
Open Access, Volume 9
Perforated liver abscess: A case report
Alharmoodi F1; Alkhyeli F2; Almadhaani S2; Ghabra S3; Buali O1; Alharthi S4
1Department of general surgery, Tawam Hospital-Alain, UAE.
2College of medicine and health sciences, United Arab Emirates University, UAE.
3Department of general surgery, Medstar Georgetown University Hospital, Washington D.C., USA.
4Department of general surgery Sheikh Shakhbout Medical City (SSMC) Abu Dhabi, UAE.
Alharmoodi F
Department of general surgery, Tawam Hospital-Alain-UAE.
Email: harmoodi.f@gmail.com
Received : April 06, 2023,
Accepted : May 15, 2023
Published : May 16, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Liver abscesses are the most common abscesses in the abdomen with pyogenic form being the most common in liver abscess. Gas forming bacteria in the liver are rare, and it increases morbidity and mortality if it occurs. Management of gas forming abscess can be challenging and multimodal treatment might be needed, in this case report we present a middle-aged male who was admitted under the impression of a perforated viscus but was found to have a perforated liver abscess that was treated accordingly.
Keywords: Gas-forming pyogenic liver abscess; Rupture; Pneumoperitoneum.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Alharmoodi F (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Alharmoodi F, Alkhyeli F, Almadhaani S, Ghabra S, Buali O, et al. Perforated liver abscess: A case report. Open J Clin Med Case Rep. 2023; 2039.
Introduction
Pyogenic liver abscess is the most common type of visceral abscess, with an incidence of 2.3 cases per 100,000 [1]. Pyogenic liver abscess (PLA) can be classified by size, etiology microorganism, and gas formation. Gas-Forming Pyogenic Liver Abscess (GFPLA) is a rare subgroup of PLA, defined as the presence of gas within the abscess, which was first recognized in 1944 by Smith [2]. There are only a few reported cases with distinct emphasis on GFPLA separately. Hence, the understanding of it remains limited. GFPLA is associated with diabetes mellitus and monomicrobial causative etiology like Klebsiella pneumoniae. It carries a significantly higher mortality (30.3%) rate compared to non-GFPLA (9%) [3].
Case Report
A 55 year old male with hypertension and type 2 diabetes presented to the emergency department due to 4 days of worsening abdominal pain, fever associated with night sweats, and difficulty breathing. He described his pain to be epigastric, radiation to his left upper quadrant which has been progressively worsening in severity. He was nauseated but had no episodes of vomiting or changes in bowel habits. Fever was subjective and associated with night sweats. Over the past 2 days, his urine was darker. He also reported decreased appetite, distention of his abdomen and yellowing of the skin. He had no sick contacts and he last traveled 3 years ago, to the Philippines, he was living an urban area. He is a non-smoker and occasionally drinks alcohol. On clinical assessment, he was borderline hypotensive (95/55), afebrile, tachycardiac, with normal respiratory effort and oxygen saturation. He was alert, oriented, but appeared to be distressed. He had jaundice and scleral icterus. Abdominal examination showed evidence of abdominal distention and right upper quadrant tenderness. Otherwise, abdomen was soft with no rebound or rigidity. Murphy’s sign negative. Liver enzymes were elevated including total and direct bilirubin of more than 200 micromol/L, he had kidney injury, leukocytosis. This was his first presentation to our hospital and no previous labs were there to compare.
Initially the ER physician suspected it might be covid infection, hence CT and covid PCR was ordered for him. The test was negative for covid, and CT chest didn’t reveal chest infection, nevertheless, it showed air under diaphragm (Figure 1).
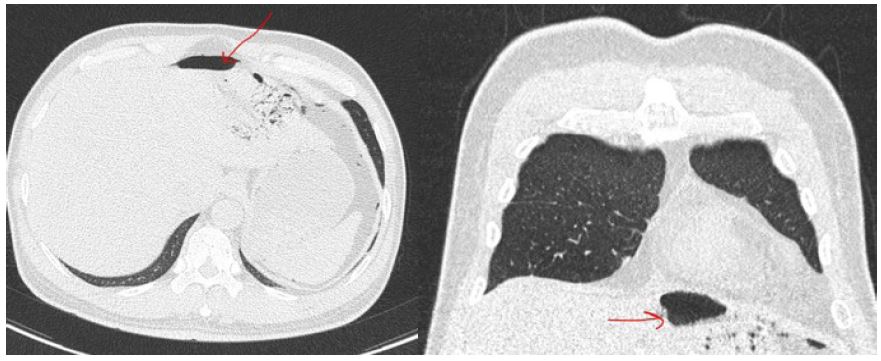
Figure 1: Showing air under diaphragm.
