
Open Access, Volume 9
Multicentric castleman disease in a HIV patient
Aashna Gandhi1*; Rahul Doshi2; Hrishita Kothavade3; S Shrividya4; Tushar Patil5; Rajeev Soman6
1Infectious Diseases Fellow, Department of Infectious Diseases, Jupiter Hospital, Pune, India.
2Consultant Physician, Department of General Medicine, Jupiter Hospital, Pune, India.
3HOD & Consultant Pathologist, Department of Pathology, Jupiter Hospital, Pune, India.
4Consultant Pathologist, Opal Histopathology Center, Pune, India.
5Consultant Oncologist, Department of Oncology, Jupiter Hospital, Pune, India.
6HOD & Consultant ID Physician, Department of Infectious Diseases, Jupiter Hospital, Pune, India.
Aashna Gandhi
Infectious Diseases Fellow, Department of Infectious Diseases, Jupiter Hospital, Pune, India.
Tel: +91-987-001-8310;
Email: aashnagandhi2206@gmail.com
Received : April 27, 2023,
Accepted : June 19, 2023
Published : June 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
A 63 year old newly diagnosed HIV positive male patient had presented with a history of fever and weight loss for 3 months, as well as generalized lymphadenopathy. Inguinal lymph node biopsy revealed features of Castleman disease. Immunohistochemistry revealed +ve staining for EBV and -ve staining for HHV-8. The patient was diagnosed to have idiopathic Multicentric Castleman disease, and treatment with antiretroviral therapy led to complete resolution of lymphadenopathy
Keywords: HIV; Fever; Disease
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Gandhi A (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Gandhi A, Doshi R, Kothavade H, Shrividya S, Patil T, et al. Multicentric castleman disease in a HIV patient. Open J Clin Med Case Rep. 2023; 2059.
Introduction
A patient afflicted with HIV is at a risk of numerous opportunistic diseases. Generalized lymphadenopathy, a manifestation of HIV itself, has a host of differential diagnoses. Multicentric Castleman disease is a rare lymphoproliferative disorder associated with HIV as reported in this case.
Case Presentation
A 63 year old male patient who had recently been diagnosed with HIV, presented with a history of fever and weight loss of 8 Kgs over 3 months. Examination revealed lymphadenopathy in cervical, axillary and inguinal regions. The baseline HIV viral load was 29,50,000 copies/ml and CD4 was 132 cells/microl (7.85%). VDRL and TPHA were positive. PET CT revealed multiple enlarged lymph nodes (Figure 1).
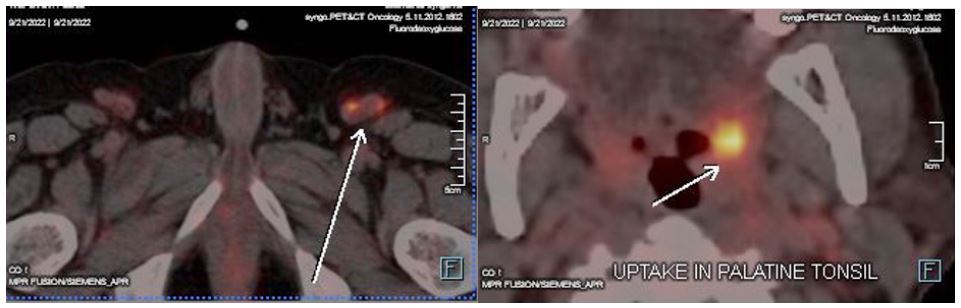
Figure 1: PET CT: FDG avid left inguinal node with an SUV Max of 11.06 (left) and FDG avid asymmetric uptake in left palatine
tonsil with an SUV Max of 12.87 (right).
Several differential diagnoses were considered at this point:
1. Tuberculosis
2. HIV related lymphadenopathy
3. Non-tuberculous mycobacterial infection
4. Secondary syphilis
5. Lymphoproliferative disorder
The patient received Inj Ceftriaxone 2 g IV BD for suspected late latent syphilis. A biopsy was performed from the left inguinal lymph node and relevant investigations were sent for the above differential diagnoses. Histopathological examination revealed interfollicular plasmacytosis, atretic lymphoid follicles with penetrating vessels, interfollicular zones with prominent proliferation of high endothelial venules and focal endothelial necrosis/apoptosis. All these features were suggestive of Castleman Disease. An immunohistochemistry was performed, which was negative for HHV-8 and positive for EBV. Figures 2, 3 and 4 describe the histopathological feature in detail.
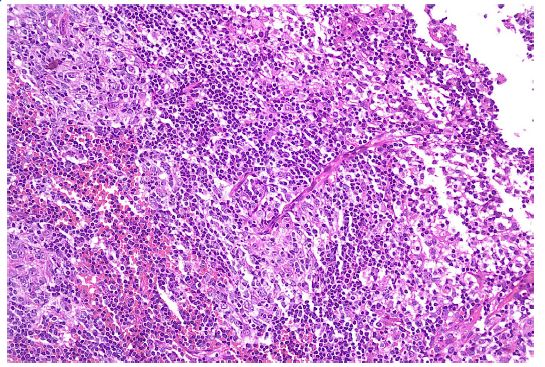
Figure 2: Atretic lymphoid follicles with penetrating vessels
(Low power magnification).
