
Open Access, Volume 9
“Fix after Flap” concept that covers exposed bone wounds on the day for suffering Gustilo-Anderson IIIB and C fractures
Masaki Fujioka1,2*; Kiyoko Fukui1; Marie Idemitsu1
11Department of Plastic and Reconstructive Surgery, National Hospital Organization Nagasaki Medical Center, Nagasaki, Japan.
22Department of Clinical Research Center, National Hospital Organization Nagasaki Medical Center, Nagasaki, Japan.
Masaki Fujioka
Department of Plastic and Reconstructive Surgery, National Hospital Organization Nagasaki Medical Center, 1001-1 Kubara 2 Ohmura City 856-8562, Japan.
Tel: +81-0957-52-3121, Fax: +81-0957-54-0292;
Email: inazumahayato7@gmail.com
Received : June 01, 2023,
Accepted : July 07, 2023
Published : July 10, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: “Fix and Flap” method is now the golden standard for the treatment of Gustilo-Anderson (GA) IIIB and C fractures. Although they require early soft tissue reconstruction, this not always possible. This paper introduces a new concept of “Fix after Flap” that aims to close the wound with a flap on the day of injury.
Case study: A retrospective descriptive study including 21 patients with CAIIB and C fractures who were treated and salvaged their feet in our Medical Center from 2012 to 2021 was carried out. First, we examined the relationship between the presence or absence of postoperative infection and period until the start of load-walking after injury for GAIIIB open fractures in 16 of these cases. Next, we examined the relationship between the period until the wound resurfacing after injury and frequency of postoperative infections for 21 patients with GAIIIB and C fractures. The Mann-Whitney U test was used to determine statistical differences.
Results: It was clarified that when postoperative osteomyelitis developed, it clearly took a significantly longer time to start weight-bearing walking (P< 0.05), and the earlier the wound closure, the lower the incidence of osteomyelitis (P< 0.05). In particular, in 7 cases in which the exposed bone wound was resurfaced on the day of injury, there was no complication of infection in any of the cases. Conclusion: We believe that "Fix after flap" that closes the wound on the day of injury, is expected to reduce the rate of postoperative infection.
Keywords: Open fracture; Gustilo-Anderson Type-III Fracture; osteomyelitis; Fix and Flap; wound closure.
Abbreviations: GA III: Gustilo-Anderson III.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Fujioka M (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Fujioka M, Fukui K, Idemitsu M. “Fix after Flap” concept that covers exposed bone wounds on the day for suffering Gustilo-Anderson IIIB and C fractures. Open J Clin Med Case Rep. 2023; 2068.
Introduction
Gustilo-Anderson (GA) III fracture is defined as open fracture with extensive soft-tissue laceration, damage, or defect. In a retrospective study of GAIII open fractures from 1961 to 1968, the infection rate was 44%, forcing many limbs to be amputated [1]. For the upper limbs, relief arm was achieved in 45 (94%) of 48 patients with GAIII in a report from 1994 to 2014 [2]. Similarly, a recent report about lower limb fractures showed that 93 cases of GAIII fractures between 1994 and 2012 necessitated amputation in 10 patients (12%). The factors leading to these amputations were infectious complications in 60% and vascular occlusion in 40% [3]. With the development of damage control surgery, surgical methods, and antibiotics, the limb salvage rate for GAIII fractures has improved. Nowadays, it is necessary to shift the purpose of treatment for severe limb trauma from limb preservation to early rehabilitation. Especially, GAIIIB and C fractures, which are defined as open fracture with extensive soft-tissue defect, requiring the resurfacing of complex bone-exposing wounds have a high complication rate of infection [1]. “Fix and flap” is considered an ideal management for the treatment of GAIIIB and C bone-exposing injuries, involving radical debridement of the wound, skeletal stabilization, and early soft-tissue coverage with a vascularized muscle flap [4,5].
In this paper, we examine the effect of the presence or absence of postoperative infection on the time to start rehabilitation, and relationship between the period until the wound resurfacing after injury and the frequency of postoperative infections in patients with severe open fractures of the lower extremities. Based on the results, I introduce the “Fix after flap” method, which is a new concept in GAIIIB and C fracture treatment strategies.
