
Open Access, Volume 9
A family educational therapy for a 15 months-old child with polydipsia
Cipriano Paola1*; Fornasier Matteo2; De Marco Francesca2; Camilla Gizzi1
1Paediatric Department, Sandro Pertini Hospital, Rome, Italy
2Paediatric Medical Specialty School, Sapienza University, Rome; Italy.
Cipriano Paola
Paediatric Department, Sandro Pertini Hospital, Rome, Italy.
Email: paola.cipriano@aslroma2.it
Received : April 20, 2023,
Accepted : June 07, 2023
Published : June 09, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Polydipsia is a condition characterized by excessive water intake and can be caused by several conditions. We present a case report of a child who was admitted in our department for persistent fever, but during the recovery a primary polydipsia was accidentally found through laboratory exams.
Keywords: Dipsogenic polydipsia; Hyponatremia; Polyuria.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Paola C (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Paola C, Matteo F, Francesca DM, Gizzi C. A family educational therapy for a 15 months-old child with polydipsia. Open J Clin Med Case Rep. 2023; 2053.
Introduction
Polydipsia is a condition characterized by excessive water intake, often associated with various degrees of hypoosmolality and hyponatremia, and a suppression of ADH (Anti-Diuretic Hormone) production that causes polyuria. These features can be found either in secondary polydipsia, for instance in patients with diabetes insipidus (DI), or in primary polydipsia. Primary polydipsia can be divided in psychogenic polydipsia, which affects patients with psychiatric disorders, and dipsogenic polydipsia, in which people have some hypothalamic dysfunction or voluntarily drink big amounts of water to achieve a healthier status [1]. If the water intake is very high and occurs in a short period of time, the kidney is not able to compensate the hypervolemia, and so acute hypoosmolality and hyponatremia occur, leading to acute cell swelling, including brain oedema. Brain cells have some protective mechanisms that prevent oedema, like active electrolytes pumping from the ICS (intra-cellular space) to ECS (extra-cellular space), but when all the compensation mechanisms are not sufficient and cerebral oedema occur, since the swelling is limited by the skull, brain herniation can be a life-threatening condition. Correction of acute hyponatremia must be very careful, since a fast sodium and fluid administration can lead to Central Pontine Myelinolysis (CPM), which is fortunately very rare in paediatric patients [2].
Case Presentation
We admitted in our paediatric first aid department a 15 months-old child, due to persistent fever unresponsive to therapy. According to our suspects and the findings at the physical examination, we performed a thorax radiography, a complete blood count with serum electrolytes and a urine analysis. The thorax radiography revealed a slight peribroncovascular thickening, the complete blood count showed a microcytic hypochromic anaemia, and serum electrolytes were normal apart from Na+ (127 mEq/L, normal values 135-145 mEq/L). The urine had a low specific weight (1009 g/L, normal values 1014-1025 g/L). Another urine sample collected few days before, in occasion of a previous access to our first aid department due similar clinical conditions, had a 1000 g/L specific weight. We then decided to hospitalize the patient in our paediatric department. Collecting anamnestic data, parents reported that the father and the grandmother have favism and that the mother has Hashimoto’s thyroiditis. Pregnancy and first months of life were uneventful, and the baby was fed with artificial milk only. When she was 10 months old, she started to refuse milk, which was then definitely removed from her diet, but from that moment on they also reported that she started to be often nervous and that they observed a drop in her growth (which had not been quantified). On that purpose, they reported that she often didn’t feel like eating for most of the day in the last months, while she felt like drinking water often, especially in the night, with an average night water intake reported of 1500 mL. Indeed, they had to change from 4 to 7 diapers during night-time. Yet, the mother reported that this condition, which was apparently normal to her and to the husband, was not seen during the day in the moments in which the daughter was not with the parents, for instance while she was playing with other children away from home. On the 2nd and the 3rd day of recovery Na+ serum levels were still below 130 mEq/L, so a kidney and bladder US was performed, revealing a poor corticomedullary differentiation, and diffuse parenchymal hypoechogenicity. We calculated the water balance during the following 24 hours, and the values reported by the nurses were 2260 mL of water intake, and a urine output of 2485 mL, defining a polyuria-polydipsia condition. To exclude other causes of polyuria we checked calcium and glucose levels, that were normal. No head traumas were reported and neither any other sign or symptom of hypothalamic disease. Even though polydipsia was reported only in home context, which led us to think about a behavioural problem, we had to exclude secondary polydipsia due to Diabetes Insipidus (DI). We performed a restriction of water intake, to make a differential diagnosis between primary and secondary polydipsia. We diminished increasingly the water intake during the day to 1000 ml along the 24 hours, and we reported blood sodium levels and urine parameters returning to almost normal values (Na+ 141 mEq/L, 1005 g/L urine specific weight). We explained to the parents how to manage the water intake during the day, and once the laboratory exams turned back to normal values, we discharged the patient. After the discharge, the baby was followed up in our endocrinology ambulatory. At the first visit we evaluated the growth pattern of the child according to the WHO Child Growth Standards. We could observe a strong decrease in the growth after milk feeding was stopped and the abnormal water intake was started, at the age of 12 months (Figure 1). In the following month the kidney US was repeated, and corticomedullary differentiation was normal, with no hypoechogenicity. The parents observed a return to normal hunger, an increased growth (Figure 1), and no more irritable mood during the day.
