
Open Access, Volume 9
Lumbar spine osteoid osteoma in a six-year-old male patient: A Case Report
Carlo Ciccullo1; Monia Martiniani2; Rosa Palmisani1; Edoardo Angeletti1; Leonard Meco2; Silvia Amico1*; Nicola Specchia1; Antonio P Gigante1
1Clinical Orthopaedics, Department of Clinical and Molecular Science DISCLIMO, Università Politecnica delle Marche, Ancona, Italy.
2Clinic of Adult and Paediatric Orthopaedics, Azienda Ospedaliero-Universitaria, Ospedali Riuniti di Ancona, Ancona, Italy.
Silvia Amico
Department of Clinical and Molecular Sciences, Università Politecnica delle Marche, Via Tronto 10/a, 60020 Torrette di Ancona, Italy.
Email: s.amico@pm.univpm.it
Received : May 30, 2023,
Accepted : July 18, 2023
Published : July 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Osteoid Osteomas (OO) are rare primary tumors that usually don’t arise the spine. Osteoid osteoma is a benign tumor that often occurs between the ages of 10 and 35 years. Histologically, the tumor consists of a central nest composed of bony trabeculae separated from each other by fibrous vascular connective tissue, surrounded by an area of sclerotic bone. We present a case of spinal osteoid osteoma (L2) of a 6-year-old boy. Lower back pain that worsened during the night hours resulting in lack of rest was the main symptom. The patient also reported difficulty and pain during squatting and a scoliotic posture. Osteoid osteoma can be detected with Magnetic Resonance Imaging (MRI) and Computed Tomography (CT), which are often used to identify the location of the nest, especially in the presence of an intra-articular lesion. CT is excellent for characterizing the lesion, while MRI is certainly sensitive but less specific. This technique is often unable to identify the nidus. Once the diagnosis was established by physical examination and imaging, laminectomy and curettages were performed. Twelve months after the surgical intervention, the patient showed complete remission of the symptoms and no disabilities. The scoliotic posture after surgery also decreased until it disappeared.
Keywords: Osteoid osteoma; Lumbar pain; Gross total resection; Posterior laminectomy; Lumbar arthrodesis.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Amico S (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Ciccullo C, Martiniani M, Palmisani R, Meco L, Amico S, et al. Lumbar spine osteoid osteoma in a six-year-old male patient: A case report. Open J Clin Med Case Rep. 2023; 2074.
Introduction
Osteoid osteoma is a rare primary tumor that usually doesn’t arise the spine. The OO is usually a benign bone tumor that typically occur in children, adolescent and young adults between the ages of 10 to 35 years with a male-to-female ratio of 3:1 [1]. It is commonly located in the long bone on the subcortical shaft and metaphysis. Femur and tibia are affected in 65-80% of cases. Other common localizations are the phalanges (20%). There are two classification schemes for osteoid osteoma, both of which describe the location of the tumor in bone. With the first scheme, tumors are classified as cortical, medullary (cancellous), or subperiosteal on the basis of radiographic findings. This method is more traditional and more frequently used than the other classification scheme [2]. Histologically, this tumor, contains osteoblasts that produces osteoid and woven bone. It is characterized by a central nidus composed of bony trabeculae surrounded by a zone of sclerotic bone. The nidus and surrounding bone are sharply demarcated from each other. The osteoid trabeculae are separated by vascular fibrous connective tissue. Macroscopically OO, usually appears like a discrete oval or round mass of reddish- brown tissue within the cortex of the involved bone. The consistency varies from soft granular to dense sclerotic [3,4]. Most lesions are around 1 cm in size and rarely exceed 2 cm even when the symptoms have been present for several years. Herein, we report a case of Osteoid Osteoma of the lumbar spine that occurred in a male six-years-old patient. In addition, we review the cases report in Italian and European literature so far.
Case Presentation
A six-years-old male child presented with an history of pain in the lumbar spine. The pain was insidious in onset, progressive and aggravated at night affecting sleep and caused difficulty in playing and squatting. There was no history of trauma, fever, pain or swelling of any joints, chest pain, weight loss or loss of appetite, and urinary/gastrointestinal or respiratory tract infections. There was family history suggestive of scoliosis.
He came to us further consultation with persistent pain and antalgic gait. On clinical examination, the child was cooperative and active, with normal height and weight for his age. Neurological and musculoskeletal examination revealed intact cranial nerves with intact bilateral lower limb sensation. There was no muscle retraction. The examination of the spine revealed the presence of a scoliotic curve with a right lumbar hump. No apparent current vascular and nervous deficits in his upper and lower limbs were detected. F5 muscle strength was evaluated using MRC (Medical Research Council) Scale. Tendon reflexes were symmetrically elicited.
