
Open Access, Volume 9
Management of pyometra after Lefort colpocleisis
Anna Trikhacheva1*; Donna Mazloomdoost2
1Department of Urogynecology, Walter Reed National Military Medical Center, Inova Fairfax, USA.
2Department of Urogynecology, Inova Fairfax, USA.
Anna Trikhacheva
Department of Urogynecology, Walter Reed National Military Medical Center, Inova Fairfax, USA.
Email: ann_trik@hotmail.com
Received : April 03, 2023,
Accepted : May 10, 2023
Published : May 16, 2023,
Archived : www.jclinmedcasereports.com
Abstract
LeFort colpocleisis is a highly effective surgical treatment for pelvic organ prolapse. Postoperative pyometra is a rare, but serious complication. Treatment options has been described only in few case reports. We present a case of post LeFort pyometra that was managed conservatively with drains and antibiotics.
Keywords: Abscess; Pyometra; LeFort; Colpocleisis.
Abbreviations: POP: Pelvic Organ Prolapse; POD: Postoperative Day; FIG: Figure; CT: Computer Tomography.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Trikhacheva A (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Trikhacheva A, Mazloomdoost D. Management of pyometra after Lefort colpocleisis. Open J Clin Med Case Rep. 2023; 2036.
Introduction
LeFort colpocleisis is an obliterative surgical treatment for pelvic organ prolapse (POP). The procedure is associated with shorter operative time, higher levels of patient satisfaction, and lower rate of complications and failure than reconstructive surgeries [1]. Postoperative pyometra is a rare, but serious complication [2,3]. Only a few case reports have previously been reported on post LeFort pyometra and its management. We present a case of postoperative pyometra managed with antibiotics and abscess drainage.
Case Presentation
A 78-year-old G2P2002 resented with stage 2 POP and stress urinary incontinence. The patient elected to undergo LeFort colpocleisis, levator myorrhaphy, midurethral sling, and cystoscopy.
On post-operative day (POD) 9, the patient presented with fever and vulvar pain. Her exam revealed induration along left labia extending lateral to the anus. Computer tomography (CT) showed an abscess (Figure 1). Patient underwent incision and drainage and drain placement in the operating room. After 48 hrs of intravenous Piperacillin/Tazobactam she was discharged home with oral Amoxicillin/Clavulanic acid to complete a 14-day course.
The patient represented on POD 18 again with fever and worsening perineal pain. She was febrile, white blood cell count was elevated, and CT showed a similar fluid collection in the uterus and re-accumulation of the perineal abscess (Figure 2). She was admitted for antibiotic administration and interventional radiology was consulted for drainage of the two areas of abscesses. On POD 19, a drain was placed vaginally into the uterus as well as a second drain into the perineal collection (Figures 3 & 4). The cultures ultimately revealed multidrug resistant Escherichia coli and Enterococcus raffinosus. She was subsequently treated with Meropenum. The patient improved and was discharged home on POD 27 without any further treatment necessary.

Figure 1: POD 9 – Pelvic CT shows 7 x 4.3 x 5.2 cm lower pelvic/perineal abscess (thin red arrow) with fluid-filled uterus (thick red arrow) consistent with pyometra. Bladder shown with a thin black arrow.

Figure 2: POD 18 – Reaccumulation of the abscess that was multilocular (outlined by a red oval) extending from the level of the posterior vagina to the left of midline and extending superiorly for about 10 cm to the level of the lower uterine segment. Fluid within the endometrial cavity measuring 4.6 x 3.3 cm (thick red arrow). Bladder shown with a thin black arrow.
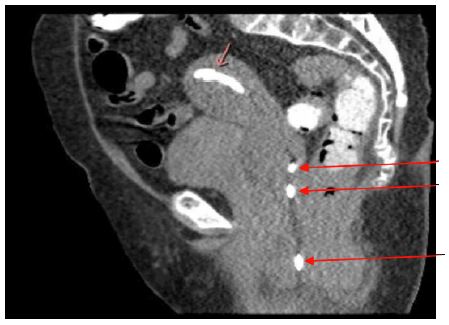
Figure 3: Drain placed by Interventional Radiology under CT-guidance into the uterine as shown by a short red arrow. The drain shows up bright on this image. Visible portions of the drain within the abscess tract are pointed out by the long red arrow. The bladder is shown by the thick black arrow.
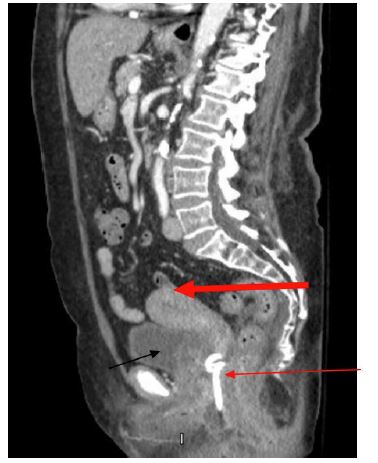
Figure 4: Drain placed within the left paravaginal portion of the abscess as shown by the thin red arrow. The drain appears bright in this image. The uterus is shown by the thick red arrow. Notice the fluid within the uterine cavity is drained after the drain placement. The bladder is shown by the thin black arrow.
Discussion
Pyometra after a LeFort colpocleisis is a rare and serious complication. It can be managed surgically via a hysterectomy or conservatively using drains. In this report we demonstrate, a patient that was managed conservatively with great success. This allowed the patient to avoid a large surgery with possible further complications.
References
- MuellerMG, Ellimootil C, Abernethy MG, Mueller ER, Hohmann S, et al. Colpocleisis: a safe, minimally invasive option for pelvic organ prolapse. Female pelvic Med Reconstr Surg. 2015; 21: 30-33.
- Yasa C, Ugurlucan FG, Yalcin O. Management of pyometra after LeFort colpocleisis resistant to drainage. Int Urogynecol J. 2016; 27: 645-646.
- Shayya RF,WeilsteinMM, Lukacz ES. Pyometra after LeFort colpocoleisis resolved with interventional radiology. Obstet Gynecol. 2009; 113: 566-568.
