
Open Access, Volume 9
A case of Lemierre syndrome with a delayed response and a fatal outcome due to a false-positive diagnosis of COVID-19
Yoshihisa Fujinami*; Mariko Hatada; Keiichirou Yamaguchi; Keiji Sato; Manabu Kirita
Department of Emergency Medicine, Kakogawa Central City Hospital, Japan.
Yoshihisa Fujinami
Department of Emergency Medicine, Kakogawa Central City Hospital, Japan.
Email: greatyoppie@yahoo.co.jp
Received : June 09, 2023,
Accepted : July 05, 2023
Published : July 10, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Five days prior to the presentation, a 25-year-old male was diagnosed with mild coronavirus disease (COVID-19) in a clinic and was undergoing home-based treatment. The patient was not obese, and his medical history included only pediatric asthma. Two days, he experienced chest pain and respiratory distress, which gradually exacerbated; therefore, an ambulance was summoned to his location. Saturation for peripheral oxygen was 93% (room air) to 97% (nasal cannula, 2 L/min), and the hypoxia was not severe. However, tachypnea was prominent, the patient exhibited signs of shock and he appeared unwell. Moreover, the patient was septic and a computed tomography scan revealed septic embolisms in his lung bilaterally and a low-density intra-luminal thrombus within his left jugular vein. He was diagnosed with sepsis secondary to Lemierre Syndrome (LS). Unfortunately, despite receiving intensive care, the patient died within a day.
We report a case of LS that was affected by the COVID-19 pandemic and had an unfortunate outcome owing to delayed diagnosis and consultation.
Keywords: Lemierre syndrome; COVID-19; Delayed diagnosis; Sepsis.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Fujinami Y (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Fujinami Y, Hatada M, Yamaguchi K, Sato K, Kirita M. A case of Lemierre syndrome with a delayed response and a fatal outcome due to a false-positive diagnosis of COVID-19. Open J Clin Med Case Rep. 2023; 2067.
Introduction
Lemierre Syndrome (LS) is a rare and critical complication of anaerobic bacteremia primarily caused by pharyngitis or tonsillitis [1]. LS can commonly affect young healthy individual. Although the incidence of LS is very low (1–2 per million), the mortality rate is reported to be as high as 20% [2].
We report a case of LS that was affected by the coronavirus disease (COVID-19) pandemic and had an unfortunate outcome owing to delayed diagnosis and consultation.
Case Presentation
Five days prior to the presentation, a 25-year-old male received a diagnosis of mild COVID-19 in a clinic and was undergoing home-based treatment. The patient was not obese and his medical history included only pediatric asthma. Two days earlier, he experienced chest pain and respiratory distress, which gradually aggravated; therefore, an ambulance was summoned to his location.
Vital signs on arrival are displayed in Table 1 and arterial blood gas analysis is presented in Table 2. Hypoxia was not severe; however, tachypnea was prominent. The patient was in a state of shock state and exhibited cold sweats and livedo reticularis.
Table 1: Vital signs on arrival.
| Blood Pressure | 115/50 | mmHg |
|---|---|---|
| Pulse Rate | 145 | /minute |
| Respiratory Rate | 40 | /minute |
| SpO2 | 93 (Room Air) →97 (nasal 2L/min.) |
% |
| Body Temperature | 36.7 | ℃ |
| Glasgow Coma Scale | 15 |
Table 2: Arterial Blood Gas Analysis.
| pH | 7.118 | |
|---|---|---|
| PaCO2 | 31.5 | mmHg |
| PaO2 | 96.0 | mmHg |
| HCO3- | 10.0 | mmol/L |
| Glucose | 98 | mg/dL |
| Lactate | 10.88 | mmol/L |
mmol: millimole; mg: milligram
The results of the blood tests and Computed Tomography (CT) scans are displayed in Table 3. The levels of inflammatory markers displayed a significant increase, whereas the markers of renal function and coagulation were also severely impaired. Plain CT scan revealed multiple bilateral shadows in the lungs (Figure 1). We assessed multiple organ failure as a result of sepsis caused by soft tissue infection or pneumonia of the COVID-19. However, contrast-enhanced CT revealed a low-density intraluminal thrombus in the left jugular vein (Figure 2). We diagnosed LS and assessed lung shadows and soft tissue swelling as secondary findings.
