
Open Access, Volume 9
Trastuzumab desensitization: A case report
Díaz Codina R1; Tejedor Tejada E2*; Soy Muner D2
1Barcelona University, Spain.
2Barcelona Clinic Hospital, Spain.
Tejedor Tejada E
Barcelona Clinic Hospital, Spain.
Email: edutejedor91@gmail.com
Received : April 24, 2023,
Accepted : June 13, 2023
Published : June 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Desensitisation of patients allergic to cancer drugs is a procedure that is used to allow patients with drug allergies to receive the necessary cancer treatments. This procedure involves the gradual administration of the drug through a series of incremental doses and rates, until the full therapeutic dose is reached [1,2].
The aim of desensitisation is to avoid a life-threatening allergic reaction, which could prevent the use of the drug in question. It is important to emphasise that desensitisation does not cure the allergy itself, but allows the use of the specific drug for the cancer treatment.
It is crucial that this procedure is carried out by personnel trained and experienced in the desensitisation of allergic patients. Monitoring of the patient throughout the process is essential to ensure an adequate response and to detect any monitoring of the patient throughout the process is essential to ensure an adequate response and to detect any allergic reactions should they occur. Although desensitisation is generally safe, there are risks associated with this procedure. For example, a severe allergic reaction may occur at any time during desensitisation, which may require immediate medical intervention. It is important that patients and their families understand these risks and discuss any concerns with their healthcare concerns with their healthcare team [3].
Desensitisation is an important procedure to allow patients with drug allergies to receive the necessary cancer treatments. If performed correctly and under proper medical supervision, it can be a safe and effective option for these patients.
This is particularly relevant in cancer, as the non-use of a drug as a therapeutic line eliminates a treatment option. In the present clinical case, the patient presented an allergy to the drug trastuzumab, which can be considered the gold standard drug in the gold standard drug par excellence in HER-2 positive breast cancer, HER-2 being a membrane tyrosine receptor that is activated by ligands of the EGF (epidermal growth factor) and which, in these cases, is present in the membrane of the tumour cells. Overexpression of HER-2 leads to dysregulation of signalling, which results in uncontrolled growth of tumour cells results in uncontrolled cell growth [4].
In cases where this mutation is affected, targeted treatment with trastuzumab is recommended. Trastuzumab is a recombinant humanised IgG1 monoclonal antibody against the extracellular domain of the HER-2 membrane receptor, thereby inhibiting the growth factor signalling pathway and, therefore, the signalling pathway and consequently inhibits the proliferation of human tumour cells overexpressing HER-2. In addition, trastuzumab is a potent mediator of cell-mediated antibody-dependent cytotoxicity (ADCC); trastuzumab-mediated ADCC is preferentially exerted on HER-2 overexpressing cells.
Keywords: Cancer; Breast; Genetic alterations; Trastuzumab; Desensitisation.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Tejedor Tejada E (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Codina RD, Tejada ET, Muner DS. Trastuzumab desensitization: A case report. Open J Clin Med Case Rep. 2023; 2056.
Introduction
Hypersensitivity reactions to antineoplastic drugs can occur on first exposure or after repeated exposure. This type of adverse effect can be lethal if not managed by specialised personnel. The main families of cancer drugs that cause hypersensitivity include platinum complexes, taxanes, anthracyclines, and monoclonal antibodies. Discontinuation of a drug of these characteristics has a major impact on cancer patients, as they no longer receive a therapeutic line, which are limited in this type of pathology. The desensitisation technique allows the reintroduction of an antineoplastic agent, in this case trastuzumab, after suffering a hypersensitivity reaction. The process consists of administering the drug at increasing doses and infusion rates; during this process, an infusion pump is needed to adjust the times until the desired total dose is reached and to allow the drug to be tolerated. With the desensitisation technique, patients can be administered a drug that would otherwise have to be discarded and therefore, second lines of therapy with more questionable effectiveness would need to be considered. Here we present a clinical case in which collaboration between hospital services was necessary for the development of a standardised working protocol for the desensitisation of a patient to trastuzumab.
Clinical Case Presentation
The following is the case of a 51-year-old female patient, diagnosed at the age of 39 years (2011) of breast cancer, with a size of 2 centimetres. A core biopsy revealed a grade 2 infiltrating ductal carcinoma, with positive estrogen receptor (ER) (75%) and progesterone receptor (PR) (13%); HER-2 was overexpressed (3+).
From the time of diagnosis, she started treatment with epirubicin and cyclophosphamide for 4 cycles and maintenance with tamoxifen (40 mg/day for five years). Cycles and maintenance with tamoxifen (40 mg/day) for five years. After a disease-free interval of 3 years, a mass was palpated in the right breast during a self-examination. After appropriate imaging and ultrasound techniques, a local recurrence of multiple nodules was diagnosed, the measure was 20 x 20 mm. In the pathological anatomy the estrogen receptors are 40%, progesterone receptors are negative, HER-2 receptor expressed and Ki67 index of 40%. At that time she started antineoplastic induction treatment with paclitaxel (80 mg/m2) and trastuzumab (6mg/kg), which will consist of 6 cycles, followed by trastuzumab maintenance every 21 days. After 4 cycles of the 6 cycles of complete treatment, the patient refers to certain discomfort in her hands, such as tingling and difficulty in performing precision tasks. It was therefore decided to treat it as a typical reaction to taxol (neurotoxicity) and it was decided to discontinue treatment. The patient continues with trastuzumab alone until the treatment is completed.
