
Open Access, Volume 9
Inoperable and treatment-resistant hypopharyngeal carcinoma carrying an NTRK gene translocation in a young adult female patient with fanconi anemia: A case report
Almudena García-Castaño1*; Belen Caramelo Hernández1,3; Laura Sánchez Togneri1; Mireia Menéndez Cava1; Patricia García Valiente1; Marta Sotelo García1; Marina Serrano Fernández1; Javier Freire Salinas4; Elena Marín-Díez5
1Medical Oncology Department, University Hospital Marqués de Valdecilla, Santander, Spain.
2Medical Oncology Department, Sierrallana Hospital, Torrelavega, Spain.
3IDIVAL- Valdecilla Health Research Institute, Santander, Spain.
4Pathological Anatomy Department, University Hospital Marqués de Valdecilla, Santander, Spain.
5Department of Radiology, Hospital Universitario Marqués de Valdecilla, Santander, Spain.
García-Castaño A
Medical Oncology Department, University Hospital Marqués de Valdecilla, 25 Avenida de Valdecilla, Santander 39008, Spain.
Email: almudena.garcia@scsalud.es
Received : April 13, 2023,
Accepted : May 29, 2023
Published : May 31, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Congenital Fanconi Anemia (FA) increases susceptibility to cancer and its treatment side effects. Here, a 38-year-old female patient presented with signs of bone marrow failure, previously undiagnosed FA and an NTRK-gene fusion-positive tumor in the hypopharynx that was inoperable. Given the early tumor relapse and poor tolerability of conventional therapy in this patient, she initiated treatment with larotrectinib. Complete tumor response was achieved after seven months of treatment and maintained throughout the 19-month follow-up period without serious adverse events. FA should be suspected in these clinical scenarios, and targeted therapy may be the best practice approach.
Keywords: Fanconi anemia; Head and neck neoplasms; Carcinoma; Squamous cell; NTRK-gene fusion; Larotrectinib.
Abbreviations CT: Computed tomography; ECOG: Eastern Cooperative Oncology Group; EMA: European Medicines Agency; ENT: Ear, nose and throat; FA: Fanconi anemia; FDA: Food and Drug Administration; HELLP: Hemolysis, elevated liver enzymes and low platelets; HPV: Human papillomavirus; IHC: Immunohistochemistry; MRI: Magnetic resonance imaging; NTRK1: Neurotrophic Tyrosine Receptor Kinase; PET: Positron emission tomography; SCC: Squamous cell carcinoma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © García-Castaño A (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: García-Castaño A, Hernández BC, Togneri LS, Cava MM, Valiente PG, Garcia MS, Fernandez MS, et al. Inoperable and treatment-resistant hypopharyngeal carcinoma carrying an NTRK gene translocation in a young adult female patient with fanconi anemia: A case report. Open J Clin Med Case Rep. 2023; 2049.
Introduction
Fanconi anemia (FA) is a rare genetic recessive disease with an incidence of approximately 1/300,000 live births [1]. It is characterized by congenital malformations in multiple organs and bone marrow failure, which causes progressive pancytopenia, often initially with thrombocytopenia or leukopenia preceding anemia. Moreover, FA predisposes to leukemia and solid tumors [2,3]. Despite these general features, clinical manifestations of FA may vary from patient to patient. Moreover, some phenotypic manifestations may be absent in up to 20-30% of the cases, thereby challenging the early diagnosis and management of FA and subsequent associated complications. In fact, diagnosis is often delayed until young adulthood [3,4].
Here, we report a life-threatening head and neck carcinoma in a young adult patient with FA showing inadequate response to chemotherapy and radiotherapy and poor tolerability profile.
Case Presentation
A 38-year-old woman and former smoker (8 pack-years) presented with a history of ectopic left kidney, hypertransaminasemia of cholestatic etiology (mainly) with no alterations in liver biopsies (May 2017) and premature ovarian failure since 2011. She was positive for high-risk Human Papillomavirus (HPV) (HPV 56, 51, 54, 66, 81 and 84) and was subject to conization in April 2014. Partial Hemolysis, Elevated Liver Enzymes and Low Platelets (HELLP) syndrome, severe preeclampsia and pancytopenia occurred during pregnancy with donor egg. The bone marrow biopsy confirmed medullary hypoplasia with no cytogenetic alterations (July 2018).
