
Open Access, Volume 9
Chlorine exposure accidents characteristics and recent progress in treatment
Chen-qian Zhao1; Qian Fang2; Meng-meng Liu3; Chun-xu Hai1*; Xiao-di Zhang1*
1Department of Toxicology, Shaanxi Key Lab of Free Radical Biology and Medicine, the Ministry of Education Key Lab of Hazard Assessment and Control in Special Operational Environment, School of Public Health, Fourth Military Medical University, Xi’an 710032, China.
2School of Nursing, Medical College of Soochow University, Suzhou 215006, China.
3Department of Health Service, Logistics of University of Chinese People’s Armed Police Force, Tianjin 300309, China.
Xiao-di Zhang & Chun-xu Hai
Department of Toxicology, Shaanxi Key Lab of Free Radical Biology and Medicine, the Ministry of Education Key Lab of Hazard Assessment and Control in Special Operational Environment, School of Public Health, Fourth Military Medical University, Xi’an 710032, China.
Email: zhangxiaodi@fmmu.edu.cn & cx-hai@fmmu.edu.cn
Received : Mar 31, 2023,
Accepted : May 09, 2023
Published : May 16, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: As a choking agent, chlorine (Cl2) exposure accidents occur frequently, which brings great threat to safety of people’s lives and property.
Objective: In this work, the study systematically reviewed the Cl2 exposure accidents from 1967 to 2022, and would like to find valuable new insights and paths in treatment of Cl2 poisoning.
Methods: Eight databases (Wanfang, VIP, CNKI, CBM, Pubmed, Embase, PsycINFO and Cochrane) were searched from the date of establishment to January 2022.
Results: A total of 159 articles involving 14,197 people with acute Cl2 exposure were included. 125 articles reported on accident types. The most frequent type of accident was industry (71.2%), followed by swimming pools (17.6%). Common symptoms were mainly manifested in the eyes, oropharynx, skin, upper and lower respiratory tract, etc. Laboratory tested mainly include physical examination, blood, and X-ray examination to provide reliable basis for treatment. Conventional treatmented options include glucocorticoids, nebulized inhalation, oxygen inhalation, anti-inflammatory, etc. Extracorporeal Membrane oxygenation (ECMO) was used in critically ill patients.
Conclusions: Timely and effective treatment is extremely important for the life safety of patients exposed to Cl2. This study provides the latest first-hand information for Cl2 exposure accidents characteristics and management strategies, which are mainly related to treatment, and can provide reference and ideas for drug screen and new treatment plans in the future.
Keywords: Chlorine; Chlorine exposure accidents; Chlorine poisoning; Lung injury; Accident statistics.
Abbreviations: Cl2: Chlorine; ECMO: Extracorporeal Membrane Oxygenation; HOCl: Hypochlorous Acid; HCl: Hydrochloric Acid; ARDS: Acute Respiratory Syndrome; ATP: Adenosine Triphosphate; FDP: Fructose-1,6-Bisphosphate; PTX: Pentoxifylline.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Zhang XD & Hai Cx (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Zhao CQ, Fang Q, Liu MM, Hai CX, Zhang XD. Chlorine exposure accidents characteristics and recent progress in treatment. Open J Clin Med Case Rep. 2023; 2035.
Introduction
Chlorine (Cl2) is a kind of yellow-green toxic gas. Up to now, Cl2 is still the most common of all the inhaled toxicants. It is widely used in household disinfection and industrial production. Accidental Cl2 exposure may occur during the production, transportation and use of Cl2. So far, many Cl2 exposure accidents have been reported all over the world. For example, the largest Cl2 leak to date occurred in South Carolina in 2005 [1], and the most recent was a Cl2 leak at the Aquatics Centre in London, England, on March 23, 2022 [2]. In fact, Cl2 leaks are not limited to accidental leaks, but have also been used as a chemical weapon for large-scale deliberate releases in wars and terrorist activities [3], have caused a large number of casualties.
Cl2 poisoning has a rapid onset and is inhaled through the respiratory tract. Various Cl2 injury case reports and studies have shown that exposure to 3 ppm Cl2 can cause mild irritation symptoms such as photophobia, lacrimation, and throat discomfort; 5-15 ppm cause moderate irritation symptoms such as expectoration and chest tightness; >15 ppm causes severe lung irritation, causing symptoms such as dyspnea, retrosternal pain; but exposure to ≥430 ppm for 30 mins or less results in death [4]. When Cl2 is inhaled, it reacts with the solution on the mucosa and alveolar to produce hypochlorous acid (HOCl) and hydrochloric acid (HCl). The toxicity of Cl2 is mainly due to its oxidation potential. The released ions can pass through the cell wall and produce oxygen free radicals [5]. The injury can lead to bronchospasm, edema, epithelial cell erosion, shedding, etc. In addition to causing epithelial cell damage, the presence of HOCl and hypochlorite in the airway can also cause inflammatory reactions. Inflammatory cells and free radicals destroy cell membrane and protein, resulting in the destruction of alveolar cells and endothelial cells of adjacent capillaries, increasing the permeability of pulmonary vascular endothelial cells, and ultimately leading to pulmonary edema and acute respiratory syndrome (ARDS) [6]. Various treatment modalities exist for acute Cl2 exposure. At present, the conventional treatment is mainly symptomatic treatment such as oxygen inhalation, glucocorticoid, bronchodilator, and anti-inflammatory, but there is no effective treatment drug.
On the basis of the previous literature [7], this study collected Cl2 poisoning accidents in a longer time range through an open source database, especially from 2017 to 2022. The study observed the events characteristics and clinical management systematically in order to find out some trails for the treatment and public health management after Cl2 exposure accident in the future.
Methods
Search strategies
From November 2021, this study systematically searched 8 databases (Wanfang, VIP, CNKI, CBM, Pubmed, Ebmase, PsycINFO and Cochrane) for eligible articles on Cl2 exposure accidents in Chinese and English. Medical Subject Headings (MeSH) and free-text terms related to Cl2 spill accidents. MeSH terms used include "Chlorine", "Gas Poisoning", "Chemically-Induced Disorders", etc. An example of a search strategy for the database PubMed is given in the appendix.
Inclusion criteria
The study excluded duplicate reports of the same accident. Review articles were excluded unless the article also contained a case report or case series. Chronic Cl2 poisoning (occupational disease) and exposure to mixture poisoning are excluded.
Literature screening and data extraction
Two researchers first independently screened literature based on study titles and abstracts. Then, after reading the full text, a decision was made whether to include the literature in this study. Two reviewers extracted data based on predesigned data and cross-checked them. Differences in data extraction and literature screening, if any, were explored with a third investigator until agreement was reached. The extracted data included the first author of the article, the age and gender of the participants, the time and place of the accident, the number of casualties, clinical symptoms, interventions, physical examination results, and more.