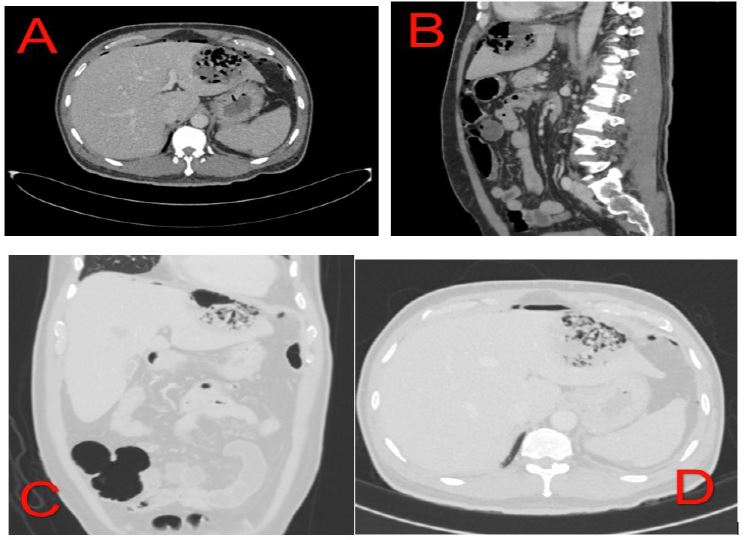
Figure 2: A and B showing gas forming liver abscess with perforation in soft tissue window C and D showing the liver abscess and the perforation in lung window.
General surgery was consulted to rule out perforated viscous and CT of the abdomen and pelvis without contrast was requested as he was having kidney injury, and the CT showed multiple, variable size, hypodense, non-enhancing focal lesions in the liver with pneumoperitoneum. The largest lesion was in the left lobe. It contained excessive air bubbles and its anterior and medial wall showed defects and subsequent air tracking into the upper peritoneal cavity. It measured about 68 x 63 mm with other smaller lesions were noted in the right lobe. These features were suggestive of multiple liver abscesses with perforation (Figure 2).
The patient was shifted to the ICU due to sepsis secondary to possibly hepatic Patient was admitted to intensive care unit and Interventional Radiology (IR), Gastroenterology (GI), Nephrology, and Infectious Diseases (ID) were consulted. The decision was made to manage this patient in multimodal treatment with antibiotic, Ultrasound-guided IR drainage of the abscess and Endoscopic Retrograde Cholangiopancreatography (ERCP).
IR drainage revealed thick and red fluid that was sent for culture and grew non ESBL Klebsiella pneumonia. GI performed ERCP with endoscopic sphincterotomy which showed no dilation of the biliary tree. Liver enzymes and bilirubin continued to rise and despite the performed treatment measures and supportive care, the patient continued to deteriorate both clinically and biochemically. Gastroenterology performed cholangiogram and observed that the abscess in the left lobe is occupied massively with necrotic tissue. This explained the patient’s deterioration and proved the requirement of surgical intervention.
He was taken to the operating theatre for diagnostic laparoscopy drainage of the liver abscess in segment 5, necrosectomy of the necrotic liver abscess in segment 2/3, and washout and drainage. Findings Intra-operatively showed a large liver abscess in segment 5 and an evidence of necrotic perforated abscess at segment 2/3. In addition, 0.5 L of bile was in the abdominal cavity.
A sample of the liver tissue and culture of the liver abscess pus was sent for examination. Later in the same evening, he was taken back to the OR for explorative laparotomy due to hemodynamic deterioration caused by bleeding from the liver surface. 5 L of blood and clots were in the abdominal cavity. No definite bleeding source was identified. There was oozing from the liver surface of segment 2 and from the under surface of the diaphragm and falciform ligament. Left lateral segmentectomy was performed using combination of diathermy, harmonics, and GIA stapler. Following the second operation, he remained intubated as his course was complicated by Disseminated intravascular coagulopathy (DIC), septic shock, and hepatorenal syndrome. He required pressor support and was started on CRRT. 3 days after the surgery, he was extubated. The pathology report confirmed acute inflammatory cell collection forming an abscess with presence of necrosis. No definite pathogen was identified and no signs of dysplasia or malignancy were present.
