
Open Access, Volume 9
Valsalva induced traumatic epiglottitis
Samantha Cox; Peter J Kumasaka; Keith Henry*; Bradley Hernandez
Emergency Medicine, Health Partners Institute for Medical Education, Regions Hospital – St Paul, Minnesota, USA.
Keith Henry
Emergency Medicine Residency, Health Partners Institute for Medical Education, Regions Hospital – St Paul, Minnesota, USA.
Email: kdhenrymd@comcast.net
Received : April 11, 2023,
Accepted : May 23, 2023
Published : May 31, 2023,
Archived : www.jclinmedcasereports.com
Keywords: Case; Breathing; Acute trauma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Henry K (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Cox S, Kumasaka PJ, Henry K, Hernandez B. Valsalva induced traumatic epiglottitis. Open J Clin Med Case Rep. 2023; 2045.
Case Presentation
A 50 year old previously healthy female, with no significant past medical history, was evaluated outside urgent care facility after sustaining a fall on outstretched left upper extremity. She was wearing a helmet at the time and sustained no head, neck, or torso injury. She noted immediate pain to her left wrist and proceeded promptly to urgent care for assessment. While driving to urgent care, she developed a gradual onset sore throat proceeding to a hoarse and muffled voice. At time of initial contact at Urgent Care, her work of breathing remained unlabored and no stridor was appreciated; she was, however tender to palpation over the anterior neck but without external evidence of acute trauma. In addition to obtaining plain film imaging of her left wrist, a contrast CT imaging study of the neck was obtained to evaluate for occult injury. Figure 1 indicates a significantly enlarged epiglottis to suggest acute inflammation vs injury to the epiglottis. Figure 2 represents an axial reconstruction of the same soft tissue neck CT; it lacks any evidence of acute blunt trauma to the anterior or pre-vertebral soft tissues of the neck.
The patient was transferred by ambulance from Urgent Care to a Tertiary Care, Level 1 trauma center within a short distance. Her vitals remained stable and work of breathing unlabored during transport and at time of arrival to her destination Hospital. No stridor was appreciated. Her abnormal imaging studies were reviewed. The abnormal epiglottis was further evaluated by flexible fiberoptic epiglottoscopy through a nasal approach seen below in figure 3.
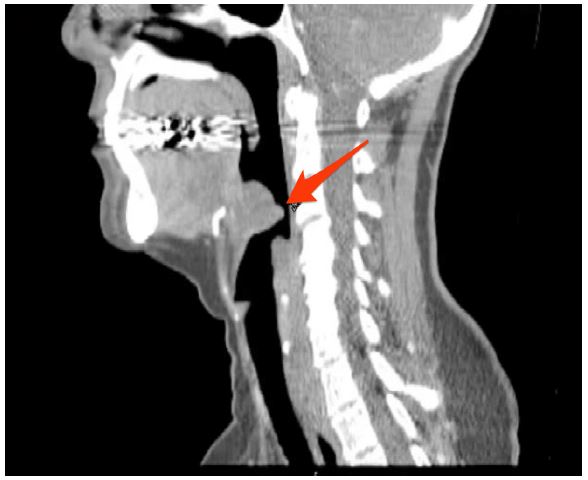
Figure 1: A soft tissue CT imaging study of the Neck. Red Arrow Denoting a significantly enlarged Epiglottis measuring 2-3 times the normal size.
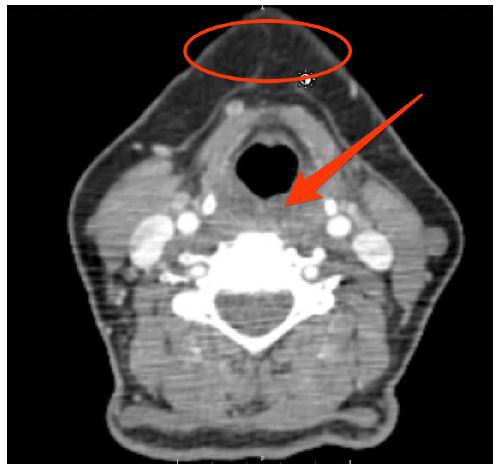
Figure 2: An axial oriented CT imaging study of the soft tissues of the neck. The red circle indicates lack of stranding or injury to the anterior neck soft tissues. The red arrow denotes any prevertebral soft tissue swelling to further suggest against traumatic blunt trauma to the anterior neck.
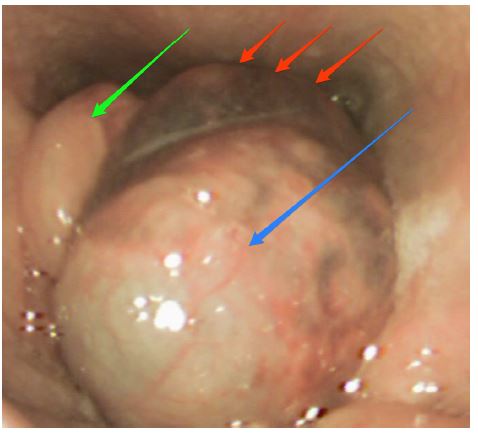
Figure 3: Blue arrow indicates a markedly swollen epiglottis. Red arrows indicate fresh hematoma contained within the soft tissues of the cord facing side of the epiglottis. Green arrow indicates swollen arytenoid cartilage.
The patient was monitored closely in the Emergency Department. A previously identified left distal radial fracture was anesthetized, reduced, and splinted. The patient was admitted to the Trauma Surgery Service for close monitoring and observation of her presumed airway injury. Ultimately this patient received 24 hours of steroids and had an uneventful two-night observation period in the hospital. Repeat scope the day following the initial injury demonstrated improved epiglottic mobility but persistent swelling. She required no acute airway intervention overnight and was discharged home in stable condition. Outpatient follow-up 8 days later demonstrated significant subjective and objective improvement with only mild edema in the arytenoids and anterior epiglottis with no plan for additional follow-up.
Discussion
There are scant published cases of non-traumatic - presumably Valsalva-induced - airway injury which have resulted in thyroid cartilage fractures and vocal cord hematomas after sneezing or coughing [1]. To our knowledge, there has not been a single published case of Valsalva-induced epiglottic injury as demonstrated in the present case. Conservative management including vocal rest, steroids, and close short-term monitoring were universally successful in these cases and in ours. Literature discussing traumatic epiglottitis is limited almost exclusively to direct trauma to the anterior neck or peri-procedurally to the epiglottis itself.
References
- Reuther MS, Weissbrod PA. Voice Change, Odynophagia, and Neck Pain Following a Sneeze. JAMA Otolaryngol Head Neck Surg. 2017; 143: 89-90.
- Shah Rahul K, Stocks Carol. “Epiglottitis in the United States: national trends, variances, prognosis, and management”. The Laryngoscope. 2010; 120: 1256-1262.