In 2018, with a 4 year old ILE, during a control ultrasound scan, a 5-6 mm lymph node mass was found, suggestive of a probable recurrence at the right axillary level. At that time, the tumour committee considered starting the following line of therapy:Trastuzumab emtansine (TDM-1) in combination with an oestrogen receptor antagonist (fulvestrant).
The patient received treatment without incident for 11 cycles until a progressive increase in bilirubin levels was observed, which made it necessary to discontinue TDM-1. At this point, it was decided that the patient should continue with trastuzumab, to which she had already responded in the past in combination with an oestrogen receptor antagonist (fulvestrant).
The patient restarted trastuzumab treatment without incident until cycle 4, at which time it had to be stopped due to poor tolerance. The patient describes a rash reaction followed by pruritus and flushing of the neck and chest. The event was associated with the infusion of the drug, so the Allergology and Pharmacy Department was contacted to perform an intradermal test to confirm allergy to the drug.
Following the positive prick result, allergy to trastuzumab was confirmed (Figure 1). For this reason, the oncology department requested a trastuzumab desensitisation regimen. This step, the patient is allowed to receive the anti-HER-2 drug as a targeted therapy against the pathology. The allergy service, in agreement with the pharmacotechnical area of the hospital pharmacy, drew up a protocol for desensitisation to trastuzumab, which divides the administration process into 11 steps (Table 1). The process consists of administering the drug in 11 exponential dilutions until the patient’s full dose is completed (384 milligrams). The admixture was prepared as instructed by manufacturer in 0.9% sodium chloride. After aseptic reconstitution with sterile water for preparation for injection, the physical and chemical stability of the reconstituted solution has been demonstrated for 48 hours at 2OC-8OC. Aseptic dilution in bags containing 9 mg/ml (0.9%) sodium chloride solution for injection has demonstrated physical and chemical stability of trastuzumab for up to 30 days at 2OC-8OC and 24 hours at temperatures not exceeding 30OC. In this case, pharmacy service dindn´t prepare the admixture with overfill to accommodate residual volume in intravenous line. The administration tube was provided by the nursing staff. Finally, after the infusion, the IV was flushed with saline to collect any drug that may have been deposited. In addition, a premedication regimen is administered, corticosteroid (methylprednisolone 60 mg) orally in combination with an antihistamine (cetirizine 10 mg) orally. The function of these drugs is to suppress the possible pro-inflammatory activation of the pro-inflammatory activation of immune system cells and to reduce the possible effects of histamine released by mast cells following exposure to the drug. The stipulated protocol consists of infusion in an ascending manner in terms of speed, up to the maximum rate described in the technical data sheet, and doses every 15 minutes, so that after 2 hours and 42 minutes, the patient receives the full dose (figure 2). In this case, the drug was administered according to the described schedule without incident, so the patient was able to resume trastuzumab administration and completed the remaining cycles of the oncological scheme (+13 cycles). Since then, in all the administrations, the speed and dose agreed in this protocol was respected (Table 1).
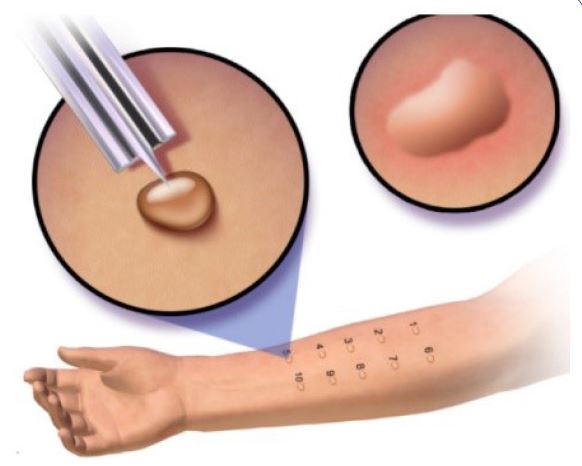
Figure 1: Prick test.

Figure 2: Drug infusion pump.