US was done before discharge which showed no liver or gallbladder abnormalities and patient was discharged from the hospital.
Discussion
Pyogenic liver abscess is the most frequent type of visceral abscess, accounting for more than 40% of peritoneal abscesses. It can present as a complication of hepatobiliary disease, previous GI surgeries or post-trauma. The primary risk factor for PLA is biliary tract disease, including biliary tract obstruction, cholelithiasis and cholangitis. Other risk factors include liver cirrhosis, diabetes, immunocompromised patients, and the use of immunosuppressive agents [4]. The microbiology depends on the initial source of the abscess. The overall most common isolated pathogens are E. coli and Klebsiella pneumoniae. Gas forming pyogenic liver abscess is an uncommon and potentially fatal disease that accounts for 7% to 24% of pyogenic liver abscesses. Nevertheless, the incidence of GFPLA has been increasing due to advancements in medical technology in the area of liver diseases [5]. Compared to pyogenic liver abscess, GFPLA is associated with higher morbidity and mortality [6-8]. One of the complications of GFPLA is spontaneous rupture within the peritoneal cavity causing pneumoperitoneum, which is rare and life threatening. It occurs in 5.4% of all liver abscesses [9].
Pyogenic liver abscess can present with nonspecific symptoms and signs; thus, a high clinical suspicion plays an important role in early diagnosis. The most common signs and symptoms are fever and upper abdominal pain, and hepatomegaly [10]. Some patients have non-specific, subtle symptoms, which may lead to a delay in the diagnosis. Pneumoperitoneum is an unusual presentation for a liver abscess. Air under the diaphragm is usually attributed to a perforated hollow viscus not as perforated liver abscess. The imaging modalities used to diagnose liver abscesses are ultrasonography and CT scan. Ultrasound has 80 to 90% sensitivity. It can be used to make a rapid diagnosis, but it is operator-dependent, and it might not pick up small, solitary abscesses. On the other hand, CT has a higher sensitivity rate (95-98%) and should be used whenever possible [10]. CT allows for the detection of intrahepatic collections as small as 0.5 cm. This advantage is noticeable in patients who have several small pyogenic abscesses [11].
The mainstay of treatment for pyogenic liver abscess is appropriate antibiotic coverage, source control, and adequate drainage. Antibiotics solely can successfully treat solitary or numerous small pyogenic abscesses (<2 cm). Broad-spectrum antibiotics should cover the commonly isolated pathogens such as Streptococci, enteric gram-negative bacilli, and anaerobes, including E. histolytica should all be included in the empiric regimen until culture and sensitivity further guides the antibiotic choice. Aminoglycoside with metronidazole or clindamycin, or a beta lactam antibiotic with anaerobic coverage can be used. Penicillin can be added to aminoglycoside in case of PLA secondary to biliary disease [11]. It is crucial to address the source of infection. Any intrinsic biliary source must be addressed, as well as any biliary obstruction. If a secondary cause is suspected, such as patients with a surgically correctable lesion, including appendicitis or biliary blockage, an appendectomy or ERCP with drainage can be performed. Percutaneous drainage is indicated when an abscess is larger than 5 cm in diameter, pyrexia persists after 48 to 72 hours of appropriate antibiotic therapy, or in the case of clinical or imaging characteristics suggestive of imminent perforation. Every aspirate material should be sent for Gram staining and culture (both aerobic and anaerobic). Since anaerobic culture necessitates treatment, it should be expressly specified on the laboratory requisition [12]. On the other hand, surgical intervention is required in cases of multiloculate liver lesions, no response to broad-spectrum antibiotic treatment, failure of laparoscopic deroofing of PLA, ruptured PLA, or failure of percutaneous drainage [13]. There are various reports that compares percutaneous vs. surgical management of pyogenic liver abscesses; however, there are no prospective randomized studies.
It has been previously suggested to take an aggressive approach, such as an initial surgical procedure rather than percutaneous drainage attempts in two types of situations. The first is related to the risk of failing percutaneous treatment which includes gas-forming abscesses, multiloculated abscess, and septic shock at presentation. The second is linked to factors associated with high mortality: elevated American Society of Anesthesiologist (ASA) score, acute physiology and chronic health evaluation score (APACHE) >15, severe sepsis, pleural effusion, and a malignant pyogenic liver abscess origin [14]. On the contrary, there are recent several studies that reported successful non-surgical treatment of ruptured pyogenic liver abscess [15,16]. Although they were successfully treated without surgical intervention, these cases had prolonged hospital stay (40-52 days).