Case Study
A retrospective descriptive study including 22 patients with CAIIB (18 patients) and C (4 Patients) fractures who were treated in our Medical Center from 2012 to 2021 was carried out. All patients underwent debridement, open reduction, and external fixation on the day of injury. Twenty-one were salvaged, but one patient underwent leg amputation due to the development of myonephropathic metabolic syndrome. The final rate of leg salvage was 95.5%, and they were all discharged walking on their feet. For all patients, penicillin or cephalosporin and anaerobic coverage (clindamycin) were used together at first, which was modified after Gram stains and culture reports became available.
First, we examined the relationship between the presence or absence of postoperative infection and period until the start of load-walking after injury for GAIIIB open fractures in 16 of these cases. Seven patients underwent internal fixation secondary, the so-called “Fix and flap” method. The remaining 9 were fixed externally. There were 10 cases of tibia and fibula fractures, and 6 of tibia fractures only.
Next, we examined the relationship between the period until the wound resurfacing after injury and frequency of postoperative infections for 21 patients with GAIIIB (18 patients) and C (3 patients) fractures. There were 14 cases of tibia and fibula fractures, and 7 of tibia fractures only.
Statistical analysis was performed using the Mann-Whitney U test and calculated them in Microsoft Excel. The value of p< 0.05 was determined as significant. The ethical committee of our medical center approved this study (Sep.5.2022. Approval number 2022077).
Results
• Relationship between postoperative infection and the period until the start of load-walking after injury (Table 1).
Seven patients developed postoperative infection. The period until the start of load-walking rehabilitation after injury in the group that developed infection ranged from 71 to 511 days (average, 285.1 ± 172.7 days), and that in the group not developing infection ranged from 24 to 234 days (average, 61.1 ± 66.4 days). There was a significant difference between the groups (P< 0.05 Mann-Whitney U test)(Figure 1).
• Relationship between the period until the wound resurfacing after injury and frequency of postoperative infections (Table 2).
Table 1: Surgical results for patients with lower leg Gustilo-Anderson IIIB fracture. If osteomyelitis occurs, + is indicated, and if not, - is indicated.
| Age | Days to resurface soft tissue (days) | Load Start (days) | Osteomyelitis | Additional surgery |
|---|---|---|---|---|
| 32 | 0 | 39 | _ | - |
| 33 | 0 | 32 | _ | - |
| 77 | 0 | 24 | _ | - |
| 88 | 2 | 30 | _ | - |
| 50 | 4 | 71 | + | - |
| 80 | 5 | 30 | _ | - |
| 22 | 9 | 31 | _ | - |
| 77 | 10 | 60 | _ | - |
| 54 | 12 | 73 | + | Masquelet technique |
| 74 | 16 | 234 | _ | - |
| 57 | 20 | 214 | + | Masquelet technique |
| 67 | 21 | 511 | + | Vascularized bone graft |
| 54 | 35 | 386 | + | Free bone graft |
| 68 | 46 | 70 | _ | - |
| 43 | 86 | 310 | + | Bone elongation |
| 29 | 180 | 431 | + | Bonne elongation |
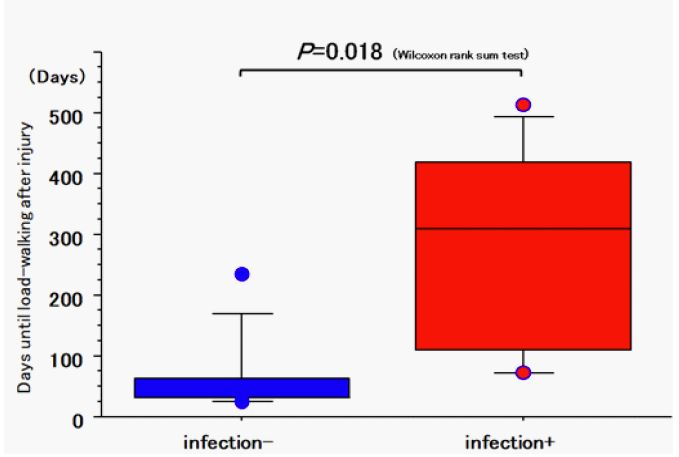
Figure 1: Relationship between the presence or absence of postoperative infection and period until the start of load-walking after lower leg Gustilo-Anderson IIIB fracture.