Review of X-Ray of the spine showed a convex right large radius curve (Figure 1). As suspicion was made on bone tumor, MRI scan of the spine was done which revealed a focal alteration of L2 with partial involvement of the left hemi portion of the soma of the entire vertebral peduncle with high signal in the long aTR frequencies. Furthermore, focal alterations of the muscle tissues adjacent to the L2 soma and to the peduncle were also reported (Figure 2).
Hence, a provisional diagnosis of osteoid osteoma was made, and CT scan of the pelvis was further done which showed a 0.98 x 1.08 x 0.46 cm well margined lytic lesion in the left hemisome of L2 suggestive of osteoid osteoma.
Among available treatment modalities, we choose the surgical treatment. The parents were given detailed explanations about the procedure. Informed written consent were signed. After a thorough preanesthetic evaluation and adequate fasting period, general anesthesia was induced on the patient with oxygen and Propofol and Laryngeal Mask Airway was inserted for airway management. Anesthesia was maintained with oxygen and inhalation anesthesia with adequate dose of Fentanyl and analgesic. The patient was positioned prone and skin preparation and draping were done as standard protocol. A L2-L3 epispinous incision of approximately 5 cm was made. Dieresis of the subcutis, adequate hemostasis to avoid excessive bleeding and subsequent fasciotomy was practiced. A subperiosteal exposure of the L2-L3 level on the left was performed. The lesion was localized with the help of fluoroscopic assistance to confirm accurate position. A left hemilaminectomy was performed. A high-speed burr was used to break through the cortex overlying the nidus, it was removed using the curettes and the tumor bed was cleaned with a high-speed burr (Figure 3). After the procedure an accurate anatomical plane suture and a sterile dressing was performed. Total duration of procedure was about 2 hours. Recovery of the child from anesthesia was uneventful. The next day the pain score was assessed to be “zero on ten” at rest and “three on ten” while sitting up and in an orthostatic position.
The procedure was performed with joint effort from the Departments of Clinica Ortopedica dell’Adulto e Pediatrica, Clinica di Anestesia and Clinica di Radiologia of the Marche Polytechnic University and it was performed at Salesi Pediatric Hospital of Ancona.
Vital signs and analyzes were checked daily during the hospital stay. The patient was discharged 3 days after the surgery with advice of follow-up.
On follow up examination after 7 days there was the disappearance of nocturnal pain and he reported no difficulty in walking autonomously. In 14 days follow up the stitches have been removed. The scar has always remained clean and tidy, without ever appearing of inflammation or infection.
In the third follow up months, the patient referred he started playing football again in a competitive manner without any problems. An improvement was also observed regarding scoliosis for which he came to our observation.
In fact, we observed that before the surgery the Cobb angle was 12.8° Cobb and 12 months after, it was 7.8° Cobb.
In the 12th follow up months, his CT findings were unremarkable and no obvious residual lesion was marked.
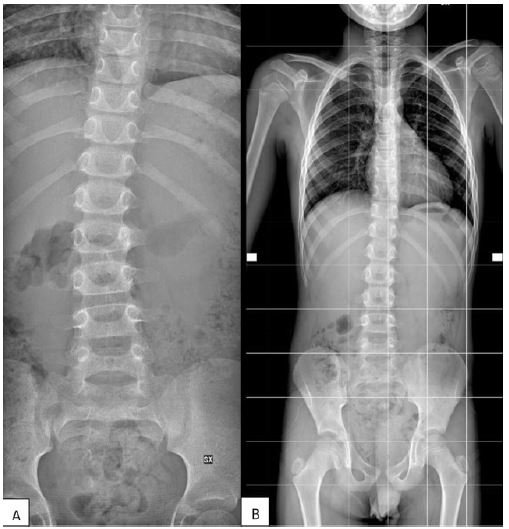
Figure 1: (A) Preoperative X-ray showing right convex scoliosis. (B) 1-year FU X-ray showing reduction of the scoliosis.
Figure 2: Preoperative MRI showing osteoid osteoma at the level of the second lumbar vertebrae.

Figure 3: (A,B) Intraoperative X-ray with landmark before OO excision. (C) Intraoperative X-ray with landmark after OO excision. (D) Intraoperative picture showing K-wires used as landmark.
Discussion
Jaffe HL was the first to describe osteoid osteoma as a specific entity in 1935. By analyzing the reported cases, we infer that a majority of osteoid osteomas of the spine occurred in the second decades of life [5].
The first step for a correct diagnosis is a traditional radiography. This particular exam may be normal or may show a solid periosteal reaction with cortical thickening. The nidus is sometimes visible as a well- circumscribed lucent region, occasionally with a central sclerotic dot. If there is extensive sclerosis or nidus < 4 mm, nidus may not be seen in plain radiographs.