In March 2019, she was initially diagnosed with acute otitis and was administered oral anti-inflammatory and antibiotic treatment for her right otalgia, with no improvement after a few weeks. Computed Tomography (CT) scan of the cervical spine showed a lesion in the mucosa of the right pyriform sinus with ipsilateral adenopathy of 3.1 cm and no signs of distant spreading (Figure 1A). The nasofribroscopy revealed a non-ulcerated vegetative neoformation in the right pyriform sinus, and the subsequent biopsy showed a well-differentiated infiltrating Squamous Cell Carcinoma (SCC).
We suspected congenital FA given the presence of a hypopharyngeal tumor in a young patient with previous cytopenia, medullar hypoplasia and no significant toxic habits. Later, the diagnosis was confirmed by diepoxybutane-induced chromosome fragility test.
Following the multidisciplinary team meeting, the patient was not eligible for organ-preserving surgery. Therefore, anti-cancer therapy was initiated in June 2019 with concurrent radiotherapy and cetuximab to prevent the high toxicity of alkylating agents in patients with AF. Afterwards, she was hospitalized for the treatment of grade 2 dermatitis, grade 3 mucositis that interfered with oral intake, grade 4 thrombocytopenia and esophageal candidiasis with candidemia. The patient received parenteral feeding and intravenous anti-fungal medication, which improved her clinical condition. However, cetuximab was suspended after the fifth cycle to avoid further toxicity. By the end of radiotherapy in July 2019, she had received 70 Gy in the retropharyngeal region, larynx, hypopharynx and bilateral areas II, III and IV. Eight weeks after the treatment, the CT scan and Magnetic Resonance Imaging (MRI) showed complete radiological response (Figure 1B). Cervical adenopathy was no longer palpable and endoscopic exploration confirmed the absence of any neoformation.
In October 2019, the patient started noticing a hard and painful submandibular mass of approximately 1 cm in diameter that had regrown on the right side of the hypopharynx. The Positron Emission Tomography (PET) scan and needle biopsy confirmed the diagnosis of SCC of the head and neck region (Figure 2). Considering the disease persistence and absence of distant tumor metastasis by imaging techniques, we performed rescue surgery on the right cervical region. During the procedure, we found that the primary tumor had spread to one of the 14 removed lymph nodes, invading the extracapsular, vascular and perineural regions and surgical margins. Despite these risk factors, the patient did not receive any adjuvant treatments due to the previous toxic effects and cumulative radiation dose.
In January 2020, after a follow-up, the patient presented with an Eastern Cooperative Oncology Group (ECOG) score of 1 and dysphagia with frequent choking when eating or drinking that seriously compromised her nutritional status. After multidisciplinary team discussion, the patient was not considered eligible for surgical or re-irradiation therapy since the right-sided parapharyngeal area affected by adenopathy had already surrounded the carotid artery (Figure 3A).
While considering other treatments, we sequenced a panel of 160 genes by next generation sequencing techniques. We could detect the presence of Neurotrophic Tyrosine Receptor Kinase (NTRK1) oncogenic fusion and then, NTRK1 gene overexpression was confirmed by immunohistochemistry (IHC) (Figure 4). Then, in March 2020, she obtained expanded access to larotrectinib, taken as 100 mg every 12 hours. After the first 28-day cycle, we observed objective response with complete disappearance of the cervical cutaneous node, gradual improvement of dysphagia and secondary weight gain. In the first reassessment (June 2020), we only reported a hyper capturing nodular thickening at the distal portal of the sternocleidomastoid muscle. In the second one (October 2020), the CT scan results showed complete objective response to larotrectinib (Figure 3B).
Regarding side effects, grade I myalgias improved with anti-inflammatory medication. In addition, the treatment was delayed twice due to afebrile G3 neutropenia, which may have been related to the underlying bone marrow failure. In the last control visit (October 2021), the patient maintained complete treatment response, ECOG score of 0 and normal lifestyle.