Table 2: Surgical results for patients with lower leg Gustilo-Anderson IIIB or C fracture. If osteomyelitis occurs, + is indicated, and if not, - is indicated.
| Age | Sex | GA | Wound resurfacing (days) | Osteomyelitis |
|---|---|---|---|---|
| 32 | M | IIB | 0 | _ |
| 77 | M | IIIB | 0 | _ |
| 33 | M | IIIB | 0 | _ |
| 71 | M | IIIB | 0 | _ |
| 64 | M | IIIC | 0 | _ |
| 29 | M | IIIC | 0 | _ |
| 74 | M | IIIC | 0 | _ |
| 88 | F | IIIB | 2 | _ |
| 50 | F | IIIB | 4 | + |
| 80 | M | IIIB | 5 | _ |
| 22 | M | IIIB | 10 | _ |
| 77 | M | IIIB | 16 | _ |
| 74 | M | IIIB | 16 | _ |
| 57 | M | IIIB | 20 | + |
| 67 | M | IIIB | 21 | + |
| 54 | M | IIIB | 35 | + |
| 54 | F | IIIB | 35 | + |
| 56 | M | IIIC | 35 | + |
| 68 | F | IIIB | 46 | |
| 43 | M | IIIB | 86 | + |
| 29 | M | IIIB | 180 | + |
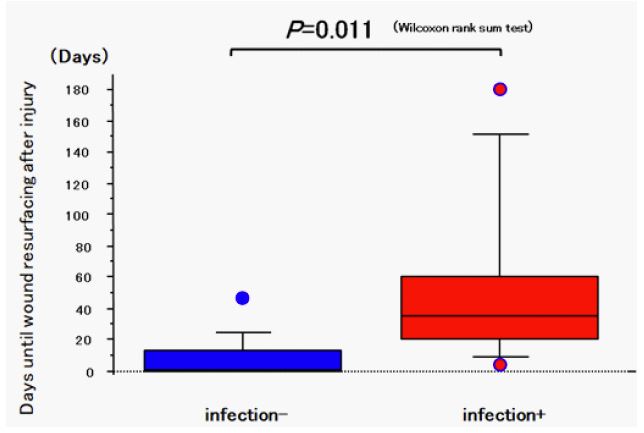
Figure 2: Relationship between the presence or absence of postoperative infection and period until wound resurfacing after lower leg Gustilo-Anderson IIIB or C fracture.
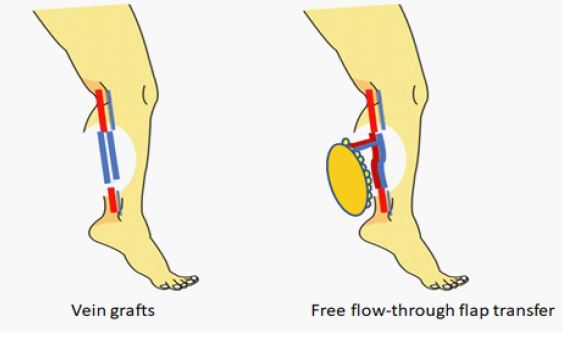
Figure 3: Illustration of vascular reconstruction in Gustilo-Anderson IIIC fracture. Instead of using a venous graft for revascularization, “Flap after Fix” can be performed by simultaneously reconstructing damaged blood vessels and soft tissue with an emergency free flow-through flap.
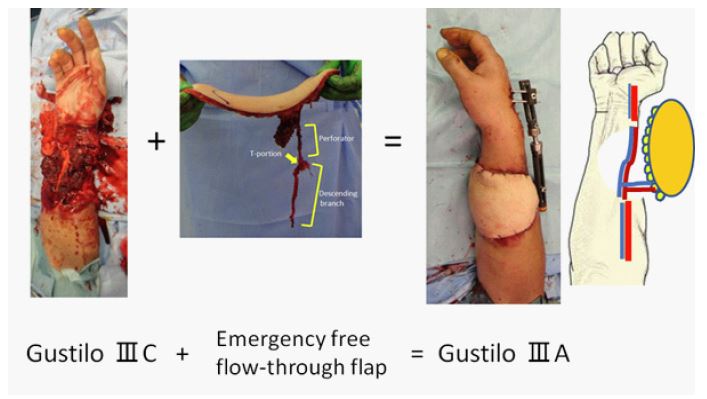
Figure 4: GAIIIC can be converted to GAIIIA by performing simultaneous reconstruction of blood vessels and soft tissues using an emergency free flow-through flap on the day of injury.