Table 3: Blood test.
| White blood cells | 36.67 | 103/mcL |
| Hemoglobin | 16.1 | g/dL |
| Hematocrit | 46.4 | % |
| Platelets | 3 | 103/mcL |
| C reaction protein | 30.67 | mg/dL |
| AST | 115 | U/L |
| ALT | 63 | U/L |
| Alkaline phosphatase | 670 | U/L |
| Creatine kinase | 1,647 | U/L |
| Total Bilirubin | 16.5 | mg/dL |
| Direct Bilirubin | 14.8 | mg/dL |
| Blood urea nitrogen | 108.1 | mg/dL |
| Creatinine | 3.79 | mg/dL |
| Sodium (Na+) | 136 | mmol/L |
| Potassium (K+) | 4.5 | mmol/L |
| Chloride (Cl-) | 91 | mmol/L |
| PT-INR | 1.29 | |
| APTT | 31.4 | second |
| D-dimer | 1.5 | mcg/mL |
mcL: microliters; mg: milligram; dL: deciliter; mmol: millimole; mcg: microgram; ALT: Alanine aminotransferase; PT-INR: Prothrombin Time-International Normalized Ratio; APTT: Activated Partial Prothrombin time.
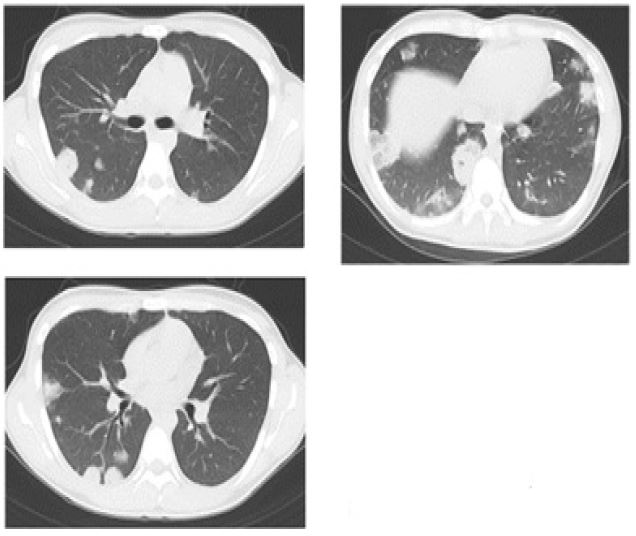
Figure 1: The plain CT scan revealed multiple shadows in the bilateral lung.
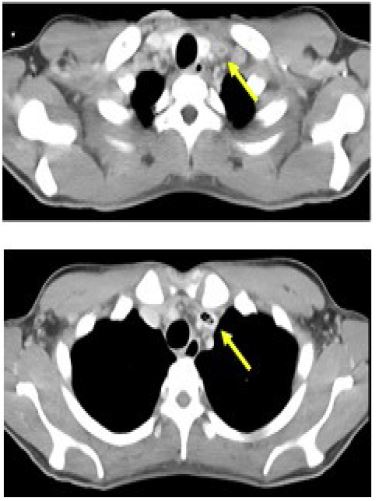
Figure 2: The contrast-enhanced CT revealed a low-density intra-luminal thrombus with in the left jugular vein.
During the course of the emergency care, the patient’s blood pressure demonstrated a downward trend and tracheal intubation and vasopressor administration were initiated. The patient was admitted to the Intensive Care Unit (ICU); however, sepsis progressed, and he died 8 h after admission. Upon admission to the ICU, antigen, and Polymerase Chain Reaction (PCR) tests for COVID-19 were negative.
Discussion
In the present case, a young man with no apparent comorbidities presented to the emergency room on the 5th day of the COVID-19 outbreak. Although the patient experienced respiratory distress, there was no significant drop in saturation for peripheral oxygen (SpO2). However, on direct examination symptoms of shock were observed. The right upper arm appeared erythematous and swollen on physical examination, and a soft tissue infection was suspected, but there was no wound on the skin that might have been a portal of entry. A CT scan revealed scattered bilateral round mass shadows. An internal jugular vein thrombus was identified, and LS was strongly suspected. The patient was treated for LS-associated sepsis. Intensive care was continued, but unfortunately, the patient died of multiple organ failure 12 h later.
The diagnostic criteria for LS include 1) infection of the oropharynx by anaerobic bacteria, 2) bacteremia, 3) thrombophlebitis of the internal jugular vein, and 4) the presence of a remote infection site [3]. In the present case, a blood culture test revealed that the pathogen causing bacteremia was Fusobacterium necrophorum, which is a reasonable cause of LS [4]. The other criteria were also met in the aforementioned case.
LS was a serious disease with a fatality rate of approximately 90% [5] before the widespread use of antimicrobial therapy. The rate of LS has improved in recent years to approximately 5% and it has come to be called "the forgotten disease," [6]; however, case reports have been published constantly. Since the 1990s, the incidence of LS has increased, which is believed to be related to a decrease in the frequency of antimicrobial use for pharyngitis [7]. In recent years, there have been infrequent reports of LS cases associated with COVID-19 [8-10], and we believe that the present case was also associated with the COVID-19 treatment system and pathophysiology.
In Japan, the criteria for determining the severity of COVID-19 and the indications for hospitalization were first assessed using SpO2 and comorbidities. In many clinics, the screening is performed first, and if the disease severity is mild, a face-to-face consultation is omitted and the patient is provided with symptomatic prescriptions.