Data analysis: Statistics were made using descriptive statistical methods.
Results
Search results
A total of 7483 potentially eligible literatures were identified through systematic retrieval of 8 databases. After reviewing the title and summary, 3285 records were excluded. Read the remaining 4198 articles for further screening, excluding 3970 articles not related to this study. 69 articles were excluded because they were unable to obtain the full text. Finally, 159 articles were included in this analysis (Figure 1) [8-165].
A total of 14,197 people were identified as exposed to Cl2, of which 159 articles reported the area of occurrence and 125 articles reported the type of accident. There were 4641 males and 3478 females. The age of contact ranged from 3 months to 90 years. Over 99% of cases survived to hospital discharge; 57 died (0.004%). Complications included chronic pharyngitis, pulmonary tuberculosis, pneumonia, bronchitis, bronchial asthma, myocarditis, and so on.
Characteristics of time distribution of Cl2 exposure accidents
This paper maked statistics on Cl2 exposure accidents in the world from 1967 to 2020. The statistical results are shown in Figure 2. It can be seen that the high incidence of Cl2 exposure accidents can be mainly distributed in three stages: (1) The first stage is from 2000 to 2002. The Cl2 exposure accidents occurred in 7 cases (4.3%), 9 cases (5.5%) and 5 cases (3.1%). (2) The second stage is from 2004 to 2006. Compared with the first stage, Cl2 exposure accidents had increased, with 9 cases (5.5%), 6 cases (3.7%) and 10 cases (6.1%), respectively. (3) The third stage is from 2011 to 2014. Since 2015, the frequency of accident has been no peak, and stabilized about 1.2%.
Categories of Cl2 exposure accidents
Among the Cl2 exposure accidents, 89 cases (71.2%) were industrially exposed to Cl2; 22 cases (17.6%) were related to swimming pool; 6 cases (4.8%) were related to Cl2 produced by hypochlorite reaction, and 2 cases (1.6%) were related to traffic accidents, military, laboratory, and swimming pool plus industrial exposure (Figure 3).
Clinical features of Cl2 poisoning
Some clinical signs and symptoms were be collected that may be related to Cl2 exposure (Table 1). Eye symptoms mainly include: photophobia, lacrimation, ophthalmalgia, blurred vision; oropharyngeal symptoms include: Pharyngeal congestion and swelling, burning sensation; skin symptoms such as sweating, paleness, and cyanosis. The upper respiratory tract was mainly characterized by vocal cord edema, hoarseness, swollen tonsils, sore throat, dry throat, laryngospasm, sneezing and other symptoms; the lower respiratory tract was mainly characterized by cough, expectoration, dyspnea, shortness of breath, chest tightness, chest pain, pulmonary atelectasis, acute pulmonary edema, respiratory failure. Some patients experienced limb symptoms such as difficulty walking, limb numbness, and gait deformity. There even had central nervous system-related symptoms such as: unconsciousness, sleepiness, coma, headache, dysphoria, slurred speech, and tetany. Gastrointestinal tract symptoms such as nausea, vomiting, epigastric pain, and upper gastrointestinal bleeding were also present. Cardiogenic shock, sinus bradycardia, palpitations, arrhythmia, flustered, elevated blood pressure, atrial premature beats, heart arrest appeared in the cardiovascular system. A small number of patients had symptoms of gatism and hypourocrinia in excretion.
Examination results of Cl2 poisoning
At the same time, this study also summarized and classified the laboratory test results (Table 2). Physical examination showed moist rales and/or wheezing in the lungs, rough breathing sounds in bilateral lungs, and triple concave sign (+). Blood tests showed increased white blood cells, elevated erythrocyte sedimentation rate, slightly elevated serum sodium+, Cl-, hypokalemia, hypoxemia, and hypercapnia. Elevated white blood cell counts and blood sedimentation suggested that an inflammatory response may have occurred in the patients’ body. Renal function examination showed that some patients had increased urea nitrogen, serum creatinine and urinary protein (+). A series of indicators of liver function, such as aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, aspartate aminotransferase and serum γ-glutamyl transpeptidase were all elevated. A small number of patients showed abnormal manifestations such as ST segment depression, T wave inversion or low level, I-degree atrioventricular block, and left ventricular hypertension in ECG examination. Almost all patients underwent X-ray. The examination results showed that the hilar shadow increased and blurred, the lung texture was enhanced and disordered, the transparency of the lung field was reduced, and scattered dotted, a low density patch in the middle and upper fields of the two lungs and other pulmonary infection and disease states.
Clinical treatment of Cl2 poisoning
In this study, the treatment methods obtained in 163 literatures were classified and summarized (Table 3). Dexamethasone was the mainstay of glucocorticoid treatment, and methylprednisolone were used in severe cases [29,30,35,36,37,40,43,44,46,67,78,84,88,90,95,97]. The main treatment options for atomization inhalation are: alternate aerosol inhalation of 2-5% sodium bicarbonate solution with dexamethasone, gentamicin, aminophylline, α-chymotrypsin, distilled water [102,122,134,145] 0.25-0.5% isoproterenol or 0.2% salbutamol or dexamethasone aerosol, each inhalation for half a minute to a few minutes [82,83,85,86, 88]. Isoproterenol and dexamethasone mixture and sodium bicarbonate are used in the treatment of throat spray.
Severe cough could be given codeine tablets oral or intravenous with promethazine or wintermin. Intravenous aminophylline was given to patients with dyspnea. Morphine and propofol combined with midazolam are used for analgesic and sedative effects, respectively [106, 109, 110, 123, 126]. Chloral hydrate could be given when patients are agitated. When nasal bleeding occurred, the nasal vestibular was pressed in time and the mucosal blood vessels are contracted by instilling 1-2% ephedrine [139, 140, 144, 156]. Patients with vomiting were given intramuscular injection of vitamin B6. Mucosal irritation symptoms: local administration of 2-3% sodium bicarbonate could be used to repeatedly flush the hyperemia site, after flushing, hydrocortisone eye drops or antibiotic eye drops could be applied to the conjunctiva [134, 148]; 1-2% ephedrine could be dropped into the nasal cavity liquid; pharynx could use Huasu tablets or Golden Throat Lozenges [73-89]. Patients with pulmonary edema were given intermittent use of 1% dimethicone aerosol to eliminate air bubbles in the respiratory tract.