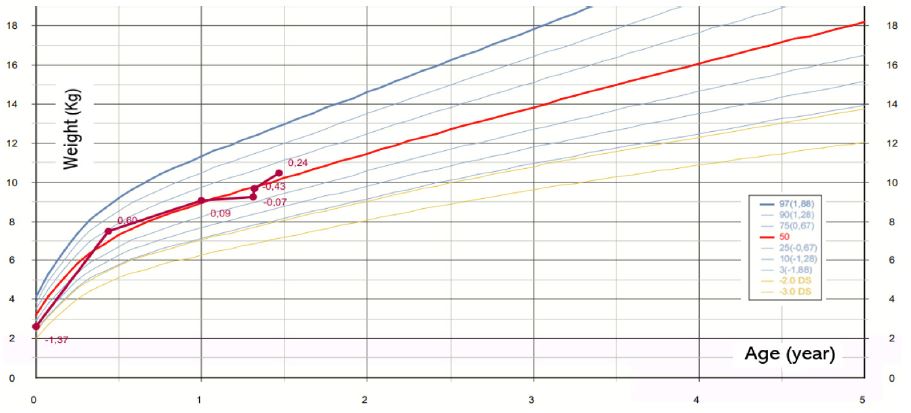
Figure 1: WHO growth chart for weight before and after educational therapy.
Discussion
According to the differences in the values of serum Na+ levels and urine specific weight we found before and after the educational therapy carried out during the days of recovery, a dipsogenic primary polydipsia diagnosis could be make, a condition in which Na+ levels return in 3-6 hours to normal values after water intake restriction [2]. The habit of the parents of maintain a daily water intake higher than 2L, probably meant to reach a healthier status, was transmitted to the child, who gained the same habit, asking by herself big amounts of water, especially during the night. Such a water intake is twice the value suggested by the EFSA guidelines for a child between 12 and 24 months of age (1100-1200 daily total water intake) [3]. We spent some more time collecting anamnestic data to exclude a Munchausen syndrome by proxy, a condition in which one of the parents creates voluntarily a pathological condition in the child to seek medical attention and receive in turn attention to him/herself and appear as a good mother/father. This option was not consistent with the reason of the hospitalization (which was an upper respiratory tract infection) and with the real lack of awareness of the parents about the abnormality of such a water intake. The lack of hunger and consequently the drop in the growth from insufficient food intake could be explained with a persistent gastric distension that led the child to feel less hunger. Irritable mood was probably due to several reasons, including poor sleep quality due to repeated interruptions for diapers change, insufficient food intake, psychological pressure from parents.
Conclusion
The collection of anamnestic data and the observation of the child's habits during hospitalization made it possible to undertake an educational program that was well accepted by the family.
References
- Kotagiri R, Kutti Sridharan G. Primary Polydipsia. 2022.
- Kliegman R, Geme J. Nelson textbook of paediatrics. 2019.
- Gandy J. Water intake: validity of population assessment and recommendations. Vol. 54, European Journal of Nutrition. Dr. Dietrich Steinkopff Verlag GmbH and Co. KG; 2015; 11-16.