Osteoid Osteoma can be detected on MRI and CT scan, which are often used to identify the location of the nidus especially when there is an intra- articular lesion.
CT scan is excellent to characterize the lesion. It shows all the principal tumor characteristics (lucent nidus within surrounding sclerotic reactive bone and central sclerotic dot).
The MRI is certainly sensitive, but it is less specific. This technique is often unable to identify the nidus. The hyperemia and resultant bone marrow edema pattern may result in the scans being misinter preted as representing aggressive pathology [6].
Other radiographical test to detect OO are scintigraphy and ultrasound.
Biopsy prior to treatment is not mandatory due to a remarkable amount of false negative findings in clinically and morphologically unambiguous cases of osteoid osteoma. With delayed diagnosis, features other than pain such as limping or muscle wasting and weakness can appear, which was prominent in this particular case.
From a clinical point of view, this lesion is biphasic. In the first time it is characterized by local pain that is typically more frequent and severe at night. This pain is usually relieved by aspirin within 30 minutes (75% of cases) and it is increased by alcohol consumption. Another characteristic early sign is local swelling and point tenderness. There are also other symptoms that could occur later: Bony deformity, Gait disturbances, muscle atrophy, Leg length discrepancy (long leg on the involved side), Scoliosis (concavity same side as lesion), growth disturbances, Osteoarthritis.
Regarding the scoliosis and its connection with OO. Lots of studies demonstrates the strict connection between these two pathologies. It has been observed that several times the concavity can be found in the same side as lesion. This could be due to the fact that the predilection site of spinal osteoid osteoma is the posterior column, which could lead to secondary scoliosis.As patients with spine OO come to visit with scoliosis as the primary symptom, the tumor could be easly misdiagnosed or even never diagnosed [7-9].
Osteoid Osteoma can be distinguished from other bone forming tumors based on the difference in size, localization, pathology, and clinical symptoms. For example, the chondroblastoma in epiphyseal locations of children with osteolytic lesions and extensive bone marrow edema and periosteal reaction can resemble osteoid osteoma.
The general indication of treatment of osteoid osteoma is persistent pain. The treatments can be different according to the needs of the patient and the operator. Non operative treatment can be considered as an option since the natural history of osteoid osteoma is that of spontaneous healing. Some authors reported resolution of symptoms with conservative management in osteoid osteoma within 6 to 15 years. Using of aspirin or other NSAIDs decreases this time to 2 to 3 years. In anatomical areas where OO is not easly accessible this may be a viable treatment [10,11].
Conventional open excision was achieved by localizing the nidus with a fluoroscope and subsequent en bloc excision or curettage. Mini-incision surgery consisted of the following procedures: first, a smooth K-wire, 1.6 mm in diameter was inserted into the nidus under CT guidance and a 2-3 cm longitudinal incision was made centered at the K-wire. The wound was then deepened to the bone along the K-wire with special attention paid to prevent neurovascular injuries. The guide wire was then removed and a drillbid or a high-speed burr was used to break through the cortex overlying the nidus. The nidus was removed with curettes, and the tumor bed was cleaned with a high-speed burr [12-14].
Other methods which are less invasive include Percutaneous Bone Resection And Drilling (PBRD) and CT-guided Radiofrequency Ablation of tumor (RFA).
Radiofrequency ablation for treating osteoid osteoma was first described in 1989. It is considered by some authors the gold standard treatment for osteoid osteoma in all locations as it is an effective, safe method with lowest recovery time and rate of complications. It allows the precise delivery of heat under image guidance to the targeted tissue. It can be done in a day care basis [15].
CT-guided RFA has become the preferred method owing to a low morbidity rate, minimal postoperative complications, minimal tissue exposure, rapid recovery, and no restriction of weightbearing activity.
In addition, the healing rate is 76% to 100%, with a major complication rate of 0% to 5%. However, using CT-guided RFA, there are different reports of articular cartilage damage in weightbearing joints.
Direct observation and femoral head distraction during the arthroscopy may decrease the risk of cartilaginous thermal damage.
The open approach for L2 lamina and soma was preferred to visualize the full extension of the tumor.
Gonzalez et al and Mallepally et al. recommend en bloc resection in osteoid osteoma [14,16,17].
Authors have used standard posterior midline approach so the lesion could be easily visualized and approached by a good skeletrization. After en bloc excision of the lesion, the defect was reinforced with graft. Surgical reinforcement can be achieved with allogenic cortical strut graft, non-vascularized autologous fibular strut, or CHA. Ideal graft material should be osteoinductive, osteoconductive, osteogenic, and easily available. Autologous non-vascularized cortical grafts provide good support at their recipient site.
Normally, once the lesion is excised, they do not recur. Although malignant transformation is very rare, one case has been reported in literature, which transformed into an aggressive osteoblastoma.