Figure 5 a, b: A 61-year-old man was run over by a tractor and suffered a GAIIIB open fracture with a right tibial fibula open fracture, ruptures of gastrocnemius and tibialis anterior muscles, and skin defect involving the right lower leg.
c: Debridement was performed urgently, and bone fixation was conducted by external fixation, but exposed bone wounds remained (circle).
d: On the day of injury, the anterior tibial artery perforator fascial flap was subsequently raised, and the exposed bone wound was covered with a flap.
e: Two days after the initial surgery, the external fixation was converted to an intramedullary nail. Mesh skin grafts were added to the flap donor site.
f: X-ray photograph 7 days after the initial surgery. The tibia was fixed rigidly by an intramedullary nail.
g: 14 days after injury. All wounds were closed, and the patient had already undergone weighted-gait rehabilitation.
c: Debridement was performed urgently, and bone fixation was conducted by external fixation, but exposed bone wounds remained (circle).
d: On the day of injury, the anterior tibial artery perforator fascial flap was subsequently raised, and the exposed bone wound was covered with a flap.
e: Two days after the initial surgery, the external fixation was converted to an intramedullary nail. Mesh skin grafts were added to the flap donor site.
f: X-ray photograph 7 days after the initial surgery. The tibia was fixed rigidly by an intramedullary nail.
g: 14 days after injury. All wounds were closed, and the patient had already undergone weighted-gait rehabilitation.
Eight patients developed postoperative infection. The period until wound resurfacing after injury in the group that developed infection ranged from 4 to 180 days (average, 52.0 ± 56.9 days), and that in the group not developing infection ranged from 0 to 46 days (average, 7.9 ± 13.5 days). There was a significant difference between the groups (P< 0.05 Mann-Whitney U test) (Figure 2).
Seven patients underwent bone-exposed wound resurfacing surgery with flaps on the day of injury, and none developed postoperative infection.
Discussion
One of the keys to treating limb fractures is rigid bone stabilization to prevent non-union. With the development of new intramedullary nails and various plates, this problem has mostly been overcome for GAI, GA II, and GAIII A fractures, which are associated with a lower incidence of infection than GAIII B and C [6,7]. It is known that the risk of developing non-union increases when a postoperative infection develops. Thakore et al. examined the prognosis of 486 patients with open tibia fractures and reported that the inci dence of infection and non-union of GAIII was much higher than that of GAI and GAII. They also reported that the rate of infection was 14% for GAIIIA, 30% for GAIIIB, and 62% for GAIIIC. The rate of non-union was 11% for GAIIIA, 26% for GAIIIB, and 25% for GAIIIC [8]. According to a study by Gustilo et al., the rate of infection in GAIII open fractures ranged between 10 and 50% [9]. Despite advances in antibiotics, surgical procedures, and perioperative management, the tendency for the infection rate to increase as the severity of open fractures increases has continued in recent years. Yeganeh A et al. reported in 2022 about outcomes of open gunshot fractures of long bones with GA III, whereby the rate of infection was 13.5% in GA IIIA, 25% in GAIIIB, and 40% in GA IIIC [10]. Levitt EB et al. investigated 154 patients with open lower extremity fractures after surgery and concluded that patients with GAIII open fractures had a significantly higher risk of infection. In addition, the infected group showed a higher rate of below-knee amputations than the uninfected group [11].
In open fractures, wound infection immediately leads to the development of osteomyelitis. The results of our study showed that patients with postoperative infections develop bone rot and non-union, which required additional surgeries for bone fusion. For this reason, the period until the start of load-bearing walking rehabilitation was significantly longer (Table 1). From the above, it is necessary to have a strategy to prevent postoperative infection, especially in GAIII B and C fractures.
A protocol that includes immediate wound resection, rigid bone stabilization, and early bone exposure wound covering with flaps is called "Fix and Flap" and is currently the most recommended treatment strategy for open fractures. The spread of this method has significantly improved patient outcomes [4,12]. Current evidence indicates that infections of open fractures are not caused by initial contaminating organisms but are acquired in the hospital [13]. Thus, the sooner the wound is closed, the lower the risk of wound infection; therefore, "Single-stage emergent Fix and flap" is an ideal method, and should provide better results by preventing infection [14].
The practically recommended treatment procedure for severe open fractures is as follows: Immediately after injury, temporary external fixation with debridement is performed, followed by conversion to internal fixation and wound closure using flaps (secondary "fixation and flap" surgery) within 72 hours after injury [4]. However, it may be difficult to perform secondary "fixation and flap" surgery within 72 hours. Rymeretal et al. surveyed 78 patients with open fractures of the lower extremities and found that only 56.4% underwent wound coverage within 72 hours. They also reported that the main reasons for the delay in secondary resurfacing surgery were transfer from another hospital, the absence of a plastic surgeon at the first surgery, and a serious general condition of the patient [15].
