
Open Access, Volume 9
MIS-A: Beware of non-lymphoma
Cantoni S1; Greco R1; Mancini V1; Russo V2; Capasso A1; Travi G3; Vanzulli A4,5; Cairoli R1,6*
1Department of Haematology, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy.
2Department of Energy, Politecnico di Milano, Milan, Italy.
3Division of Infectious Diseases, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy.
4Department of Medical Physics, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy.
5Department of Oncology and Haemato-oncology, University of Milan, Milan, Italy.
6Department of Medicine and Surgery, University of Milano-Bicocca, Monza, Italy.
Cairoli Roberto
Department of Medicine and Surgery, University of Milano-Bicocca, Monza, Italy.
Tel: 0039-0264442668;
Email: roberto.cairoli@ospedaleniguarda.it
Received : April 27, 2023,
Accepted : June 16, 2023
Published : June 20, 2023,
Archived : www.jclinmedcasereports.com
Keywords: SARS-CoV-2; MIS-A; Lymphoma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Cairoli R (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Cantoni S, Greco R, Mancini V, Russo V, Capasso A, Travi G, Cairoli R, et al. MIS-A: Beware of non-lymphoma. Open J Clin Med Case Rep. 2023; 2058.
Short Report
Multisystem Inflammatory Syndrome (MIS) is an acute and serious sequela of SARS-CoV2 infection characterized by a dysregulated systemic immune and inflammatory response which has been associated with SARS-CoV-2 disease and vaccines [1].
From a clinical standpoint, it may be difficult to properly manage these patients who are acutely ill and in need of prompt medical intervention, but whose treatment, although urgent, ought to be nevertheless appropriate.
We report on a young adult patient who developed severe systemic symptoms shortly after receiving a booster dose of SARS-CoV-2 mRNA-based vaccine. Early recognition of MIS-A avoided unnecessary invasive diagnostic procedures and inappropriate treatment.
This 50 year old female patient presented with prominent constitutional symptoms and fever not responsive to empiric azithromycin and NSAIDs and requiring hospital admission.
Her past history was uneventful, other SARS-CoV2 infection two months before (just running nose). She had received the 2nd SARS-CoV-2 mRNA vaccine booster a week before onset of symptoms and on admission nasopharyngeal swab for SARS-Co-V-2 PCR tested weakly positive. Of notice, the rest of her family tested positive for SARS-CoV-2 the day after her vaccination. Upon arrival she appeared acutely ill, with an ECOG PS of 3. Her temperature was 39°C and laboratory tests were consistent with a systemic inflammatory reaction: CRP 6 mg/dl, ESR 123 mm/h, albumin 1,98 g/dl, fibrinogen 506 mg/dL, ferritin 388 ng/ml, IL6 98 pg/ml, Hb 7,8 g/dl, plt count up to 849 x 109/L. Procalcitonin, LDH and lactate remained within normal range. Alkaline phosphatase and GGT were elevated, up to 309 and 587 U/L respectively.
Testing for EBV and CMV genomes was negative. ANA, ENA, LAC and IgG4 titers were normal. SARS-CoV-2 antibodies testing showed high anti-spike antibodies (38.935 AU/mL), anti-nucleocapsid antibodies were negative.
Bone marrow examination was not diagnostic for hematological disorders. A CT scan revealed bilateral pleural effusions, retroperitoneal and mesenteric lymphadenopathy (maximum diameter of 18 mm), and hepatosplenomegaly (spleen maximum diameter of 15 cm).
Hypoxemic respiratory failure developed on day + 8, requiring ICU admission and non-invasive respiratory support and thoracentesis. Empiric antibiotic therapy with piperacillin/tazobactam and vancomycin again did not result in clinical improvement. Underlying lymphoma was hypothesized and TC/PET was performed on day + 12. Increased uptake (max SUVs 7.34) in the retroperitoneal area and perivisceral adipose tissue was found; cervical, mediastinal and inguinal lymph nodes were also weakly positive (Figure 1).
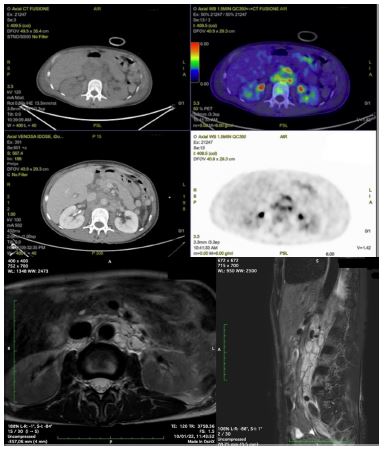
Figure 1: (a) CT/PET total body showing a retroperitoneal mass with increased uptake (SUVs 7.34) in the periaortic area at L1-L3 level. (b) T2w MRI acquisition in sagittal and axial plane: the detection of T2 high intensity inflammatory tissue around enlarged limphonods (arrow) suggest the possible diagnosis of immune related pathology
Because of critical clinical condition, imaging suggestive for a reactive nature of lymphadenopathy and need of an invasive surgical approach, lymph node biopsy was postponed.
