
Open Access, Volume 9
Priapism managed with anti-platelets after failed shunting
Sunayana Chatterjee*; Hrishikesh Deshmukh; Sagar Bassi; Shamz Iqbal
Department of Surgery, Bharati Vidyapeeth Deemed University Medical College, Pune, India.
Sunayana Chatterjee
Department of Surgery, Bharati Vidyapeeth Deemed University medical college, Pune, India.
Email: sunayana.october13@gmail.com
Received : June 03, 2023,
Accepted : July 25, 2023
Published : July 31, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Priapism is a non-sexual, persistent erection characterized by little or no cavernous blood flow and abnormal cavernous blood gases [1]. Ischemic priapism is a urologic emergency with an estimated incidence of 5.3 per 100,000 men per year in the USA [2]. More than 95% of priapism cases are ischaemic [3]. We reviewed a case of recurrent ischemic priapism with multiple failed attempts of shunt surgery and finally treating with anti-platelets which was successful.
Keywords: Ischemic priapism; Shunt surgery; Refractory; Anti-platelets.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Chatterjee S (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Chatterjee S, Deshmukh H, Bassi S, Iqbal S. Priapism managed with anti-platelets after failed shunting. Open J Clin Med Case Rep. 2023; 2080.
Introduction
Priapism is defined as a prolonged penile erection lasting more than 4 h, remaining despite orgasm and in the absence of sexual stimulation. There are three types of priapism: Ischaemic, non ischaemic and stuttering. The most common of these is Ischaemic Priapism (IP). It represents a compartment syndrome of the corpus cavernosa with minimal or no arterial flow into the penis. It causes time-dependent damage to the smooth muscle, which results in significant longterm morbidities- permanent Erectile Dysfunction (ED), penile shortening, penile curvature and loss of girth [4]. The first step in the management of priapism is to aspirate the blood of the corpus cavernosa with a large bore 16–18G butterfly needle. A sample of the aspirate should be sent for arterial blood gas analysis. A hypoxic, hypercapnic and acidotic blood gas sample confirms the diagnosis of IP [4]. Following aspiration, the corpus cavernosa should be irrigated with 0.9% normal saline. This may lead to successful detumescence in approximately 30% cases. If this fails, injection a sympathomimetic agent into the corpus cavernosa with simultaneous cardiac monitoring should be done [4]. Shunt procedures are undertaken in patients with IP that are refractory to these initial management steps [4].
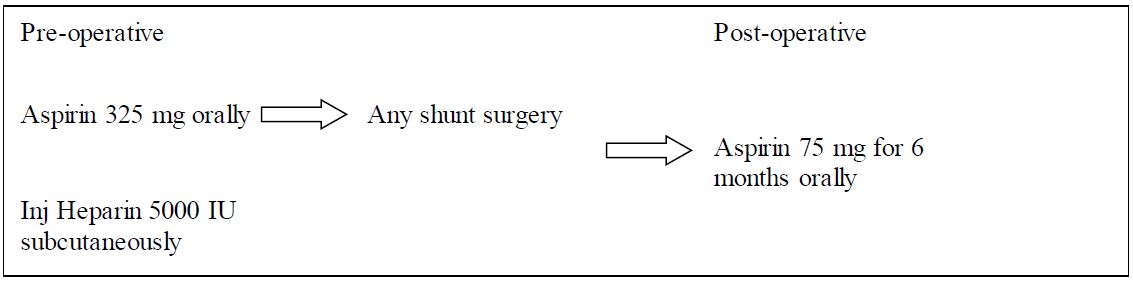
Our index case is a 23 year old male, who presented to casualty with complains of sustained pain ful erection for last 34 hours. He had history of similar complaints twice in past (1 month back), which resolved spontaneously after 6-8 hours. There was no history of trauma to the pelvis/ perineum or penis. Patient was immediately taken up for aspiration of pooled blood and irrigation with epinephrine. But patient developed recurrent priapism. Winter shunt, T- shunt and Al Ghorab shunt was also attempted but, patient continued to develop recurrent priapism. Sub cutaneous heparin 5000 IU stat dose was given and the patient was started on anti-platelets, the patient achieved penile faccidity. Patient was discharged on anti-platelets for 6 month. On 6 month follow up, patient was doing well and had no episode of recurrent priapism and had normal erections.

Figure 1: (A): Irrigation of corpora cavernosa, (B): aspiration of clots and old blood; (C): Al Ghorab shunt
Discussion
In acute ischemic priapism that fail to respond to alpha-adrenergic agonists, various shunting procedures have been developed to re-establish circulation of the corpora cavernosa and prevent necrosis of erectile tissues. However, early closure of the newly created shunt, resulting in recurrent priapism, is a common complication which leads to repeated shunting procedures [5]. In subsequent re-shunting, blood clots at the site of shunting and the un-coagulated “crank-case oil”-like old blood are removed. The old blood inside the corpora cavernosa does not clot due to the abundance of endothelium-derived anticoagulating and fibrinolytic factors within the corpora cavernosa. But, the newly created shunt is not lined and protected by endothelium. In fact, the shunts created, cuts a new wound through the collagen-rich tunica albuginea. Hence, the collagen-activated platelets and fibrin begin to form a clot within minutes to seal off the shunt [5]. So, keeping the newly created shunt patent requires a continuous high blood flow through a large caliber shunt. This helps the shunt to remain open for hours to days until the smooth muscles of the corpora cavernosa and helicine arteries regain normal contractile capacity. Premature closure of the shunt is due to inadequate size and stagnant blood flow, which enhances the adherence of platelets and fibrin to collagen, and eventually forms a thrombus at the site of shunting and causes early recurrence of priapism. Hence, early postoperative shunt closure is a postoperative thrombotic complication, and its management should be incorporated into the future guidelines for treatment of ischemic priapism [5].
References
- Bivalacqua TJ, Allen BK, Brock G, Broderick GA, Kohler TS, et al. Acute ischemic priapism: an AUA/SMSNA guideline. The Journal of urology. 2021; 206: 1114-21.
- Butaney M, Thirumavalavan N, Rodriguez D, Gross MS, Munarriz R. Current practice in the management of ischemic priapism: an anonymous survey of ISSM members. International journal of impotence research. 2019; 31: 404-9.
- Baumgarten AS, VanDyke ME, Yi YA, Keith CG, Fuchs JS, et al. Favourable multi‐institutional experience with penoscrotal decompression for prolonged ischaemic priapism. BJU international. 2020; 126: 441-6.
- Johnson MJ, Kristinsson S, Ralph O, Chiriaco G, Ralph D. The surgical management of ischaemic priapism. International Journal of Impotence Research. 2020; 32: 81-8.
- Lue TF, Garcia M. Should perioperative anticoagulation be an integral part of the priapism shunting procedure?. Translational Andrology and Urology. 2013; 2: 316.