Patients whose eyes were irritated by Cl2 should be flushed with water or normal saline; 5% cortisone eye drops, chloramphenicol eye drops; erythromycin eye ointment should be applied to the eyes at night. Most patients who inhale Cl2 would have an inflammatory reaction in their body, and they need to be given 2nd and 3rd generation cephalosporins or quinolones for anti-infective treatment. Adenosine Triphosphate (ATP), coenzyme A, inosine, Fructose-1,6-Bisphosphate (FDP) were usually used for myocardial protection. Some critically ill patients used Extracorporeal membrane oxygenation (ECMO) and ventilator for life support [95-112].
We also found a use of integrated traditional Chinese and Western medicine drug “Chaihuangshenquduguben” (the main components include: bupleurum, scutellaria, rhubarb, rhizoma coptidis, red peony root, radix scrophulariae, salvia miltiorrhiza, ginseng, radix rehmanniae, honeysuckle, forsythia, fructus aurantii, gardenia, licorice) used in clinical Cl2 poisoning treatment [147]. This treatment plan has a significant effect on improving pulmonary edema. It is a typical case of clinical treatment of Cl2 poisoning. However, the basic research on the mechanism of action and the principle of effect still needs to be further improved and deepened.
Experimental research progress
With the development of laboratory research in recent years, some promising treatments for Cl2 poisoning have been proposed, but most are still based on antioxidant and anti-inflammatory. At present, N-acetyl-L-cysteine, iron chelating agent and a low molecular antioxidant, AEOL10150 [4,5,7,166] and so on, are the rugs reported in the laboratory about antioxidant damage. Anti-inflammatory drugs include triptolide, nitrite, mometasone [3,10,15].
Pentoxiflline (PTX) is widely used in various vascular injury diseases, as a phosphodiesterase inhibitor. Our group has discovered that compared with Cl2 group, PTX intervention could down-regulate levels of MDA, GSSG, TOM 20 protein expression and activities of Na+, K+-ATPase and Ca2+, Mg2+ -ATPase, and upregulate GSH level, GSH/GSSG ratio and CAT protein expression level in rat lung tissues [167,172]. Additionally, the results also showed that PTX exerted an inhibition effect on protein expressions of HIF-1α, VEGF and occludin, and increased the level of E-cadherin in rat lung tissues [168,172,174]. In order to further explore the mechanism of PTX against oxidative damage and mitochondrial protection, we conducted a series of in vitro experiments [169]. The results show that compared with the control group, the green fluorescence intensity of Mito Tracker Green and Rho 123 decreased, while the red fluorescence intensity of Mito SOX increased after t-BHP (tert-butyl hydroperoxide) treatment. Compared with t-BHP group, PTX increased cell viability, decreased the levels of LDH, MDA and GSSG in cell culture supernatant, SOD activity and Nrf-2 protein expression in HUVECs (human umbilical vein endothelial cells), and increased levels of GSH, GSH/GSSG ratio, SOD1 protein expression, ATP, and the activities of Na+, K+-ATPase and Ca2+, Mg2+ -ATPase [169]. As an original drug, the biggest advantage of PTX is that the new use of old drug can not be used for clinical application safety evaluation.
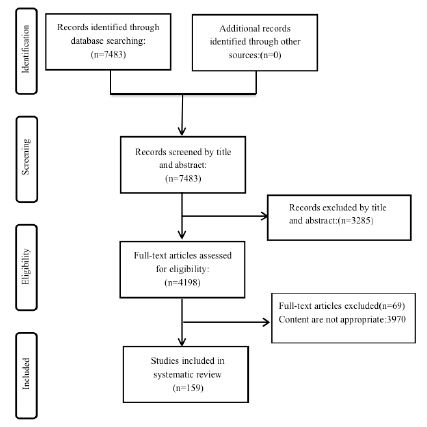
Figure 1: Flow Chart of Literature Identification and Selection.
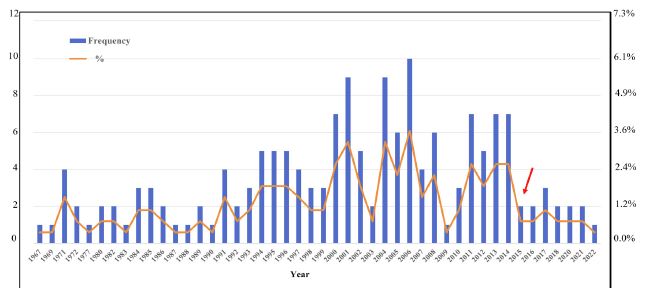
Figure 2: Statistics of the Frequency and Rate of Cl2 Exposure Accidents from 1967-2022. Red Arrow: Events Drop Point.
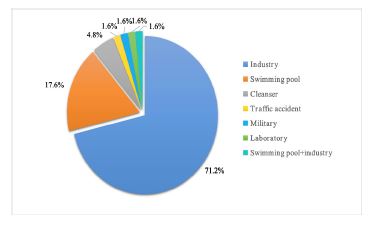
Figure 3: Statistics of the Types of Cl2 Exposure Accidents from 1967 to 2022.
Table 1: Classification of Clinical Features after Cl2 Poisoning.
| Body Region | Symptoms |
|---|---|
| Ophthalmic | Photophobia, lacrimation, ophthalmalgia, blurred vision |
| Oropharynx | Pharyngeal congestion and swelling, burning sensation |
| Skin | Sweat, pale complexion, cyanosis |
| Upper respiratory tract | Vocal cord edema, hoarseness, tonsil swelling, Sore throat, dry throat, laryngospasm, sneeze |
| Lower respiratory tract | Cough, expectoration, dyspnea, shortness of breath, chest distress, chest pain, pulmonary atelectasis, acute lung edema, respiratory failure |
| Limbs | Difficult to walk, limb numbness, gait deformity |
| Central nervous system | Unconsciousness, sleepiness, coma, headache, dysphoria, slurred speech, tetany |
| Gastrointestinal tract | Nausea, vomit, epigastric pain, upper gastrointestinal bleeding |
| Cardiovascular system | Cardiogenic shock, sinus bradycardia, palpitation, arrhythmia, flustered, elevated blood pressure, atrial premature beats, heart arrest |
| Defecate and urinate | Gatism, hypourocrinia |
Table 2: Laboratory Examination after Cl2 Poisoning.