The patient slowly recovered without further therapy and was afebrile by day + 16; lab tests improved and splenomegaly and lymphadenopathy were no longer present at an abdomen ultrasound performed on day + 19. She was discharged on day + 22 with a final diagnosis of vaccine-associated MIS-A. Complete recovery was confirmed at the 2 month follow up visit.
Although the SARS-Cov-2 pandemic appears to be resolving world-wide, still this virus has not been and probably never will be eradicated. One lesson that has been learned from this pandemic is that SARS-CoV-2 infection is often associated with sustained dysregulation of adaptive and innate immunity giving rise to a spectrum of clinical manifestations which go beyond the acute, direct effect of the virus on tissues [2-5].
Moreover, several cases of new-onset or re-exacerbation of pre-existing autoimmune disorders have been reported to be associated with mRNA-based SARS-CoV-2 vaccines [6].
Multisystem inflammatory syndrome (MIS) is a rare and poorly understood post-acute, post- infection complication associated with SARS-CoV-2. Its pathogenesis is at present unknown but it is thought to be the result of a delayed immune dysregulated response to a recent infection thus being broadly classified in the growing group of hyperinflammatory syndromes.
It was firstly described in children (MIS-C) and later on also in the adult population (MIS-A) albeit more rarely. MIS-A has also been described following COVID-19 vaccination [1].
This association appears to be exceedingly rare, with only few cases described [7], an instance which makes its diagnosis challenging. This latter instance appears to be the case of our patient who, contrary to prevailing epidemiology [7], was of female gender and Caucasian. Constitutional symptoms and associated involvement of lymph nodes and spleen were suggestive of underlying lymphoma. However, the disproportional increase of inflammation markers leads us to question this hypothesis and search for and alternative diagnosis. In this specific case, it can be speculated that the combined immunological stimulus resulting from exposure to SARS-CoV-2 in infected family members and the concomitant vaccination may have elicited the severe inflammatory reaction observed. Of note, albeit severe, this reaction subsided spontaneously in approximately 3 weeks without need for specific treatment.
Recognition of the association between MIS-A and SARS-CoV-2 vaccines is important in view of the potential risk of MIS-A recurrence following repeat vaccination after recovery.
Declarations
Authors contributions: Cantoni Silvia: Design and conceptualized study; drafted the manuscript for intellectual content. Major role in the acquisition of data. Greco Rosa: Revised the manuscript for intellectual content. Mancini Valentina: Revised the manuscript for intellectual content. Russo Valeria: Revised the manuscript for intellectual content. Capasso Antonella: Revised the manuscript for intellectual content. Travi Giovanna: Revised the manuscript for intellectual content. Vanzulli Angello: Revised the manuscript for intellectual content. Cairoli Roberto: Design and conceptualized study; drafted the manuscript for intellectual content.
Funding/support: none
Conflict of interest disclosures: The authors declare that they have no competing interests for this work. No conflicts of interest declared. The data support the findings of this study of this are available from the corresponding author upon reasonable request. The participant provided written informed consent for data publication.
References
- Belay ED, Cato SG, Rao AK, Abrams J, Wyatt Wilson W, et al. Multisystem Inflammatory Syndrome in adults after severe Acute Respiratory Syndrome Coronavirus 2 (SARSCoV-2) infection and Coronavirus Disease 2019 (COVID-19) vaccination. Clin Infect Dis. 2022; 75: e741-e748.
- Files JK, Boppana S, Perez MD, Sarkar S, Lowman KE, et al. Sustained cellular immune dysregulation in individuals recovering from SARS-CoV-2 infection. J Clin Invest. 2021; 131: e140491
- Rodrigueza Y, Novellib L, Rojas M, Santis MD, Acosta-Ampudia Y, et al. Autoinflammatory and autoimmune conditions at the crossroad of COVID-19. J Autoimmunity. 2020; 114: 102506.
- Ehrenfelda M , Tincani A, Andreoli L, et al. Covid-19 and autoimmunity. Autoimmunity Rev. 2020; 19: 102597.
- Osuchowski MF, Winkler MS, Skirecki T, Cajander S, Shankar-Hari M, et al. The COVID-19 puzzle: deciphering pathophysiology and phenotypes of a new disease entity. Lancet Respir Med. 2021; 9:.622-642.
- Wong H-L, Hu M , Zhou CK, Lloyd PC, Amend KL, et al. Risk of myocarditis and pericarditis after the COVID-19 mRNA vaccination in the USA: a cohort study in claims databases Lancet. 2022; 399: 2191-2199.
- Worku D. Multisystem Inflammatory Syndrome in Adults (MIS-A) and SARS-CoV2: An Evolving Relationship. BioMed. 2023; 3: 195-102.