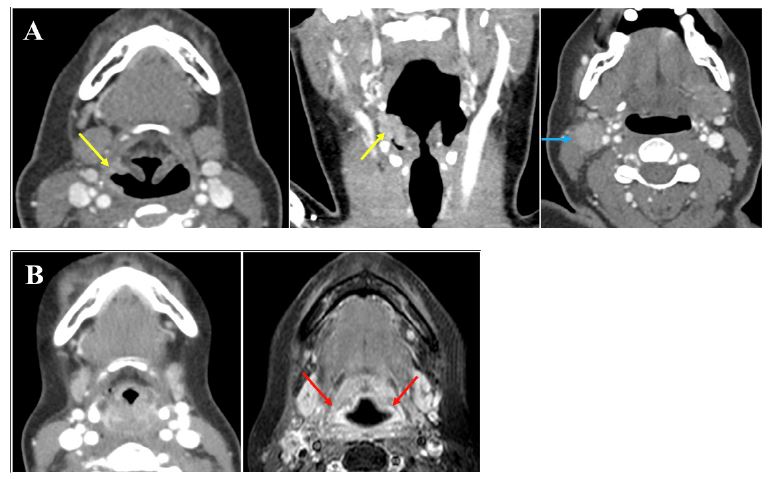
Figure 1: (A) CT scan with contrast of the cervical spine at diagnosis. A hyperintense vegetative lesion in the right pyriform sinus (yellow arrows) can be observed in the axial (left panel) and coronal (middle panel) sections. The level III axial section (right panel) depicts adenopathy in the right cervical region (blue arrow). (B) CT scan and MRI with contrast eight weeks after completion of chemotherapy and radiotherapy. CT scan in axial section (left panel) shows significant inflammatory changes in the mucosa of the hypopharynx and occlusion of both pyriform sinuses. Fat saturated T1 post-contrast sequence MRI in axial section (right panel) shows no findings suspicious for malignancy (red arrows). CT, computed tomography; MRI, magnetic resonance imaging.
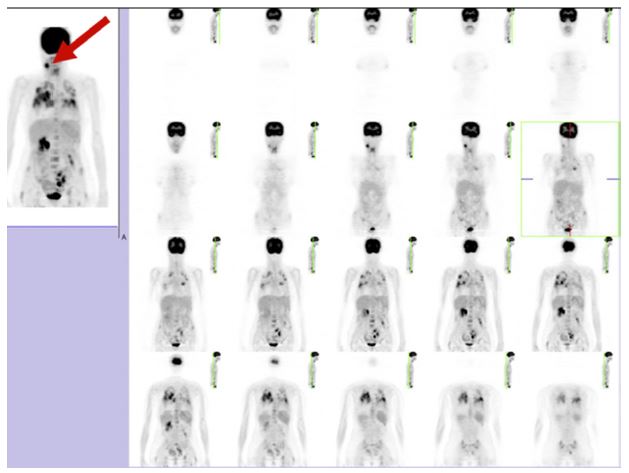
Figure 2: PET scan confirming right laterocervical and hyperintense adenopathy in the patient after tumor relapse. PET, positron emission tomography.
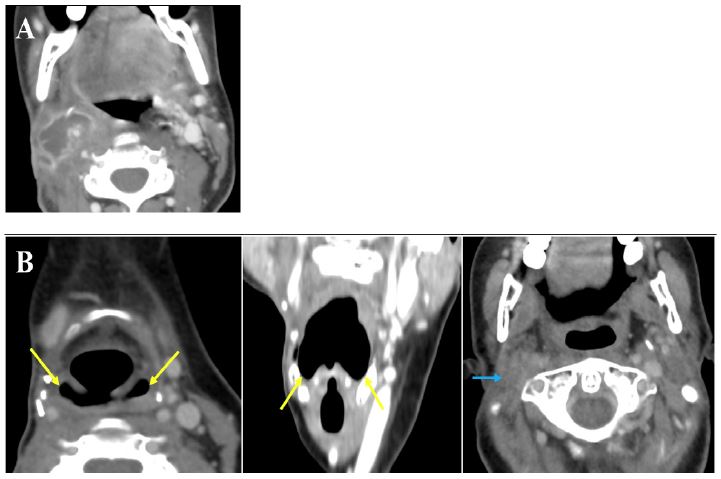
Figure 3: (A) Level IIA/III CT scan with contrast of the cervical spine confirming locoregional tumor relapse. (B) CT scan with contrast after seven months of treatment with larotrectinib. Axial (left panel) and coronal (middle panel) sections show the absence of any asymmetries and suspicious contrast-enhanced areas in the hypopharynx (yellow arrows). Axial section (right panel) depicts structural changes due to previous rescue surgery, but no signs of tumor relapse can be detected (blue arrow). CT scan, computed tomography scan.