The most common symptoms of COVID-19 is a sore throat and most patients do not actively seek medical attention with a sore throat as their primary complaint, especially those who are young. Moreover, even when patients seek medical attention, pharyngeal observations are often excluded to avoid exposure to aerosols.
The case was finally diagnosed as a COVID-19 false-positive case. The PCR test performed at the health center 5 days before the visit was positive, whereas the PCR and antigen tests performed at our hospital on the day of the visit were negative. In general, PCR tests for COVID-19 have a sensitivity of 70%–90% and a specificity of 99% or higher [11,12], whereas antigen tests have a sensitivity of 50%–80% and a specificity of 99% or higher, depending on the test kit [13,14]. As this case occurred following the peak of the outbreak period of Omicron strains, the exact prevalence is unknown, and the negative predictive value cannot be calculated. However, even if the prevalence was overestimated by 1%, it is reasonable to conclude that the patient was a false-positive, with a positive predictive value of approximately 50% and a negative predictive value of >99%.
Patients often complain of difficulty with oral intake during home care due to sore throats. Moreover, such patients do not adequately maintain oral hygiene, including tooth brushing. Exposure to oral bacteria may be very critical due to pharyngeal swelling and mucosal inflammation caused by viral pharyngitis.
LS in young patients is a universal complication of acute upper respiratory tract infections, therefore, the pathogen-specific impact of COVID-19 needs to be considered separately. However, we suggest that the issue, in this case, was not whether he had COVID-19 but rather the fact that he missed the opportunity to be examined because of the altered system of care due to COVID-19.
Conclusion
While oral and neck examinations are becoming hesitant because of the COVID-19 pandemic, Lemierre syndrome should be considered as a possibility.
References
- Lemierre A. On certain septicemias due to anaerobic organisms. The Lancet. 1936; 227: 701-703.
- Riodan T, Wilson M. Lemierre’s syndrome: More than a historical curiosa. Postgrad Med J. 2004; 80: 328-336.
- Sinave CP, Hardy GJ, Fardy PW. The Lemierre’s syndrome: suppurative thrombophlebitis of the internal jugular vein secondary to oropharyngeal infection. Medicine. 1989; 68: 85-94.
- Johannesen K, Bodtger U. Lemierre’s syndrome: Current perspectives on diagnosis and management. Infect Drug Resist. 2016; 9: 221-227.
- Karkos PD, Asrani S, Karkos CD, Leong SC, Theochari GT, Alexopoulou TD, et al. Lemierre’s Syndrome: A Systematic review. Laryngoscope 2009; 119: 1552-1559.
- Gupta T, Parikh K, Puri S, Agrawal S, Agrawal N, Sharma D, et al. The forgotten disease: bacterial lemierres disease with mycotic aneurysm of the vertebral artery. Am J Case Rep. 2014; 15: 230-234.
- Ramirez S, Hild TG, Rudolph CN, Sty JR, Kehl SC, Havens P, et al. Increased Diagnosis of Lemierre Syndrome and Other Fusobacterium necrophorum Infections at a Children’s Hospital. Pediatrics. 2003; 112: 380-385.
- Soares C, Blackwood K, Vecchio M, Francis ER, Zhu S, Johnson J. Diagnosing Lemierre’s Syndrome as the Cause of Multifocal Pneumonia During the COVID-19 Pandemic. RHODE ISLAND MEDICAL JOURNAL. 2021
- Costa F, Matos BM, Ferreira I, Rodrigues CC, Silva AA. Not all Pulmonary Densifications Are COVID-19: A Case Report About Lemierre’s Syndrome. Cureus. 13: e15984.
- Dai YL, Chen VM, Hedges TR, Malek A. Lemierre syndrome associated mycotic cavernous sinus thrombosis and carotid aneurysm after COVID-19. American Journal of Ophthalmology Case Reports. 2022; 27: 101642.
- Udugama B, Kadhiresan P, Kozlowski HN, Malekjahani A, Osborne M, Li VYC, et al. Diagnosing COVID-19: the disease and tools for detection. ACS Nano. 2020; 14: 3822-3835.
- Fang Y, Zhang H, Xie J, Lin M, Ying L, Pang P, et al. Sensitivity of chest CT for COVID-19: comparison to RT-PCR. Radiology. 2020; 296: E115-E117.
- Pekosz A, Parvu V, Li M, Andrews JC, Manabe YC, Kodsi S, et al. Antigen-based testing but not real-time polymerase chain reaction correlates with severe acute respiratory syndrome coronavirus 2 viral culture. Clinical infectious diseases. 2021; 73: e949-e950.
- Dinnes J, Deeks JJ, Adriano A, Berhane S, Davenport C, Dittrich S, et al. Rapid, point‐of‐care antigen and molecular‐based tests for diagnosis of SARS‐CoV‐2 infection. Cochrane Database of Systematic Reviews. 2021.