| Laboratory examination | Results |
|---|---|
| Physical examination | Pulmonary moist rales and/or wheezes, rough breathing sounds in both lungs, bubbling sound, three depressions sign (+) |
| Blood examination | Leukocyte increase, blood sedimentation increase, blood Na +, Cl slightly elevated, hypokalemia, hyoxemia, hypercapnia |
| Renal function tests | Increased urea nitrogen, elevated serum creatinine, urine protein (+) |
| Liver function test | Aspartic acid aminotransferase, alanine aminotransferase, alkaline phosphatase, aspartate aminotransferase and serum Y-glutamyl transpeptidase increased |
| ECG | ST segment depression, T wave inversion or low level, I-degree atrioventricular block, left ventricular high voltage |
| X-ray | The hilar shadow is enlarged and blurred, lung texture enhanced and disorder, lung field transparency decreases, scattered, a low density patch in the middle and upper fields of the two lungs |
Table 3: Laboratory Examination after Cl2 Poisoning.
| Therapy | Scheme |
|---|---|
| Glucocorticoid | Dexamethasone, severe administration to methylprednisolone |
| Atomization inhalation | Alternate aerosol inhalation of 2-5% sodium bicarbonate solution with dexamethasone, gentamicin, aminophylline, a-chymotrypsin, distilled water, 0.25%-0.5% isoproterenol or 0.2% salbutamol or dexamethasone aerosol, each inhalation for half a minute to a few minutes |
| Laryngeal spraying | Isoproterenol and dexamethasone mixture, sodium bicarbonate |
| Severe cough | Codeine tablets (PO); promethazine or wintermin (IV) |
| Dyspnea | Aminophylline (IV) |
| Analgesia | Morphine |
| Sedation | Propofol combined with midazolam |
| Restlessness | Chloral hydrate |
| Nasal bleeding | Compress the nasal vestibule and instill 1%-2% ephedrine to constrict the mucosal blood vessels to stop bleeding |
| Vomiting | Vitamin B6 (IM) |
| Mucosal irritation | Locally given 2%-3% sodium bicarbonate repeatedly washing the congestion site, after washing the conjunctiva can drop hydrocortisone eye drops or antibiotic eye drops; cydiodine buccal tablets or Golden Throat Lozenges available in throat |
| Pulmonary edema | 1% dimethicone aerosol |
| Ocular region | Rinse with water or normal saline; 5% cortisone eye drops, chloramphenicol eye drops; erythromycin eye ointment at night |
| Anti-infection | 2nd and 3rd generation cephalosporins or quinolones |
| Myocardial protection Equipment | ATP, coenzyme A, inosine, FDP ECMO, ventilator |
Discussion
Through the statistical analysis of the types of Cl2 exposure accidents, this study found that most exposure accidents were related to civil industrial use, which accounted for as high as 71.2%. There have been two military-related accidents, the most recent of which was the Syrian armed conflict in 2014, in which 15 people were injured. The main symptoms were related to respiratory tract injury. At present, symptomatic treatment is still the mainstay. Interestingly, this study found that the frequency of Cl2 exposure events was in a high-low cycle before 2015, but the accident rate has kept a lower level after 2015. This change could be related to the increasing emphasis on emergency management investment by countries around the world.
After a sudden Cl2 expose, saving lives is of paramount importance. How to deliver treatment in a timely and effective manner is an ongoing concern in many countries, while still presenting challenges for medical staff.
It is known that the main symptoms of Cl2 injury are manifested in the respiratory system. In this study, it was found that the main symptoms of the patients were mainly the upper and lower respiratory tract, such as dyspnea, acute pulmonary edema, respiratory failure and so on. During the study, a massive Cl2 spill occurred on 23 March 2022 at the Aquatics Centre in London, UK, injuring 29 people, most of whom were taken to hospital for breathing difficulties. However, the mechanism of injury to the respiratory system remains unclear. This study need to continue to pay attention to the relevant literature at the forefront.
The majority of the Cl2 exposure animal studies show that a series of inflammatory reactions occur in the body after Cl2 inhalation. Blood tests results showed increased white blood cell count and erythrocyte sedimentation rate. X-ray showed reduced transparency of the lung fields and scattered patchy shadows in both lungs. The results of these tests showed that there was inflammatory response in the body. It has been reported that inflammatory factor storm may be the main pathological cause of pulmonary lesions such as pulmonary edema and respiratory distress after Cl2 exposure. However, its specific molecular mechanism still needs to be further explored.
New solutions for Cl2 poisoning treatment are constantly being sought, among which Yue et al. proposed a new scheme of combined treatment of traditional Chinese medicine and western medicine in the process of clinical treatment of 1539 cases of sudden mass Cl2 poisoning [147]. On the basis of comprehensive treatment, the use of Fengnuo's combination with vitamin B6, short-course anisodamine combined with dexamethasone pulse therapy and the traditional Chinese medicine“ Chaihuangshenquduguben” has good effects on severe patients with Cl2 poisoning , but the mechanism remains unclear.
The research group had been conducting research on the mechanism and treatment of choking agent poisoning [175-167]. The team discovered PTX, a drug that improves microvascular circulation, which could reverse the Cl2 induced ALI in rats through its anti-inflammatory and antioxidant effects [172]. In the early stage, our research group found that the oxidation damage reaction induced by Cl2 was improved after PTX intervention through in vivo and in vitro experiments. For example, raise GSH, GSH/GSSG and CAT, and reduce MDA and GSSG. It shows that the mitochondrial function of Cl2 damage could be repaired after PTX intervention. And the same effect had been verified in another choking agent phosgene induced lung injury.175 Recently, PTX was also used for ALI caused by COVID-19 [176-177], and it was found to have a good therapeutic effect in some clinical observation. All of these once again verified the improvement effect of PTX on ALI. PTX may be a potential drug candidate for Cl2 injury treatment.
Limitation
For literature inclusion, a scientific and comprehensive search and screening was carried out in this study. However, except for only a few randomized controlled trials, most of the literatures are case reports, and there may be some reporting bias.
Conclusion
In conclusion, this work systematically reviewed the Cl2 poisoning accidents that occurred worldwide in the past 55 years, analyzed and summarized the events characteristics and current status of diagnosis and treatment, and reported valuable research results. The treatment of traditional Chinese medicine and PTX, a methylxanthine derivative, in the treatment of Cl2 poisoning should be given more attention. It is hoped that the clinical application and laboratory research of drugs can provide help and reference for future research on Cl2 poisoning treatment strategies.
Declarations
Funding: The work was supported by grants from the project of Military Medical Innovation (16CXZ021).
Conflict of interest: The authors declare that they have no conflict of interest.
Author contributions: CQZ and QF designed/performed most of the investigation, data analysis and wrote the manuscript. MML contributed to interpretation of the data and analyses. CXH and XDZ was responsible for review design and manuscript revision.