Conclusions
The occurrence of Osteoid Osteoma in the spine of a 6-years-old male patient is rare. Herein, we reported this case. Clinical, radiographic, and pathological features were considered to arrive at the correct diagnosis. The small number of cases reported in this regard necessitates an increased awareness among the pediatric orthopedists worldwide to report additional cases in literature.
It will provide a means for better understanding and show a clear picture of such rare bony lesions so that they could be diagnosed at a much earlier stage.
Declarations
Conflicts of interest: The authors certify that they have NO affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.
Funding: The authors report no involvement in the research by the sponsor that could have influenced the outcome of this work.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors’ contributions: All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Carlo Ciccullo, Monia Martiniani, Rosa Palmisani, Edoardo Angeletti. Leonard Meco and Silvia Amico. The first draft of the manuscript was written by Carlo Ciccullo, Monia Martiniani and Rosa Palmisani. All authors commented on previous versions of the manuscript. All authors read and approved the final version of the manuscript.
All authors contributed equally to the manuscript and read and approved the final version of the manuscript.
Acknowledgements: None.
References
- Jee Won Chai, Sung Hwan Hong, Ja-Young Choi, Young Hwan Koh, Joon Woo Lee, et al. Radiologic Diagnosis of Osteoid Osteoma: From Simple to Challenging Findings. RadioGraphics. 2010; 30: 737-749.
- Kayser F, Resnick D, Haghighi P, Pereira Edo R, Greenway G, et al. Evidence of the subperiosteal origin of osteoid osteomas in tu-bular bones: analysis by CT and MR imaging. AJR Am J Roentgenol. 1998; 170: 609-614.
- Kan P, Schmidt M. Osteoid osteoma and osteoblastoma of the spine. Neurosurgery clinics of North America. 2008; 19: 65-70.
- Noordin S, Allana S, Hilal K, Nadeem N, Lakdawala R, et al. Osteoid osteoma: Contemporary management. Orthopedic reviews. 2018; 10: 108-119.
- Jaffe HL. Benign osteoblastoma. Bull Hosp Jt Dis. 1956; 17: 141-151.
- De Ga K, Bateni C, Darrow M, McGahan J, Randall LR, et al. Polyostotic osteoid osteoma: A case report. Radiology Case Reports. 2020; 15: 411-415.
- Jain M, Doki S, Gantaguru A, Mohakud S, Jha S. Osteoid Osteoma of the Body of the Vertebrae Causing Painful Scoliosis. Asian J Neurosurg. 2020; 15: 1037-1040.
- Chen YL, Jiang WY, Ma WH. Osteoid osteoma: Lower back pain combined with scoliosis. J Int Med Res. 2020; 48: 1-6.
- Sapkas G, Efstathopoulos NE, Papadakis M. Undiagnosed osteoid osteoma of the spine presenting as painful scoliosis from adolescence to adulthood: A case report. Scoliosis. 2009; 4: 9.
- Burn S, Ansorge O, Zeller R, Drake J. Management of osteoblastoma and osteoid osteoma of the spine in childhood: Clinical article. Journal of Neurosurgery: Pediatrics. 2009; 4: 434-438.
- Freiberger RH. Osteoid Osteoma of the Spine. A Cause of Backache and Scoliosis in Children and Young Adults. Radiology. 75; 2.
- Campanacci M, Ruggieri P, Gasbarrini A, Ferraro A, Campanacci L. Osteoid osteoma. Direct visual identification and intralesional excision of the nidus with minimal removal of bone. J Bone Joint Surg Br. 1999; 81: 814-820.
- Saccomanni B. Osteoid osteoma and osteoblastoma of the spine: A review of the literature. Curr Rev Musculoskelet Med. 2009; 2: 65-67.
- Mallepally AR, Mahajan R, Pacha S, Rustagi T, Marathe N, et al. Spinal osteoid osteoma: Surgical resection and review of literature. Surg Neurol Int. 2020; 11: 308.
- Kumar Duwal Shrestha S, Jung Rayamajhi A, Rawal P, Thapa R, Karki U, et al. Radiofrequency Ablation of Osteoid Osteoma of Neck of Femur: A Case Report. J Nepal Med Assoc. 2021; 59: 513-517.
- Gonzalez G, Abril JC, Mediero IG, Epeldegui T. Osteoid osteoma with a multicentric nidus.. International Orthopaedics (SICOT). 1996; 20: 61-63.
- Adam G, Neuerburg J, Vorwerk D, Forst J, Gunther RW. Percutaneous treatment of osteoid osteomas: combination of drill biopsy and subsequent ethanol injection. Semin Musculoskelet Radiol. 1997; 1: 281-284.