Fernandez et al. also assessed the course of 48 patients with GAIIIB and IIIC leg fractures and reported that 72-hour secondary soft tissue coverage was achieved in only 54%. These reports show that ideal soft tissue closure surgery within 72 hours was performed in only about half of the cases [16]. These facts indicate that wound coverage within 72 hours of injury is extremely difficult; therefore, the high risk of postoperative infection in severe limb trauma remains.
It is ideal from the viewpoint of infection prevention to be able to perform "emergency Fix and Flap" surgery on the day of injury. One of the reasons why "emergency Fix and Flap" is not possible is that intramedullary nails and plates of appropriate shape and size for various fracture sites and shapes are not always available. However, even in such cases, open fracture treatment always requires wound irrigation, debridement, and at least external fixation as primary surgery. The idea of "Fix after Flap" is to cover the exposed bone surface with a flap during this initial surgery without waiting for rigid fixation of the bone. Surprisingly, this method is practical for the more severe cases of GAIIIC fractures, which generally require immediate repair of damaged vessels by venous transplantation to save the limbs. By inserting free flow-through flap vessels into the distal and proximal ends of the injured vessel instead of venous transplantation, blood flow in the distal extremities can be maintained, while soft tissue can rapidly resurface exposed bone wounds (Figure 3).
This operation can markedly convert GAIIIC to GAIIIA in the first surgery on the day of injury (Figure 4) [17,18].
When performing immediate free flow-through flap transfer for GAIIIC fracture, we frequently use an anterolateral thigh flap as the first choice for flaps. The reason is that this flap is ideal for limb reconstruction as it can provide a large skin paddle, has long flow-through vessels, does not require intraoperative repositioning, and minimizes donor site sacrifice [19-21].
On the other hand, when performing the "Fix after Flap" method for GAIIIB fractures, the flap does not necessarily have to be a free flap. Penetrating branch flaps, muscular flaps, and fascial flaps can be selected according to the degree of damage to the surrounding soft tissue. It is possible to select pedicle flaps, such as perforator flaps, muscular flaps, and fascial flaps, depending on the degree of damage to the surrounding soft tissue (Figure 5).
Even if it becomes necessary to plate-fix the fractured part in the secondary surgery, there is no problem in removing the flap covering the bone to expose the bone surface. After fixing the plate, it can be covered with a flap again. The only point to note in "Fix after Flap" is that there is a risk of flap necrosis due to delayed vasoconstriction and thrombus formation, as the vessel is manipulated in the zone of injury during flap harvesting or mobilization.
Conclusion
Although secondary "Fix and Flap" surgery in GA III B and C fractures has been recommended to be performed within 72 hours, this was achieved in less than 40% of all cases causing many postoperative infections. On the other hand, the 7 cases in which the wound was closed on the day of the injury showed a good course without any postoperative infection. These are "emergency Fix and Flap" or "Fix after Flap" cases in which wound closure was performed prior to rigid bone fixation. We believe that "Fix after Flap" is a useful option to reduce the frequency of infections that affect the prognosis of patients with severe limb trauma.
Declarations
Conflict of interest and source funding: Author (Masaki Fujioka) have not received conflicts of interest and sources of funding, including financial, consultant, institutional and other relationships.
Acknowledgment: None
Financial Disclosures: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
This paper had not been presented in any academic conference, but presented at The 19th Kyushu Congress of The Pressure Ulcer (2022.5.14, Miyazaki, Japan).
Ethical considerations: The procedures followed were in accordance with the ethical standards of our institutional committee on human experimentation and with the Helsinki . Patient in this manuscript were informed about the patient’s ethical rights by the author, and agreed that the patient’s illustrative material, including face, could be used for the aim of the medical study, and also agreed to the photos being published in a medical journal.
Running head: Colostomy for rectum exposing wound.
References
- Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: Retrospective and prospective analyses. J Bone Joint Surg Am. 1976; 58: 453-458.
- Fochtmann A, Binder H, Rettl G, Starlinger, Aszmann O, Sarahrud K, et al. Third degree open fractures and traumatic sub-/total amputations of the upper extremity: Outcome and relevance of the Mangled Extremity Severity Score.Orthop Traumatol Surg Res. 2016; 102(6): 785-790.