References
- Mackie E, Svendsen E, Grant S, et al. Management of chlorine gas-related injuries from the Graniteville, South Carolina, train derailment. Disaster Med. Public Health Prep. 2014; 8: 411-416.
- Chen ML. A chlorine gas leak at an aquatics center in London, England. 2022.
- Zellner T, Eyer F. Choking agents and chlorine gas-History, pathophysiology, clinical effects and treatment. Toxicology letters. 2020; 320: 73-79.
- Achanta S, Jordt SE. Toxic effects of chlorine gas and potential treatments: a literature review. Toxicology mechanisms and methods. 2021; 31: 244-256.
- Radbel J, Laskin DL, Laskin JD. Disease-modifying treatment of chemical threat agent-induced acute lung injury. Ann N Y Acad Sci. 2020; 1480: 14-29.
- Jones R, Wills B, Kang C. Chlorine gas: an evolving hazardous material threat and unconventional weapon. The western journal of emergency medicine. 2010; 11: 151-156.
- Govier P, Coulson JM. Civilian exposure to chlorine gas: A systematic review. Toxicology letters. 2018; 293: 249-252.
- Adelson L, Kaufman J. Fatal chlorine poisoning: report of two cases with clinicopathologic correlation. American journal of clinical pathology. 1971; 56: 430-442.
- Agabiti N, Ancona C, Forastiere F, Di Napoli A, Lo Presti E, et al. Short term respiratory effects of acute exposure to chlorine due to a swimming pool accident. Occupational and environmental medicine. 2001; 58: 399-404.
- Babu RV, Cardenas V, Sharma, G. Acute respiratory distress syndrome from chlorine inhalation during a swimming pool accident: a case report and review of the literature. Journal of intensive care medicine. 2008; 23: 275-280.
- Barret L, J Faure. Chlorine poisoning. Lancet (London, England). 1984; 1: 321-322.
- Bellenger SR, Frizzi JD. Sevoflurane as a therapy for acute chlorine gas exposure in an austere healthcare environment: a case report. AANA journal. 2014; 82: 223-226.
- Bonetto G, Corradi M, Carraro S, Zanconato S, Alinovi R, et al. Longitudinal monitoring of lung injury in children after acute chlorine exposure in a swimming pool. American journal of respiratory and critical care medicine. 2006; 174: 545-549.
- Bonetto KH. Chlorine-induced damage documented by neurophysiological, neuropsychological, and pulmonary testing. Archives of environmental health. 2000; 55: 31-37.
- Bosse GM. Nebulized sodium bicarbonate in the treatment of chlorine gas inhalation. Journal of toxicology. Clinical toxicology. 1994; 32: 233-241.
- Bracco D, Dubois MJ, Bouali R. Intoxication by bleach ingestion. Journal canadien d’anesthesie. 2005; 52: 118-119.
- Moore BB, Sherman M. Chronic reactive airway disease following acute chlorine gas exposure in an asymptomatic atopic patient. Chest. 1991; 100: 855-856.
- Carpenter A, Cox AT, Marion D, et al. A case of a chlorine inhalation injury in an Ebola treatment unit. Journal of the Royal Army Medical Corps. 2016; 162: 229-231.
- Centers for Disease Control and Prevention (CDC) (2012). Chlorine gas release associated with employee language barrier--Arkansas. Morbidity and mortality weekly report. 2011; 61; 981-985.
- Charan NB, Lakshminarayan S, Myers GC, et al. Effects of accidental chlorine inhalation on pulmonary function. The Western journal of medicine. 1985; 143: 333-336.
- Chester EH, Gillespie DG, Krause FD. The prevalence of chronic obstructive pulmonary disease in chlorine gas workers. The American review of respiratory disease. 1969; 99: 365-373.
- Clark KA, Chanda D, Balte P, et al. Respiratory symptoms and lung function 8-10 months after community exposure to chlorine gas: a public health intervention and cross-sectional analysis. BMC public health. 2013; 13: 945.
- Courteau JP, Cushman R, Bouchard F, et al. Survey of construction workers repeatedly exposed to chlorine over a three to six month period in a pulpmill: I. Exposure and symptomatology. Occupational and environmental medicine. 1994; 51: 219-224.
- Van Sickle D, Wenck MA, Belflower A, Drociuk D, Ferdinands J, et al. Acute health effects after exposure to chlorine gas released after a train derailment. The American journal of emergency medicine. 2009; 27: 1-7.
- Duncan MA, Drociuk D, Belflower-Thomas A, Van Sickle D, Gibson JJ, et al. Follow-up assessment of health consequences after a chlorine release from a train derailment--Graniteville, SC, 2005. Journal of medical toxicology. 2011; 7: 85-91.
- Elsafti Elsaeidy AM, Alsaleh OI, van Berlaer G, Alhallak AA, Saeed SS, et al. Effects of Two Chlorine Gas Attacks on Hospital Admission and Clinical Outcomes in Kafr Zita, Syria. Cureus. 2021; 13: e17522.
- Endrizzi J, Nobay F, Wiegand T, Porter E. Bronchoscopic Findings Associated with Inhaled Chlorine Toxicity. The Journal of emergency medicine. 2015; 49: e123-e125.
- Bonetto G, Corradi M, Carraro S, Zanconato S, Alinovi R, et al. Longitudinal monitoring of lung injury in children after acute chlorine exposure in a swimming pool. American journal of respiratory and critical care medicine. 2006; 174: 545-549.
- Gentleman JF, Whitmore GA. Measurement of Possible Lung Damage to Firefighters at the Mississauga Train Derailment. Canadian journal of statistics. 1984; 12: 7-10.
- Güloğlu C, Kara IH, Erten PG. Acute accidental exposure to chlorine gas in the Southeast of Turkey: a study of 106 cases. Environmental research. 2002; 88: 89-93.
- Bonetto KH. Chlorine-induced damage documented by neurophysiological, neuropsychological, and pulmonary testing. Archives of environmental health. 2000; 55: 31-37.
- Hasan FM, Gehshan A, Fuleihan FJ. Resolution of pulmonary dysfunction following acute chlorine exposure. Archives of environmental health. 1983; 38: 76-80.
- Hung GU, Lin WY, Wang SJ. Increased pulmonary clearance of 99mTc DTPA aerosol. Semin Nucl Med. 2002; 32: 214-216.
- Fleta J, Calvo C, Zuñiga J, Castellano M, Bueno M. Intoxication of 76 children by chlorine gas. Human toxicology. 1986; 5: 99-100.
- Jones RN, Hughes JM, Glindmeyer H, Weill H. Lung function after acute chlorine exposure. The American review of respiratory disease. 1986; 134: 1190-1195.
