
Open Access, Volume 9
Surgical treatment of giant diving goiter: A case report
Duarte AJV; Fernandes LD; Virla AF; Magalhaes PNLM; Oliveira GS; Lima LV; Ferry F; Ascencao MAS; Morard MRS; Fiorelli RKA*
Department of Surgery, Gaffrée and Guinle University Hospital, Federal University of the State of Rio de Janeiro (UNIRIO), Rio de Janeiro, Brazil.
Rossano K A Fiorelli
Department of Surgery, Gaffrée and Guinle University Hospital, Federal University of the State of Rio de Janeiro (UNIRIO), Rio de Janeiro, Brazil.
Email: fiorellirossano@hotmail.com
Received : May 26, 2023,
Accepted : July 13, 2023
Published : July 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
It is estimated that goiters occur in about 5% of the world’s population and that they constitute about 7% of mediastinal tumors [1]. We present a case in which a diving goiter was much larger in size than those normally published in the literature worldwide.
Keywords: Diving goiter; Thyroid goiter; Mediastinal mass.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Fiorelli RKA (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Duarte AJV, Fernandes LD, Virla AF, Magalhaes PNLM, Oliveira GS, Lima LV, Fiorelli RKA, et al. Surgical treatment of giant diving goiter: A case report. Open J Clin Med Case Rep. 2023; 2072.
Introduction
Diseases of the thyroid gland are common problems and are increasingly diagnosed by the availability and ease of access to tests such as cervical ultrasound and computed tomography of the chest and neck, which leads patients, symptomatic or not, to seek clarification of the images obtained. The main indications for surgical treatment of thyroid changes include clarification of suspicious lesions, treatment of diagnosed neoplasms and goiters, compressive or leading to aesthetic changes [1,2].
We present a case of giant diving goiter with exuberant respiratory symptomatology that exceeded commonly published limits.
Case Presentation
A 68-year-old female patient, smoker since the age of eight, diagnosed with giant diving goiter, irregularly monitored by several endocrinologists in recent years, presenting progressive dyspnea mainly in the supine position. Computed tomography performed on the 10th of may of 2022 revealed a heterogeneous mass with hypodense areas and foci of calcification, measuring 20.6 x 7.5 x 10.7 cm, located in the anterior mediastinum, determining significant compression of the trachea, esophagus and lung parenchyma in correspondence, associated with collateral circulation in the anterior mediastinum and anterior chest wall (Figure 1). Due to the exuberance of the respiratory symptoms that compromised the quality of life, the patient was submitted to complete resection of the diving goiter through cervicotomy associated with sternotomy. Involvement of the innominate trunk was observed, requiring its respective ligation (Figure 2 and 3). The specimen sent for anatomopathological study measured 24 x 13 x 06 cm (Figure 4), weighed 772 g and revealed nodular follicular thyroid disease, with extensive areas of hyalinization.

Figure 1:

Figure 2:
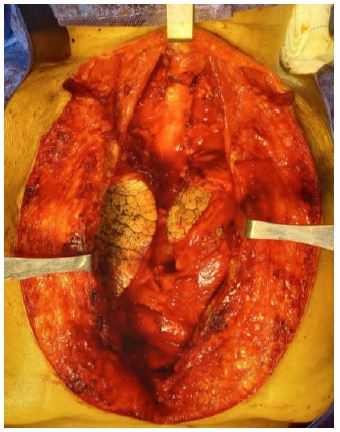
Figure 3:

Figure 4:
The patient remained in the postoperative ICU, intubated due to her precarious respiratory condition for 48 hours, requiring tracheostomy after extubation for bilateral paralysis of the vocal cords. In the ICU due to pneumonia and large amount of secretion, she presented infection of the surgical wound with sternal dehiscence that was treated with antibiotic and intensive care of the operative wound. On the 10th postoperative day and, with improvement of the infectious condition, she was taken to the operating room for reapproach of the surgical wound with debridement and sternorhaphy. She was discharged to the ward on the 14th postoperative day in good general condition, remaining until the 21st postoperative day, when she underwent videolaryngoscopy that revealed functioning vocal cords being decannulated without intercurrences. She was discharged from the hospital in good general and local conditions, and she was intructed to follow-up with endocrinology and thoracic surgery physicians.
Discussion
Goiter is a term that means thyroid enlargement and can be defined in several ways, among them, as a gland twice as large as the normal size of the gland or a thyroid weighing more than 40 g [3]. It is estimated that goiters occur in about 5% of the world's population and that they constitute about 7% of mediastinal tumors [2]. There are several concepts in the literature for diving goiter, such as: retrosternal, intrathoracic, substernal, mediastinal, endothoracic or intrathoracic goiter, considering that it extends beyond the thoracic introitus or that they penetrate 50% of the gland into the thoracic cavity or even that it presents insinuation to the mediastinum [4,3,5]. The diving goiter mainly affects women over 60 years of age. The clinical picture usually presents a slow evolution, of an insidious character, as the patient remains asymptomatic for a long period; when symptomatic there may be dyspnea, dysphagia, dysphonia, hyperthyroidism, superior vena cava syndrome, among others. Even in asymptomatic cases, the surgical approach is generally accepted as a therapeutic option due to the potential airway compromise, possibility of malignancy and the ineffectiveness of nonoperative treatment, with cervical incision associated with sternotomy being a safe resection modality, especially in goiters closely related to noble mediastinal structures [1,4].
In the operations of diving goiters, the concern with possible nerve injuries should be great because of the eventual need to make a digital displacement of the endothoracic component of the goiter or the need to do a sternotomy to achieve its resection. Removal of substernal goiter has higher rates of unintentional permanent injury of the recurrent laryngeal nerve when compared to cervical goiter [6-8]. Given the propensity to cause symptoms, especially airway compressives, and the possibility of malignancy, surgical treatment should be considered in most cases. The preferred access route is cervicotomy, which may be accompanied by sternotomy; in some cases, and the experience of the surgical team is of fundamental importance to avoid injuries during surgery, especially nervous injury (Table 01) [1,6,3,9-13].
Table 1: Access routes.
Author: casuistry, sternotomy, cancer, paralysis.
| Author | Casuistry | Sternotomy | Cancer | Paralysis |
|---|---|---|---|---|
| Vadaz et al. | 175 | 17,7% | 5,7% | 8% |
| Vlasak et al. | 87 | 4,6% | 4,6% | 5,7% |
| Torre et al. | 237 | 3,4% | 6,8% | 4,6% |
| Cougard et al. | 225 | 8% | 3,7% | 1,3% |
| Zhang et al. | 87 | 30% | 11,5% | 20,7% |
| Fiorelli et al. | 239 | 5% | 27,6% | 5,44% |
Conclusion
Computed tomography is essential for the diagnosis of goiters with penetration into the posterior mediastinum or with prolongation below the aortic arch aiming at programming associated thoracotomy.
Post-thyroidectomy vocal complaints are frequent, even in patients without videolaryngoscopic alterations of laryngeal mobility.
Giant goiters will necessarily require associated sternotopmy due to the impossibility of extraction by a neck incision.
References
- Aspinall S. Effect of surgeons’ annual operative volume on the risk of permanent Hypoparathyroidism, recurrent laryngeal nerve palsy and Haematoma following thyroidectomy: Analysis of United Kingdom Registry of Endocrine and Thyroid Surgery (UKRETS). Langenbeck’s Archives of Surgery. 2019; 404: 421-430.
- Newman E, Shaha AR. Subesternal goiter. J Surg Oncol. 1995; 60: 207-212.
- Neves MCD, Rosano M, Hojaij FC, Abrahão M. et al. Avaliação crítica de 33 pacientes com bócio mergulhante cirurgicamente por cervicotomia. Revista Brasileira de Otorrinolaringologia, 75, n. 2, pág. 172-176, 2009.
- Cougard P, Vanet S, Matet P, Goudet P, Viard H. Endothoracic goiter operated on by cervicosternotomy. Apropos of 18 cases. Chirurgie. 1994; 120: 309-313.
- Torre G, Borgonovo G, Amato A, Arezzo A, Ansaldo G, et al. Surgical management of substernal goiter: analysis of 237 patients. Am Surg. 1995; 61: 826-831.
- Fiorelli RKA, Duarte AJV, Quadros TA, Montenegro TS, Portari Filho PE, et al. Anatomical and developmental aspects of iatrogenic injury to the right recurrent laryngeal nerve in surgical resections of substernal goiter. Anatomical Record-Advances in Integrative Anatomy and Evolutionary Biology. 2021; 304: 1242-1254.
- White ML, Doherty GM, Gauger PG. Evidence-based surgical management of substernal goiter. World Journal mundial of surgery. 2008; 32: 1285-1300.
- Zhang B, Tu G. Surgery of substernal thyroid goiter. Zhonghua Er Bi Yan Hou Ke Za Zhi. 1997; 32: 115-118.
- Pieracci FM, Fahey III TJ. Effect of hosital volume of thiroidectomies on outcomes following substernal thyroidectomy. Would Journal of Surgery. 2008; 32: 740-746.
- Simas CJA, Duarte AJV, Portari Filho PE, Fiorelli RKA, Silva DSE, et al. Laryngoscopic and Electromyographic Findings after Thyroidectomy. Scholarly Journal of Otolaryngology. 2023; 9: 1067-1072.
- Sosa JA et al. The importance or sugeon experience for clinical and economic outcomes from thiroidectomy. Annals of Surgery. 1998; 228: 320-330.
- Vadaz P, Kotsis L. Surgical aspects of 175 mediastinal goiters. Eur J Cardiothorac Surg. 1998; 14: 393-397.
- Vlasak V, Vach B, Valka J. Personal experience with surgery of retrosternal goiter. Cas Lek Cesk. 1995; 134: 583-586.
