
Open Access, Volume 9
Avascular necrosis of the femoral head in a patient recovering from COVID-19: A case report and literature review
Jorge Guzman-Potes1*; Camilo Delgadillo1,2; Richard Bastidas1; Daniel Monsalvo3
1Department of Orthopaedics and Traumatology, Fundación Santa Fé de Bogotá, Bogotá, Colombia.
2Universidad Del Rosario, School of Medicine and Health Sciences, Bogotá, Colombia.
3Department of Hip and Knee Arthroplasty, Fundación Santa Fé de Bogotá, Bogotá, Colombia.
Jorge Guzman-Potes
Department of Orthopaedics and Traumatology, Fundación Santa Fé de Bogotá, Bogotá, Colombia.
Email: jorgeen.guzman@urosario.edu.co
Received : June 12, 2023,
Accepted : July 27, 2023
Published : July 31, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Case report of a 31 year old man affected by Coronavirus Disease 2019 (CoViD-19) requiring orotracheal intubation in prone position for several days, presenting left hip groin pain and limitation of range of motion after one year of recovery of his stay in intensive care unit, without history of previous symptoms or trauma. Following studies with imaging and clinical concordance to avascular necrosis of the femoral head pattern related to corticosteroid therapy.
Keywords: Acute respiratory distress syndrome; COVID-19; Avascular necrosis of the femoral head.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Guzman-Potes J (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Guzman-Potes J, Delgadillo C, Bastidas R, Monsalvo D. Avascular necrosis of the femoral head in a patient recovering from COVID-19: A case report and literature review. Open J Clin Med Case Rep. 2023; 2083.
Introduction
Severe Acute Respiratory Syndrome-CoronaVirus-2 (SARS-COV-2) is a contagious pathogen related to coronavirus Disease 2019 (CoViD-19), declared as a global pandemic by the World Health Organization in 2020 [1,2]. Some patients affected by CoViD-19 develop Acute Respiratory Distress Syndrome (ARDS) and may require invasive mechanical ventilation. It has been reported approximately 15% of patients affected develop pneumonia requiring any source of oxygen support and 33% of them require invasive mechanical ventilation [2].
Different line treatments have been considered for CoViD but unfortunately there is still no resolutive therapy. For many years prone position has been used to improve oxygenation in severe acute respiratory syndromes due to homogeneous distribution of stress and strain in lung tissue from dorsal to ventral in this condition, but there are no differences in lungs vascular perfusion [3]. For patients with moderate and severe ARDS from CoViD-19 is recommended this position for mechanical ventilation 12-16 hours per day [4].
Case Presentation
We report a case of a 31 years-old male, with medical history of obesity (BMI 31) and severe pneumonia by CoViD-19 previous, during hospital stay requires intravenous steroids (total dose 60 mg of dexamethasone) and immobilization secondary prostration at least one month. He consults one year later for pain in left groin and secondary limp. Physical examination showed abduction, external rotation and flexion diminished in left hip. Initial X-ray evidence areas of low density both femoral heads (Figure 1). Following study with simple Magnetic Resonance Image (MRI) (Figure 2) showed right hip with changes of necrotic bone without edema, a calculated Kerboul angle of 274o, in left hip edema and areas on necrotic bone, with an anterocentral subchrondral bone fracture of femoral head, Kerboul angle of 257º.
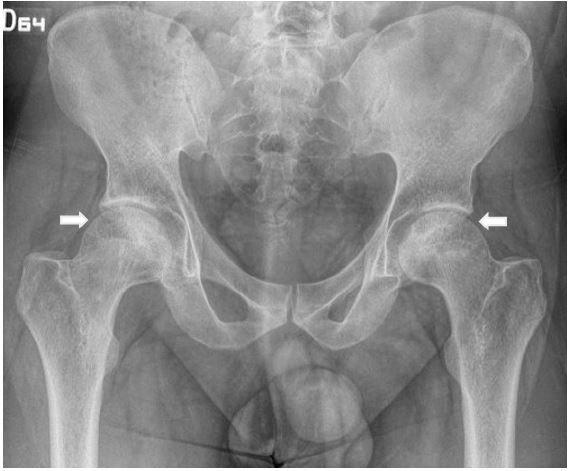
Figure 1: Bilateral hip X-ray Anterior-posterior view showing low density zones (arrows) in both femoral heads.
Following study with simple magnetic resonance imagen (MRI) (Figure 2) showed right hip with changes of necrotic bone without edema, a calculated Kerboul angle of 274o, in left hip edema and areas on necrotic bone, with an anterocentral subchrondral bone fracture of femoral head, Kerboul angle of 257o.