- Jones FL. Chloride poisoning from mixing household cleaners. JAMA. 1972; 222: 1312.
- Jones R, Wills B, Kang C. Chlorine gas: an evolving hazardous material threat and unconventional weapon. The western journal of emergency medicine. 2010; 11: 151-156.
- Kaufman J, Burkons D. Clinical, roentgenologic, and physiologic effects of acute chlorine exposure. Archives of environmental health. 1971; 23: 29-34.
- Kennedy SM, Enarson DA, Janssen RG, Chan-Yeung M. Lung health consequences of reported accidental chlorine gas exposures among pulpmill workers. The American review of respiratory disease. 1991; 143: 74-79.
- Khilji MF. Clinical presentations and outcomes of industrial chlorine gas exposure incidence in Oman. Prehospital and disaster medicine. 2021; 36: 18-24.
- Kim JA, Yoon SY, Cho SY, Yu JH, Kim HS, et al. Acute health effects of accidental chlorine gas exposure. Annals of occupational and environmental medicine. 2014; 26: 29.
- Kose A, Kose B, Açikalin A, Gunay N, Yildirim C. Myocardial infarction, acute ischemic stroke, and hyperglycemia triggered by acute chlorine gas inhalation. The American journal of emergency medicine. 2009; 27: 1022.e1-1022.e10224.
- Kowitz TA, Reba RC, Parker RT, Spicer WS. Effects of chlorine gas upon respiratory function. Archives of environmental health. 1967; 14: 545-558.
- Lehavi O, Leiba A, Dahan Y, Schwartz D, Benin-Goren O, et al. Lessons learned from chlorine intoxications in swimming pools: the challenge of pediatric mass toxicological events. Prehospital and disaster medicine. 2008; 23: 90-95.
- Li BQ. Comparative study on chest imaging and clinical manifestations of acute chlorine poisoning. Chinese Journal of Critical Care Medicine. 2011; 31: 375-379.
- Li P. First aid and nursing of acute chlorine poisoning. Journal of Medical Forum. 2011; 29: 125-126.
- Li QA. Analysis of 56 cases of acute chlorine poisoning. People’s Military Surgeon. 2000; 5: 249.
- Levy DM, Tzabar Y. Whiter Than Whiteout. American Journal of Obstetrics and Gynecology.1993; 48: 91.
- Matos AM, Oliveira RR, Lippi MM, et al. Use of noninvasive ventilation in severe acute respiratory distress syndrome due to accidental chlorine inhalation: a case report. Revista Brasileira de terapia intensiva. 2017; 29: 105-110.
- Myers SJ. Chlorine inhalation in a pediatric patient. Journal of emergency nursing. 1997; 23: 583-585.
- Nishiguchi M, Takahashi M, Nushida H, Okudaira1 N, Nishio1 H, et al. An Autopsy Case of a Nonprescription Aspirin Overdose and Chlorine Gas Exposure. J Forensic Res. 2013; 4: 187.
- Ploysongsang Y, Beach BC, DiLisio RE. Pulmonary function changes after acute inhalation of chlorine gas. Southern medical journal. 1982; 75: 23-26.
- Schönhofer B, Voshaar T, Köhler D. Long-term lung sequelae following accidental chlorine gas exposure. Respiration; international review of thoracic diseases. 1996; 63: 155-159.
- Sexton JD, Pronchik DJ. Chlorine inhalation: the big picture. Clinical toxicology. 1998; 36: 87-93.
- Kowitz TA, Reba RC, Parker RT, et al. Effects of chlorine gas upon respiratory function. Archives of environmental health. 1967; 14: 545-558.
- Toland C. Treatment of a case of near-drowning in chlorinated fresh water. British journal of anaesthesia. 1972; 44: 616-619.
- VVajner J E, Lung D. Case files of the University of California San Francisco Medical Toxicology Fellowship: acute chlorine gas inhalation and the utility of nebulized sodium bicarbonate. Journal of medical toxicology. 2013; 9: 259-265.
- Warren B, Royall N, Smith H, Bhullar IS. Novel Treatment of Acute Respiratory Distress Syndrome after Chlorine Gas Inhalation Injury. The American surgeon. 2016; 82: e219-e220.
- Wood BR, Colombo JL, Benson BE. Chlorine inhalation toxicity from vapors generated by swimming pool chlorinator tablets. Pediatrics. 1987; 79: 427-430.
- Abhyankar A, Bhambure N, Kamath NN, Pajankar SP, Nabar ST, et al. Six month follow-up of fourteen victims with short-term exposure to chlorine gas. The Journal of the Society of Occupational Medicine. 1989; 39: 131-132.
- Bell DG. Severe lung injury following exposure to chlorine gas: A case series. Chest. 2007; 132: 566S-566S.
- Van Sickle D, Wenck MA, Belflower A, Drociuk D, Ferdinands J, et al. Acute health effects after exposure to chlorine gas released after a train derailment. The American journal of emergency medicine. 2009; 27: 1-7.
- Kilburn KH. Chlorine-induced damage documented by neurophysiological, neuropsychological, and pulmonary testing. Arch Environ Health. 2000; 55: 31-37.
- Chester EH, Kaimal J, Payne CB, Kohn PM. Pulmonary injury following exposure to chlorine gas. Possible beneficial effects of steroid treatment. Chest. 1977; 72: 247-250.
- Vohra R, Clark RF. Chlorine-related inhalation injury from a swimming pool disinfectant in a 9-year-old girl. Pediatric emergency care. 2006; 22: 254-257.
- Stopps GJ. Pneumonitis due to chemical irritants. JAMA. 1960; 173: 1762.
- Zhen JL, De JH, Zhong QW, Wang Z, Chang SH, et al. Radiographic and computed tomographic manifestations of chest in patients with acute chlorine gas poisoning. Chinese Medical Journal. 2010; 90: 2740-2744.
- Bai SL, Xie HX. Nursing experience of acute chlorine poisoning. ShandngMedicine. 2002; 35: 85-85.
- Cai LN. Treatment of acute toxic gas poisoning. Industrial Health and Occupational Diseases. 2012; 38: 314-315.
- Cai PQ, Zhu L. Clinical analysis of 8 cases of acute lung injury caused by toxic gas. Chinese Journal of Clinical Medicine. 2000; 7: 397-399.
- Cao XM. Clinical analysis of 82 cases of acute chlorine poisoning. Occupational Health and Emergency Rescue. 2000; 213-214.
- Chen, JY, Han XH, Gan HZ. Rescue and holistic nursing of 242 patients with acute chlorine poisoning. Modern Nurse. 2001; 33-34.