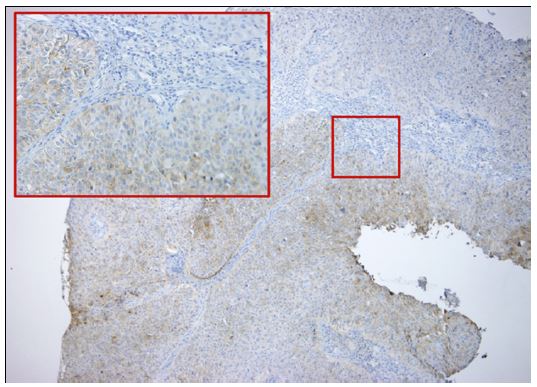
Figure 4: TRK IHC detecting NTRK gene fusion. 10x and 40x original magnification. IHC, immunohistochemistry; NTRK,neurotrophic TRK; TRK, tropomyosin receptor kinase.
Discussion
We present a patient with previously undiagnosed FA, unresectable head and neck carcinoma and early tumor relapse who was successfully treated with larotrectinib, thereby radically improving the patient’s prognosis.
Patients with FA are at an increased risk of esophageal and anogenital tumors. Specifically, there is a 500/700-fold increased risk for head and neck cancer compared with the general population [5]. For this reason, a thorough Ear, Nose and Throat (ENT) examination for tumors is recommended every six months for patients with FA aged ten and older. HPV vaccination is also recommended as emerging evidence points towards a possible contribution of this viral infection to the development of head and neck SCC [6].
FA is often diagnosed upon detecting these rare tumors in young patients or by the excessive toxicity after chemotherapy or radiotherapy. In our case, previous ectopic kidney, premature ovarian failure and cytopenias could not be explained individually, but we strongly suspected that FA was the underlying pathological condition in light of the later oncologic findings. Furthermore, we could also observe the increased susceptibility of our patient to anti-cancer treatment side-effects, persistent mixed (central and drug-induced) thrombocytopenia and infectious diseases (candidemia) that are common among immunocompromised patients.
Given the early tumor relapse after the initial treatment and in the absence of any other conventional therapeutic options for our patient, we decided to use a tumor-agnostic approach based on the NTRK fusion-positive test results. NTRK1, NTRK2 and NTRK3 genes encode TRKA, TRKB and TRKC kinases, respectively, which are involved in several signaling pathways that regulate cell proliferation and differentiation. When present, the NTRK gene fusion leads to constitutive kinase activity and, consequently, uncontrolled cellular proliferation and tumor growth [7]. Up to 1% of all primary tumors harbor this oncogenic aberration, mainly rare adult tumors such as secretory breast cancer and secretory carcinoma of salivary gland, as well as pediatric tumors including infantile fibrosarcoma and cellular congenital mesoblastic nephroma [8]. In head and neck SCC, the identification of PAN3-NTRK2 fusion was identified by Stransky and collaborators, inviting the use of TRK inhibitors in these tumors [9].