Our patient initially presented with a ruptured pyogenic liver abscess. He first underwent drainage by interventional radiology, but he continued to deteriorate. He followed a complicated course with sepsis and acute kidney injury. He had to undergo surgical drainage of the liver abscess since his clinical course continued to deteriorate and improved significantly after it, and discharged from the hospital at day 28.
With the conflicting data available, it is unclear whether an early surgical intervention in this patient would have resulted in a better outcome in terms of length of stay and complications, but we think the decision for his initial management was adequate and was agreed on with multidisciplinary team.
Conclusion
Ruptured gas-forming pyogenic liver abscess is a rare, life-threatening complication. It can present in several ways; however, pneumoperitoneum is a rare presentation. Pneumoperitoneum is commonly been diagnosed for a ruptured hollow viscus, hence a high index of suspicion is the key to preventing misdiagnosis of a ruptured pyogenic liver abscess with it. Early diagnosis is associated with better outcomes in terms of hospital length of stay and prognosis.
References
- Abbas MT, Khan FY, Muhsin SA, Al-Dehwe B, Abukamar M, et al. Epidemiology, Clinical Features and Outcome of Liver Abscess: A single Reference Center Experience in Qatar. Oman medical journal. 2014; 29: 260-263.
- Smith RS. Pyogenic liver abscess in the aged. The American Journal of Surgery. 1944; 63: 206-213.
- Thng CB, Tan YP, Shelat VG. Gas-forming pyogenic liver abscess: A world review. Annals of hepato-biliary-pancreatic surgery. 2018; 22: 11-18.
- Altemeier WA, Culbertson WR, Fullen WD, Shook CD. Intra-abdominal abscesses. Am J Surg. 1973; 125: 70-79.
- Lai Y, Su Y, Chang W. Ruptured hepatic abscess mimicking perforated viscus. International Journal of Infectious Diseases. 2008; 12: e95–e97.
- Chen SC, Tsai SJ, Chen CH, Huang CC, Lin DB, et al. Predictors of mortality in patients with pyogenic liver abscess. Neth J Med. 2008; 66: 196-203.
- Zhang Y, Zang GQ, Tang ZH, Yu YS. Fatal gas-forming pyogenic liver abscess due to Klebsiella pneumoniae. Rev Inst Med Trop Sao Paulo. 2013; 55: 144.
- Chou FF, Sheen-Chen SM, Chen YS, Lee TY. The comparison of clinical course and results of treatment between gas-forming and non-gas-forming pyogenic liver abscess. Arch Surg. 1995; 130: 401-405.
- Chalh O, Sibbou K, El Fenni J. Ruptured Pyogenic Liver Abscess as an Uncommon Cause of Pneumoperitoneum. J Belg Soc Radiol. 2022; 106: 13.
- Kumar SK, Perween N, Omar BJ, Kothari A, Satsangi AT, et al. Pyogenic liver abscess: Clinical features and microbiological profiles in tertiary care center. Journal of family medicine and primary care. 2020; 9: 4337-4342.
- Holzheimer RG, Mannick JA. Surgical Treatment: Evidence-Based and Problem Oriented,. Journal of Trauma-Injury Infection and Critical Care. 2001.
- Chemaly RF, Hall GS, Keys TF, Procop GW. Microbiology of liver abscesses and the predictive value of abscess gram stain and associated blood cultures. Diagn Microbiol Infect Dis. 2003; 46: 245-248.
- Su YJ, Lai YC, Lin YC, Yeh YH. Treatment and prognosis of pyogenic liver abscess. Int J Emerg Med. 2010; 3: 381-384.
- Alkofer B, Dufay C, Parienti J, Lepennec V, Dargère S, et al. Are Pyogenic Liver Abscesses Still a Surgical Concern? A Western Experience. Hpb Surgery. 2012; 1-7.
- Herschorn S, Ryu SB. Ruptured Gas-forming Pyogenic Liver Abscess into the Peritoneal Cavity Treated Successfully with Medical Treatment. The Korean Journal of Gastroenterology. 2018.
- Motoyama T, Ogasawara S, Chiba T, Suzuki E, Yokota H, et al. Successful Non-surgical Treatment of Ruptured Pyogenic Liver Abscess. Internal Medicine. 2013.