Table 1: Trastuzumab desensitisation regimen.
| Step | Vel (mL/h) | Time | Vol | Dose | Cumulative dose |
|---|---|---|---|---|---|
| 1 | 0,6 | Oh 15min | 0,2 | 0,21 | 0,21 |
| 2 | 1,2 | Oh 15min | 0,3 | 0,43 | 0,64 |
| 3 | 2,4 | Oh 15min | 0,6 | 0,86 | 1,50 |
| 4 | 4,8 | Oh 15min | 1,2 | 1,72 | 3,22 |
| 5 | 9,6 | Oh 15min | 2,4 | 3,43 | 6,66 |
| 6 | 19,2 | Oh 15min | 4,8 | 6,87 | 13,53 |
| 7 | 38,4 | Oh 15min | 9,6 | 13,74 | 27,27 |
| 8 | 76,8 | Oh 15min | 19,2 | 27,48 | 54,74 |
| 9 | 153,6 | Oh 15min | 38,4 | 54,96 | 109,70 |
| 10 | 307,2 | Oh 15min | 76,8 | 109,92 | 219,62 |
| 11 | 536,6 | Oh 12min | 114,9 | 164,38 | 384,00 |
| TOTAL | 2h 42min | 268,3 |
Discussion
Several publications describing trastuzumab desensitisation protocols can be found in the literature. Trastuzumab desensitisation protocols of 12 steps and 3 bags used for our patient [5-8].
In contrast to these articles, in this case, a standardised working protocol consisting of a single bag of drug was used with good tolerance, as Ramirez and colleagues [9]. Similarly, Lee and colleagues [10], performed desensitisation studies with positive results in patients who were hypersensitive to chemotherapy [9]. In case of the patient described, the hypersensitivity reactions occurred with re-exposure to trastuzumab after a prolonged course of therapy (11 cycles), with good tolerability, as occurred in the studies by Melamed, De Lira-Quezada et al., in which they presented a protocol supported by a similar magnitude. Our experience has allowed us to demonstrate the safety of using an optimised desensitisation protocol for the patient and nursing staff [11-13]. The eleven-step process was well tolerated and the patient was able to continue with her standard HER-2 breast cancer treatment. It is necessary to remember the continued risk of anaphylaxis for patients with any drug sensitisation, in this case trastuzumab will require desensitisation every time it is administered for the rest of her life.
References
- Barreiro-Fernández E.M, Gil-Sierra MD, Briceño-Casado M, Martínez-Díaz C, Ríos-Sánchez E. Inclusión de omalizumab en un protocolo de desensibilización de trastuzumab. Farm Hosp. 2022; 46.
- López-de-Torre Querejazu A, Ibarra Barrueta O, Santos Ibañez A, Mayo Suárez. Desensibilización a enfuvirtide: a propósito de un caso fallido. J. Farm Hosp. Abril. 2012; 36: 112-113.
- Ibrahim Y, Bin Naji S, Mobayed H, Al-Nesf M. Contributions of nurse specialists in the allergy and immunology service and patient care. Qatar Med J. 2022; 2022: 7.
- Harbeck N, Gnant M. Breast cancer. Lancet. 2017; 389: 1134-1150.
- Maximiano S, Magalhães P, Guerreiro MP, Morgado M. Trastuzumab in the Treatment of Breast Cancer. BioDrugs. 2016; 30: 75-86.
- Lee CW, Matulonis UA, Castells MC. Rapid inpatient/outpatient desensitization for chemotherapy hypersensitivity: Standard protocol effective in 57 patients for 255 courses. Gynecol Oncol. 2005; 99: 393-399.
- Brennan PJ, Rodriguez Bouza T, Hsu FI, Sloane DE, Castells MC. Hypersensitivity reactions to mAbs: 105 desensitizations in 23 patients, from evaluation to treatment. J Allergy Clin Immunol. 2009; 124: 1259-1266.
- Bavbek S, Kendirlinan R, Çerçi P, et al. Desensibilización rápida a fármacos con productos biológicos: una experiencia de un solo centro con cuatro productos biológicos. Int Arch Allergy Immunol. 2016; 171: 227-233
- Ramírez-Cruz S, Lucena-Campillo MA, Vila-Albelda C, Garrido-Arévalo M, De Agustín-Sierra L, et al. Desensitization protocol to nivolumab without corticosteroid use in a kidney cancer patient. Farm Hosp. 2020; 44: 182-183.
- Lee CW, Matulonis UA, Castells MC. Desensibilización rápida para pacientes hospitalizados/ambulatorios por hipersensibilidad a la quimioterapia: protocolo estándar efectivo en 57 pacientes durante 255 ciclos. Gynecol Oncolo. 2005; 99: 393-399.
- Lira-Quezada de C. Protocol for Desensitization to Trastuzumab in a Patient With Anaphylaxis and Stage IV Breast Cancer: A Case Report. J Investig Allergol Clin Immunol.
- de Lira-Quezada CE, Villarreal-González RV, González-Díaz SN, Acuña-Ortega N. Protocol for Desensitization to Trastuzumab in a Patient With Anaphylaxis and Stage IV Breast Cancer: A Case Report. J Investig Allergol Clin Immunol. 2020; 30: 376-377.
- Melamed J, Stahlman JE. Rapid desensitization and rush immunotherapy to trastuzumab (Herceptin) [3]. Journal of Allergy and Clinical Immunology. 2002; 110: 813-814.
