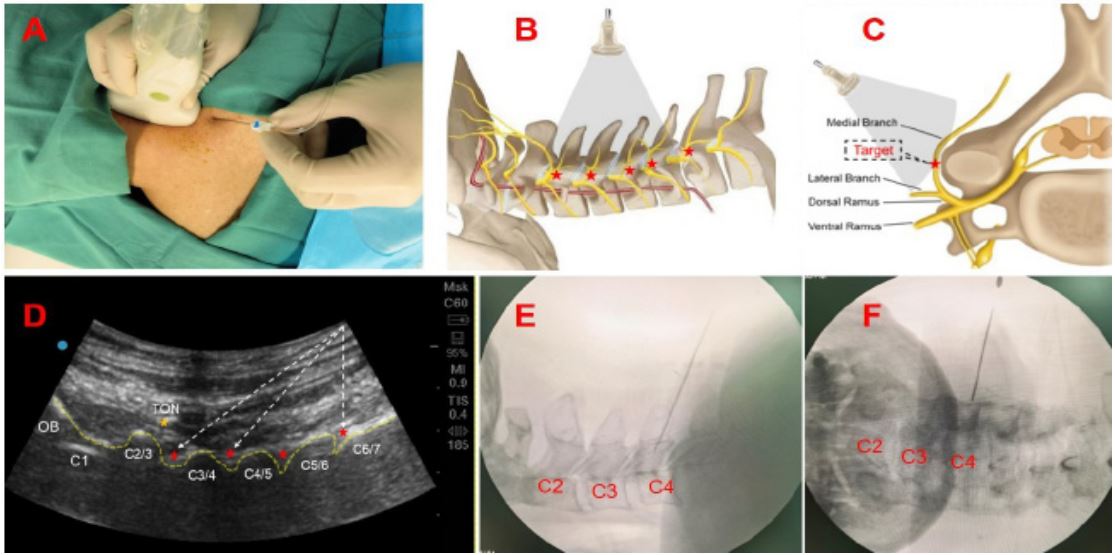
Figure 1: Schematic diagram of lateral and posterior long axis articular pillar plane medial branches (LP-APMBs) puncture,
(A) Patient was prone position, then the skin was sterilized by povidone iodine and the sterile surgical towel was placed on
the patient; (B) and (C) are the placement schematic diagrams of the ultrasonic probe on the longitudinal and transverse
axes of the cervical spine respectively. (D) Ultrasonic positioning long axis articular pillar plane, dotted line was puncture
needle route. Puncture needle was injected into the C3 and C6 longitudinal axis plane. (E) and (F) show the lateral and anteroposterior radiographs of the cervical spine under X-ray.
Abbreviations: OB: Occipital Bone; TON: Third Occipital Nerve; PN: Puncture Needle.
Abbreviations: OB: Occipital Bone; TON: Third Occipital Nerve; PN: Puncture Needle.
Table 1: General preoperative characteristics of enrol- led chronic cervical facet joint pain patients (mean ± SD).
| Patients (n=10) | |
|---|---|
| Age (years) | 42.4 ± 6.1 |
| BMI (cm2/kg) | 22.1 ± 3.0 |
| Gender (M/F) | 6/4 |
| Duration of pain (months) | 5.6 ± 2.5 |
| Preoperative symptoms | |
| Unilateral vs. Bilateral | |
| Diseased joints (C2-C7) (n) | |
| 1 | 3 |
| 2 | 4 |
| 3 | 2 |
| 4 | 1 |
| Liver function (abnormal/normal) | 0/10 |
| Renal function (abnormal/normal) | 0/10 |
Compared with traditional MBBs, we believe LP-APMBs puncture is a simple, effective and accurate puncture treatment method for complete ultrasound-guided MBBs. Of course, our sample size was small and the patients were only followed up for a period of 3 months after treatment. These are just our preliminary results, we will adopt LP-APMBs puncture method to further study, observed the clinical therapeutic effects of LP-APMBs puncture.
Table 2: Patients’ indicators after LP-APMBs puncture (mean ± SD).
| Patients (n=10) | P | |
|---|---|---|
| Number of percutaneous puncture (n) | ||
| 1 | 10 | |
| Operation duration (min) | 5.2 ± 0.5 | |
| NRS scores | ||
| Pre-operation | 6.1 ± 0.99 | |
| Post-operation | ||
| POD | 1.1 ± 0.99 | < 0.001 |
| 1 Week | 2.5 ± 1.18 | < 0.001 |
| 1 Month | 3.4 ± 1.26 | < 0.001 |
| 3 Months | 4.2 ± 0.94 | < 0.05 |
| One day Post-operation | ||
| Adverse reactions (n) | ||
| Hyperglycemia | 1/10 | |
| Hypertension | 1 | |
| Dizziness | 2 | |
| Nausea | 0 | |
| During 3 months Post-operation | ||
| Liver function (abnormal/normal) | 0/10 | |
| Renal function (abnormal/normal) | 0/10 |
NRS: Numeric Rating Scale; P < 0.001, P < 0.05 versus the Pre-operation.