- Chen MQ, Chen Jk, Zhang WW, et al. Acute inhalation chlorine poisoning (report of 24 cases). Mil Med J Southeast Chin. 2007;117-118.
- Chen SF, Shi HP, Liu Y. Two cases of acute lung injury caused by irritant gas. Chin J Ind Hyg Occup Dis. 2006; 24: 62.
- Chen SB. Clinical analysis of 42 cases of acute chlorine inhalation. Anhui Med J. 1999; 47-48.
- Chen XJ, Qi XW. Clinical analysis of 423 cases of chlorine poisoning. Academiae Medicinae Suzhou. 1997; 17: 1189-1189.
- Chen Y. Rescue and nursing coordination of 39 cases of acute chlorine poisoning in children. Chinese Medicine of Factory and Mine. 1996; 9: 269-270.
- Chi LC, Duan ZJ, Jin S. Investigation report of a chlorine gas poisoning accident. Modern Preventive Medicine. 2003; 30: 65.
- Dai FL, Wei CL, Han J. Emergency treatment and nursing experience of 14 patients with acute chlorine poisoning. Tianjin Journal of Nursing. 2008; 16: 278-279.
- Diao XF, Sun SQ, Xu JX, et al. Salvage analysis of 11 cases of lung injury caused by chlorine gas explosion. The Medical Forum. 2007; 11: 374.
- Ding Y, Wang CM. Emergency management and nursing of 42 cases of chlorine poisoning. Journal of Clinical Medicine in Practice. 2005; 9: 50-51.
- Fan XJ, Zou JR, Li YH. Clinical analysis of 24 cases of chemical pulmonary edema. Clinical Focus. 2000; 15: 1020-1020.
- Feng JZ. Emergency nursing of patients with acute chlorine poisoning. Journal of Nursing science. 2002; 17: 660-661.
- Gao MQ. Report of 18 cases of acute chlorine poisoning. Jiangsu Medical Journal. 1995; 21: 99-99.
- Ge Sk, Wang NN, Zhao RX. Effect of short-range high-dose dexamethasone combined with anisodamine shock therapy on acute chlorine poisoning induced chemical lung injury. Guide of China Medicine. 2017; 15: 84.
- Geng XJ. Clinical analysis of acute irritant gas poisoning complicated with respiratory distress syndrome (ARDS) in 12 cases. Clinical Medicine. 1992; 12: 159-160.
- Guan YH, Z YL. Analysis of clinical characteristics of 46 cases of acute chlorine poisoning. Medical information. 2011; 24: 1288.
- Guo Y, Mei BR. Four cases of acute lung injury caused by swimming in swimming pool. Chinese Journal of Pediatrics. 2001; 39: 372-373.
- Hang TX. Observation and nursing care of 7 cases of chlorinepoisoning treated with Penehyclidine Hydrochloride. Journal of Clinical Medicine in Practice. 2010; 14: 31-32.
- He GW. Clinical analysis of 384 Cases of acute chlorine poisoning. China Journal of Modern Medicine. 1994; 4: 68-69.
- He HH, Li JP, Lian HQ. Rescue and nursing experience of patients with acute chlorine poisoning. Journal of Tropical Medicine. 2004; 3: 328-329.
- He XY. Clinical analysis of 14 cases of acute chlorine poisoning. Industrial Health and Occupational Diseases. 2003; 29: 307-308.
- He YJ. Analysis of 52 cases of chlorine leakage poisoning in pre hospital first aid. Chinese Journal of Trauma and Disability Medicine. 2013; 21: 291-292.
- Hong YQ, Wang LX. Clinical analysis of 22 cases of acute severe chlorine poisoning. Journal of Clinical Pulmonary Medicine. 2006; 11: 148-149.
- Hu CW, Zhang SL. Rescue and nursing of 25 cases of chlorine poisoning. Chinese Journal of Practical Nursing. 1992; 8: 20-21.
- Hu HZ. Emergency nursing experience of 93 cases of group acute chlorine poisoning. Medical Journal of the Chinese People’s Armed Police Forces. 2014; 25:1067-1069.
- Hu QX, Yu XM, Zhang HY. Nursing experience of hyperbaric oxygen treatment for sudden group chlorine poisoning. Zhejiang Medical Journal. 2014; 36: 2052-2053+2057.
- Hu WX. Lung damage caused by chlorine inhalation: a case report. Modern Medical Imagelogy. 1996; 5: 239-240.
- Hu ZP. Effect of chlorine on pulmonary ventilation function of workers. Occupation and Health. 2005; 21: 674-675.
- Li YS, Wang YL. X-ray findings of 50 cases of acute chlorine inhalation pneumonia. People’s Military Surgeon. 1991; 6: 58-59+86.
- Li ZM, Li L. Clinical analysis of 65 cases of chlorine poisoning. Chongqing Medicine. 2006; 21:1980-1981.
- Liang P, Cheng HA, Xie YP. Rescue and nursing of occupational acute chlorine poisoning. Occupation and Health. 2004; 5: 30-31.
- Liu GF, Zhao LF. Report of 62 cases of acute chlorine poisoning. Clinical Medicine. 1999; 11: 29-30.
- Liu JM. Treatment of 48 cases of chlorine inhalation poisoning. The Journal of Medical Theory and Practice. 2005; 2: 179-180.
- Liu XJ, Du YH. Rescue experience of acute chlorine poisoning. Journal of Modern Medicine & Health. 2006; 20: 3159.
- Liu XM. Clinical analysis of 127 cases of acute chlorine poisoning. Chinese Journal of Urban and Rural Industrial Hygiene. 2018; 33: 73-75.
- Liu YM. Nursing care of a child with severe chlorine poisoning. Proceeding of Clinical Medicine. 2006; 15: 59-60.
- Lu SH. Treatment of 12 cases of chlorine poisoning. Guide of China Medicine. 2011; 9: 130.
- Lu ZY. Rescuing a case of acute chlorine poisoning. Anhui Medical Journal. 2004; 4: 269.
- Lu J. First aid nursing of a large number of chlorine poisoning. Modern Journal of Integrated Traditional Chinese and Western Medicine. 2004; 19: 2116.
- Lu YH. Rescue and nursing of 17 cases of acute chlorine poisoning. Modern Rehabilitation. 1998; 2: 113-113.
- Ma XY. Acute pulmonary edema with myocardial damage caused by acute chlorine poisoning: a report of 5 cases. Practical Journal of Cardiac Cerebral Pneumal and Vascular Disease. 1995; 3: 44.
- Mao H. Chlorotoxic pulmonary edema: a report of 9 cases. Qinghai Medical Journal. 1995; 25: 50-51.