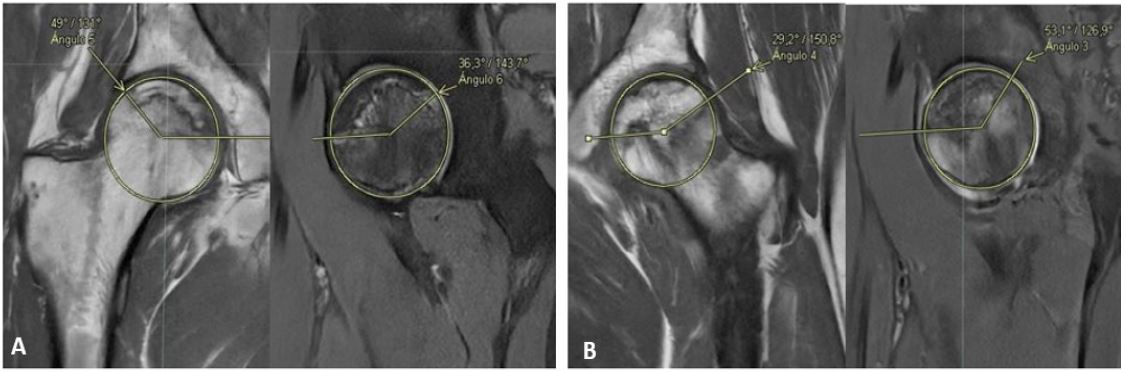
Figure 2: Bilateral hip MRI showed changes of avascular necrosis of the femoral head, with a kerboul angle of 274o on the right hip (A) and 257o on the left hip (B), associated with anterocentral subchrondral bone fracture of the femoral head.
Due to symptomatology and limp, was considered a total hip replacement for left hip, and clinical observation for right hip. The procedure was performed through a Gibson modified approach, at osteotomy of femoral head, cancellous non-vital bone was evident (Figure 3).
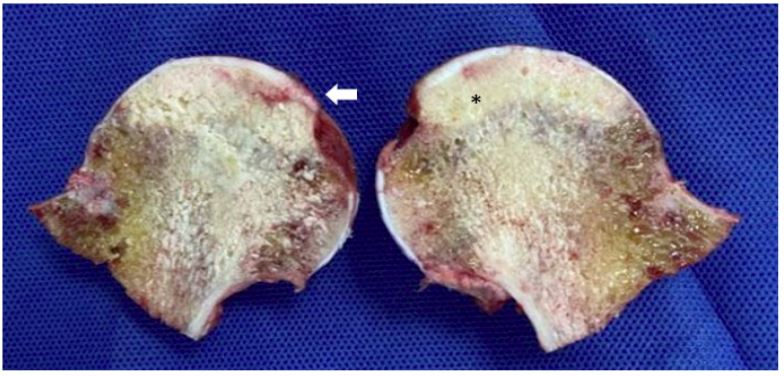
Figure 3: Anatomical dissection of the femoral head after its resection with necrotic areas (*) and subchondral fracture (arrow).
A primary total hip prosthesis with ceramic-polyethylen was used, with postoperative radiography with adequate position of the components and restoration of the offset (Figure 4).
Anatomic study confirm zones of necrotic bone with thrombosis of arteries in the medullar bone. Rehabilitation program initiated on first day postoperative. In the following days, the patient did not present acute complications, met rehabilitation goals and was discharged from hospital.

Figure 4: Postoperative Anterior-posterior hip X-ray showing left total hip artrhoplasty with ceramic-polyethylene bear surface.
Discussion
Avascular necrosis of the femoral head it is diagnosed in the United States from 20,000 to 30,000 each year, within 5% and 12% are treated with THR [5], there are possible associations that may generate this condition, including pregnancy, steroids, hematologic disorders, alcoholism; which generate thrombosis and hypo-vascularity, with secondary necrosis of the medullar bone.
With the arrival of Sars-CoViD-19 virus, the reports of steroids used in moderated and severed ill patients are increasing, showing a low frequency, but we must have in mind, like a cause in limp and groin in younger patients. There are reports about a minimum dose of steroids for ANFH, out patient received a low dose and present with bilateral ANFH. After the infection of COVID, an inflammatory and immunologic response is created, itself theoretically could produce intraluminal thrombosis with subsequent edema and necrosis.
In cases of initial stages (Ficat I or II), the risk of collapse should be measured with Kerboul angle, < 190º the possibility it is almost 0% in 5 years, but in angles between >190º-<240º chance can rise up to 50% at 5 years; treatment could be observation, antiresorptive drugs, core decompression with grafting, in our case, we do not observe acute changes on MRI, therefore we preferred observation. When subchondral fracture is presented the progression to osteoarthritis is inenvitable, THR is the ideal treatment and should be perform according to symptoms.
Declarations
Acknowledgments: All authors participate in equal quantitively for these care report. There were no sources of funding.
Conflict of interest: None declared.
Ethical approval: No ethical approval was needed for this case report.
Consent: The authors obtained written informed consent from the patient for this publication.
References
- L Gattinoni, P Taccone, E Carlesso, et al. Prone position in acute respiratory distress syndrome. Rationale, indications, and limits, Am. J. Respir. Crit. CareMed. 2013; 188: 1286-1293.
- World Health Organisation, Clinical Management of Severe Acute Respiratory Infection (SARI) when COVID-19 Disease is Suspected-Interim Guidance, WHO. 2020.
- Guérin J, Reignier JC, Richard, PROSEVA Study Group, et al. Prone positioning in severe acute respiratory distress syndrome, N. Engl. J. Med. 2013; 368: 2159-2168.
- Alhazzani W, Møller MH, Arabi YM, et al. Surviving sepsis campaign: Guidelines on the management of critically ill adults with coronavirus disease 2019 (COVID-19). Intensive Care Med. 2020; 46: 854e87.
- Zalavras CG, Lieberman JR. Osteonecrosis of the femoral head: Evaluation and treatment. J Am Acad Orthop Surg. 2014; 22: 455-464.