Declarations
Acknowledgements: We thank all of the study participants.
Funding statement: This work was supported by Special clinical research project for health industry by Shanghai Municipal Health Commission (No. 202040007), The National Natural Science Foundation of China (81971863 and 82272230 to H. Fang).
Conflict of interest: Each author certifies that he or she has no commercial association that might pose a conflict of interest in connection with the submitted manuscript.
Declaration of competing interest: The authors declare no conflicts of interest.
References
- Speldewinde GC, Bashford GM, Davidson IR. Diagnostic cervical zygapophyseal joint blocks for chronic cervical pain. Med J Aust. 2001; 174: 174-176.
- Manchikanti L, Singh V, Rivera J, Pampati V. Prevalence of cervical facet joint pain in chronic neck pain. Pain Physician. 2002; 5: 243-249.
- Manchikanti L, Manchikanti KN, Pampati V, Brandon DE, Giordano J. The prevalence of facet-joint-related chronic neck pain in postsurgical and nonpostsurgical patients: A comparative evaluation. Pain Pract. 2008; 8: 5-10.
- Lee MJ, Riew KD. The prevalence cervical facet arthrosis: An osseous study in a cadveric population. Spine J. 2009; 9: 711-714.
- Nevalainen MT, Foran PJ, Roedl JB, Zoga AC, Morrison WB. Cervical facet oedema: prevalence, correlation to symptoms, and follow-up imaging. Clin Radiol. 2016; 71: 570-575.
- Falco FJ, Erhart S, Wargo BW, Bryce DA, Atluri S, et al. Systematic review of diagnostic utility and therapeutic effectiveness of cervical facet joint interventions. Pain Physician. 2009; 12: 323-344.
- Rubinstein SM, van Tulder M. A best-evidence review of diagnostic procedures for neck and low-back pain. Best Pract Res Clin Rheumatol. 2008; 22: 471-482.
- Manchikanti L, Boswell MV, Singh V, Benyamin RM, Fellows B, et al. Comprehensive evidence-based guidelines for interventional techniques in the management of chronic spinal pain. Pain Physician. 2009; 12: 699-80.
- Manchikanti L, Boswell MV, Singh V, Derby R, Fellows B, et al. Comprehensive review of neurophysiologic basis and diagnostic interventions in managing chronic spinal pain. Pain Physician. 2009; 12: E71-120.
- Manchikanti L, Sanapati MR, Pampati V, Soin A, Atluri S, et al. Update of Utilization Patterns of Facet Joint Interventions in Managing Spinal Pain from 2000 to 2018 in the US Fee-for-Service Medicare Population. Pain Physician. 2020; 23: E133- 133E149.
- Hurley RW, MCB A, Barad M, Bhaskar A, Bhatia A, et al. Consensus practice guidelines on interventions for cervical spine (facet) joint pain from a multispecialty international working group. Reg Anesth Pain Med. 2022; 47: 3-59.
- Bogduk N. The clinical anatomy of the cervical dorsal rami. Spine (Phila Pa 1976). 1982; 7: 319-330.
- Zhang J, Tsuzuki N, Hirabayashi S, Saiki K, Fujita K. Surgical anatomy of the nerves and muscles in the posterior cervical spine: A guide for avoiding inadvertent nerve injuries during the posterior approach. Spine (Phila Pa 1976). 2003; 28: 1379-1384.
- Kweon TD, Kim JY, Lee HY, Kim MH, Lee YW. Anatomical analysis of medial branches of dorsal rami of cervical nerves for radiofrequency thermocoagulation. Reg Anesth Pain Med. 2014; 39: 465-471.
- Won HS, Jang HY, Moon HS, Zhu PB, Kim YD, et al. Fluoroscopic Findings of Extra-Cervical Facet Joint Flow and Its Incidence on Cervical Facet Joint Arthrograms. J Clin Med. 2020; 9.
- Siegenthaler A, Mlekusch S, Trelle S, Schliessbach J, Curatolo M, et al. Accuracy of ultrasound-guided nerve blocks of the cervical zygapophysial joints. Anesthesiology. 2012; 117: 347-352.