- Fochtmann A, Mittlböck M, Binder H, Köttstorfer J, Hajdu S. Acute Care Surg.Potential prognostic factors predicting secondary amputation in third-degree open lower limb fractures. J Trauma. 2014; 76(4): 1076-1081.
- Gopal S, Majumder S, Batchelor AG, Knight SL, De Boer P, Smith RM. Fix and flap: The radical orthopaedic and plastic treatment of severe open fractures of the tibia. J Bone Joint Surg Br. 2000; 82(7): 959-966.
- Soni A, Tzafetta K, Knight S, Giannoudis PV. Gustilo IIIC fractures in the lower limb: our 15-year experience. J Bone Joint Surg Br. 2012; 94: 698-703.
- Ogunlusi J, Olasinde A, Ikem I, Davids T. Gunshot fractures of tibia and femur-excellent results with reamed bone marrow graft and interlocking nailing. East African Medical Journal. 2011; 88(10): 337-343.
- Hilton T, Kruger N, Wiese K, Martin C, Maqungo S. Gunshot tibia fractures treated with intramedullary nailing: A single centre retrospective review. SA Orthopaedic Journal. 2017; 16(1): 32-38.
- Thakore RV, Francois EL, Nwosu SK, Attum B, Whiting PS, Siuta MA, et al. The Gustilo–Anderson classification system as predictor of nonunion and infection in open tibia fractures. European Journal of Trauma and Emergency Surgery. 2017; 43(5): 651-656.
- Gustilo RB, Mendoza RM, Williams DN. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. The Journal of trauma. 1984; 24(8): 742-746.
- Yeganeh A, Amiri S, Otoukesh B, Moghtadaei M, Sarreshtedari S, Daneshmand S, et al. Arch Characteristic Features and Outcomes of Open Gunshot Fractures of Long-bones with Gustilo Grade 3: A Retrospective Study. Bone Jt Surg. 2022; 10(5): 453-458.
- Levitt EB, Patch DA, Johnson MD, McLynn R, Debell H, Harris JB, et al. What Are the Risk Factors for Infection After Operative Treatment of Peritalar Fracture Dislocations? J Orthop Trauma. 2022; 36(5): 251-256.
- Mehta S, Williams W. Fix and flap: the radical orthopaedic and plastic treatment of severe open fractures of the tibia. J Bone Joint Surg Br. 2001; 83(5): 773-774.
- Weitz-Marshall AD, Bosse MJ. Timing of closure of open fractures. J Am Acad Orthop Surg. 2002; 10: 379-384.
- Singh J, Dhillon MS, Dhatt SS. Malays Orthop J.Single stage "Fix and Flap" gives Good Outcomes in Grade 3B/C Open Tibial Fractures: A Prospective Study. Malays Orthop J. 2020; 14(1): 61-73.
- Rymer B, Dimovska EOF, Chou DTS, Choa R, Davis B, Huq S. A representative assessment of the management of open fractures of the lower limb within UK orthoplastic centres: A two-centre audit of compliance with national standards. Injury. 2017; 48(10): 2266-2269.
- Fernandez MA, Wallis K, Venus M, Skillman J, Young J , Costa ML. The impact of a dedicated orthoplastic operating list on time to soft tissue coverage of open lower limb fractures. Ann R Coll Surg Engl. 2015; 97(6): 456-459.
- Fujioka M, Hayashida K, Murakami C. Artificial dermis is not effective for resurfacing bone-exposing wounds of Gustilo-Anderson III fracture. J Plast Reconstr Aesthet Surg. 2013; 66(4): e119-121.
- Soutar DS, Scheker LR, Tanner NS, McGregor IA.The radial forearm flap: a versatile method for intra-oral reconstruction.Br J Plast Surg. 1983; 36(1): 1-8.
- Koshima I, Fujitsu M, Ushio S, Sugiyama N, Yamashita S. Flow-through anterior thigh flaps with a short pedicle for reconstruction of lower leg and foot defects. Plast Reconstr Surg. 2005; 115(1): 155-162.
- Fujioka M.Application of free flow-through anterolateral thigh flap for the reconstruction of an extremity soft tissue defect requiring vascularization. In:Sherif A, editor. Flap surgery. Chapter 4. London: InTech. 2018; 51-76.
- Fujioka M. Emergent or early flap resurfacing is required for the bone-exposing wounds of Gustilo-Anderson IIIB and C fractures. In:Sherif A, editor. Flap surgery. Chapter 5. London: InTech. 2018; 78-100.