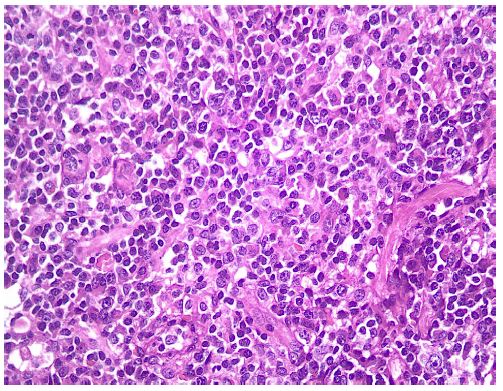
Figure 3: Increased number of plasma cells (High
power magnification).
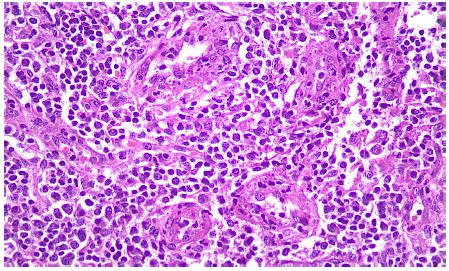
Figure 4: Interfollicular zone with prominent proliferation of high endothelial
venules and focal endothelial necrosis/ apoptosis (High power magnification).
Hence, he was diagnosed to have EBV +ve, HHV8 -ve, idiopathic Multicentric Castleman disease. The patient was started on antiretroviral therapy (Tenofovir alafenamide fumarate 25 mg + Emtricitabine 200 mg + Dolutegravir 50 mg) after diagnosis. No chemotherapy was used. After 6 months, he had complete resolution of symptoms, reduction in HIV viral load to 408 copies/ml, improvement in CD4 to 204 cells/ microl (10%) and PET CT showed a complete radiologic and metabolic resolution of the lesions (Figure 5).
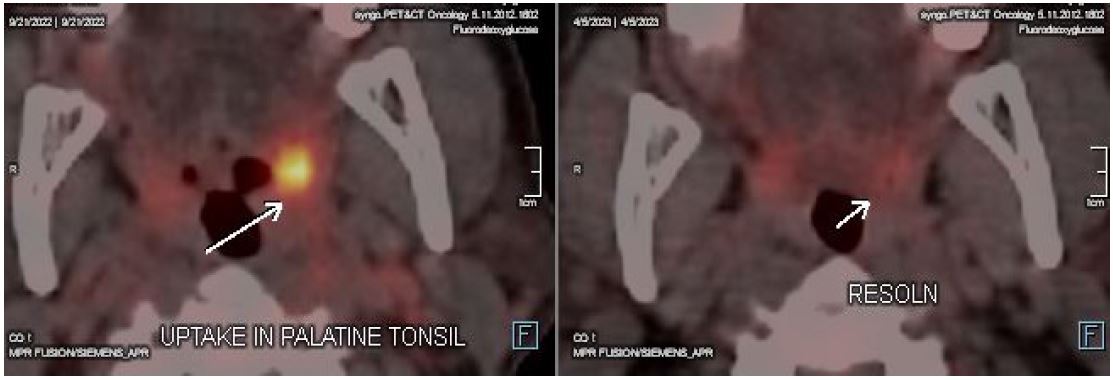
Figure 5: Complete resolution of enlarged left inguinal lymph node (top) and palatine tonsil (bottom). Left side of the
image shows the old PET CET and right side shows the new PET CT, after 6 months.
Discussion
Castleman Disease (CD) includes a heterogenous group of lymphoproliferative disorders that share common histopathological features. Multicentric Castleman Disease (MCD) can be HHV-8 or KSV (Kaposi Sarcoma Virus) +ve, which is the most common MCD associated with HIV, or HHV-8 –ve / idiopathic MCD (iMCD). Disease in Indian patients may be HHV-8 –ve, but +ve for EBV [1], as seen in this patient and may have a role in causation. The primary treatment for MCD is chemotherapy. HHV-8 +ve patients are treated with Rituximab, while HHV-8 –ve patients are treated with Siltuximab as the first line chemotherapy agents [2]. Considering the high risk of infectious complications following cytotoxic therapy in the AIDS population, patients with AIDS-related MCD may be first managed with antiretroviral therapy, leaving more aggressive therapeutic approaches for patients if relapse occurs [3]. There are multiple case reports of HIV associated MCD being treated with just antiretroviral therapy, without chemotherapy [4,5], as we did in this patient, and led to complete resolution of signs and symptoms.
References
- Bhanvadia V, Shet T, Rao V, Epari S, Gujral S, et al. Multicentric Castleman’s disease in India-Does EBV rather than HHV8 play a role?. Indian Journal of Pathology and Microbiology. 2021; 64: 302.
- Dispenzieri A, Fajgenbaum DC. Overview of Castleman disease. Blood. 2020; 135: 1353-1364.
- Sprinz E, Jeffman M, Liedke P, Putten A, Schwartsmann G. Successful treatment of AIDS-related Castleman’s disease following the administration of Highly Active Antiretroviral Therapy (HAART). Annals of oncology. 2004; 15: 356-358.
- Lee SM, Edwards SG, Chilton DN, Ramsay A, Miller RF. Highly active antiretroviral therapy alone may be an effective treatment for HIV-associated multi-centric Castleman’s disease. Haematologica. 2010; 95: 1979
- Lanzafame M, Carretta G, Trevenzoli M, Lazzarini L, Concia SV. CASE REPORT: Successful Treatment of Castleman’s Disease with HAART in Two HIV-Infected Patients. Journal of Infection. 2000; 40: 90-91.