The TRK inhibitor larotrectinib was approved by the U.S. Food and Drug Administration (FDA) in 2018 and, one year later, by the European Medicines Agency (EMA) to treat adult and pediatric patients with NTRK fusion-positive solid tumors that are metastatic, unresectable or in the absence of satisfactory therapeutic alternatives [10,11]. The three pivotal trials (Phase 1 study [NCT02122913], SCOUT [NCT02637687] and NAVIGATE [NCT02576431]) demonstrated the efficacy of larotrectinib in a heterogenic population of adult and pediatric patients with NTRK fusion-positive solid tumors, with an overall response rate of 75% and 80% according to independent review and investigator assessments, respectively [12]. More recently, a combined and updated analysis of 159 patients from these trials obtained a median duration of response of 35.2 months and a median progression-free and overall survival rates of 28.3 and 44.4 months, respectively. Here, the objective response rate by investigator was 79%, regardless of tumor type and patient age, with 16% of patients having complete responses [13]. In line with these results, tumor genotyping of our patient allowed the application of a molecularly targeted therapy with larotrectinib, which resulted in rapid objective response within three months and complete tumor remission after seven months of treatment.
Conclusion
In conclusion, FA should be suspected in young patients diagnosed with ENT tumors and no related toxic habits, especially in the presence of persistent cytopenia due to medullar hypoplasia. Moreover, early patient genotyping may allow innovative and efficacious treatments based on NTRK-gene rearrangements.
Declarations
Acknowledgements: The authors thank Bayer for providing larotrectinib through their Expanded Access Program and Neus Cantariño (Trialance SCCL, Spain) for her medical writing support.
Authorship contribution statement: AGC: Conceptualization (lead); methodology (lead); formal analysis (lead); writing – original draft (lead); review and editing (equal). BCH: Conceptualization (equal); writing – original draft (equal); review and editing (supporting). MMC: Conceptualization (equal); writing – original draft (equal); review and editing (equal). LST, PGV, MSG, MSF, JFS and EM-D: review and editing (equal). All authors read and approved the submitted version of the manuscript.
Author Disclosure Statement: No competing financial interests exist.
Funding: Medical writing assistance was funded by Bayer Spain. No other sources of funding were received for the work.
References
- Orphanet. The portal for rare diseases and orphan drugs. Fanconi anemia. 2020.
- Nepal M, Che R, Zhang J, Ma C, Fei P. Fanconi Anemia Signaling and Cancer. Trends in cancer. 2017; 3: 840-856.
- Fiesco-Roa MO, Giri N, McReynolds LJ, Best AF, Alter BP. Genotype-phenotype associations in Fanconi anemia: A literature review. Blood Rev. 2019; 37: 100589.
- Mehta PA, Ebens C. Fanconi Anemia. In: Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJ, Gripp KW, et al., editors. GeneReviews. Seattle (WA): University of Washington, Seattle; 2021; 1-391.
- Kutler DI, Wreesmann VB, Goberdhan A, Ben-Porat L, Satagopan J, et al. Human papillomavirus DNA and p53 polymorphisms in squamous cell carcinomas from Fanconi anemia patients. J Natl Cancer Inst. 2003; 95: 1718-1721.
- Fanconi Anemia Research Fund. Fanconi Anemia Clinical Care Guidelines. 5th Edition 2020. 2020.
- Berger S, Martens UM, Bochum S. Larotrectinib (LOXO-101). In: Recent results in cancer research Fortschritte der Krebsforschung Progres dans les recherches sur le cancer. Recent Results Cancer Res. 2018; 141-151.
- Filippi R, Depetris I, Satolli MA. Evaluating larotrectinib for the treatment of advanced solid tumors harboring an NTRK gene fusion. Expert Opin Pharmacother. 2021; 22: 677-684.
- Stransky N, Cerami E, Schalm S, Kim JL, Lengauer C. The landscape of kinase fusions in cancer. Nat Commun. 2014; 5: 4846.
- European Medicines Agency (EMA). Vitrakvi. 2019.
- U.S. Food and Drug Administration (FDA). VITRAKVI-Accelerated Approval (COR-NDAACTION-04). 2018.
- Drilon A, Laetsch TW, Kummar S, DuBois SG, Lassen UN, et al. Efficacy of Larotrectinib in TRK Fusion–Positive Cancers in Adults and Children. N Engl J Med. 2018; 378: 731-739.
- Hong DS, DuBois SG, Kummar S, Farago AF, Albert CM, et al. Larotrectinib in patients with TRK fusion-positive solid tumours: a pooled analysis of three phase 1/2 clinical trials. Lancet Oncol. 2020; 21: 531-540.