- Mei Z, Wu XW. Analysis of 58 cases of acute liquid chlorine poisoning. Negative. 2004; 16: 1463.
- Mu RA, He GWen. Treatment experience of 28 cases of acute severe chlorine poisoning. Hunan Medical Science.1994; 11: 305-306.
- Shao CZ. Rescue experience of acute chlorine poisoning. Occupational Health and Emergency Rescue. 1997; 4: 39.
- Shen GL. Treatment of acute chlorine inhalation injury in batches. Chinese Journal of Burns. 2004; 20: 52.
- Song S, Yao ZR. Scopolamine in rescuing a case of acute chlorine toxic shock. Zhejiang Medical Journal. 1982; 5: 16.
- Sun XD. Experience in the rescue of acute chlorine poisoning complicated with toxic pulmonary edema (clinical report of 13 cases). Qingdao Medical Journal. 1996; 3: 1-3.
- Wang JL.Treatment of acute chlorine poisoning in children. Journal of Applied Clinical Pediatrics. 1989; 1: 25-26.
- Wang CX. Nursing points of acute chlorine poisoning. Occupational Health and Emergency Rescue. 2005; 23: 163-163.
- Wang DQ, Lin J, Jiang JH. Investigation on health status of chlorine workers in a chemical enterprise. Strait Journal of Preventive Medicine. 2019; 25: 22-24.
- Wang J. Treatment of 22 cases of acute chlorine poisoning. Occupational Health and Emergency Rescue. 2007; 25: 280-283.
- Wang JY. First aid and nursing care of 83 cases of acute chlorine poisoning. Ningxia Medical Journal. 2004; 26: 250.
- Wang SX. Clinical analysis of 152 cases of acute chlorine poisoning. Protection & Occupational Safety and Health. 1985; 2: 21-23.
- Wang SQ. Nursing experience of mass chlorine poisoning. Chemical Industry Occupational Safety & Health. 1995; 6: 278-279.
- Wang WL, Ni WM. Report of 71 cases of acute chlorine poisoning. Chinese Journal of Industrial Medicine. 1991; 3: 37-38.
- Wang Y. Clinical nursing of 61 cases of acute chlorine poisoning. Journal of Qilu Nursing. 2010; 16: 84-85.
- Wang Y. Analysis of 31 cases of acute chlorine poisoning. Chinese Journal for Clinicians. 2000; 5: 31.
- Wei JJ. Therapeutic value of hyperbaric oxygen on acute chlorine toxic pulmonary edema. China Occupational Medicine. 1993; 2: 91.
- Wu LJ, Sun YX. Clinical analysis of 130 cases of acute chlorine poisoning. People’s Military Surgeon. 1980; 8: 44-46.
- Wu YY, Shan BR. Nursing experience of acute chlorine poisoning. Chinese Journal of Urban and Rural Industrial Hygiene. 2006; 4: 51.
- Xia XJ. Treatment of 10 cases of acute chlorine poisoning. Journal of Binzhou Medical University. 2012; 35: 461-462.
- Xian HH, Yu Li K. Clinical analysis of 21 cases of acute chlorine poisoning. Journal of Environmental and Occupational Medicine. 1985; 2: 41-42.
- Xiao BR. First aid and nursing care of 32 patients with group acute chlorine poisoning. For all Health. 2013; 7: 156.
- Xing XN. Treatment of toxic pulmonary edema caused by acute chlorine poisoning. Journal of Environmental. 2004; 0: 578-579.
- Xu L, Pu HY. First aid and nursing care of 6 patients with sudden chlorine poisoning. Jilin Medical Journal. 2011; 32: 400.
- Xue JL. First aid and nursing of acute chlorine poisoning. Occupation and Health. 1999; 8: 17-18.
- Yang J. Report of 4 cases of acute chlorine poisoning. Fujian Medical Journal. 1998; 1: 936-937.
- Yang L. Rescue and nursing of group chlorine inhalation. Chemical Industry Occupational Safety & Health. 1998; 4: 33-34.
- Yi MB, Chen GC, Zhang, et al. Hyperbaric oxygen in the treatment of 10 cases of acute chlorine poisoning. Chinese Journal of Nautical Medicine and Hyperbaric Medicine. 2006; 13: 146.
- Yin N. Rescue and nursing of patients with chlorine poisoning. Journal of Nurses Training. 2012; 27: 1916-1918.
- Yu, HN, Zhang, XQ, Zhang, WZ. Treatment of 58 cases of acute chlorine poisoning. Modern Medicine & Health. 2004; 24: 2693-2694.
- Yu SQ, Li F. Rescue experience of 24 cases of toxic pulmonary edema caused by chlorine poisoning. Journal of Internal Intensive Medicine. 2005; 11: 288-289.
- Yuan MQ, Shen YM. Emergency nursing of 80 patients with acute chlorine poisoning. Tianjin Journal of Nursing. 2001; 4: 173-174.
- Yue JM, Zhang XM. Emergency nursing of patients with acute chlorine poisoning. Practical Journal of Medicine & Pharmacy. 2014; 8: 740-742.
- Yue MX, Xia XY, Li Y. Clinical treatment of 1539 cases of sudden mass chlorine gas poisoning. Chinese Journal of Health Emergency Management. 2018; 4: 145-151.
- Zhang BL. Report of 5 cases of acute chlorine poisoning. Occupation and Health. 1988; 3: 47.
- Zhang J, Tang XD, Chen Q. Treatment experience of sudden mass acute chlorine poisoning. Medical Information Operations Sciences Fascicule. 2011; 24: 157-158.
- Zhang SF, Chi N, Wang YH. Treatment experience of sudden group acute chlorine poisoning. Guide of China Medicine. 2020; 7: 78-79.
- Zhang XF, Chen JB. A case report of acute chlorine poisoning. China Occupational Medicine. 1994; 1: 8.
- Zhang XY. Report of 14 cases of chlorine poisoning in children. Suzhou University Journal of Medical Science. 1997; 3: 435.
- Zhang YJ. Clinical observation on 36 cases of chlorine poisoning complicated with pulmonary edema treated by noninvasive mechanical ventilation. Chinese Journal of Critical Care Medicine. 2008; 28: 90-91.
- Zhao XJ. First aid and nursing of patients with chlorine poisoning. Healthmust Readmagazine. 2012; 11: 132-133.
- Zhi FC, Xue FW, Han LY. Observation of inflammatory index in patients with acute attack of chronic obstructive pulmonary disease after chlorine poisoning. Hubei J Tradit Chin Med. 2014; 36: 45-46.
- Zhou JJ. First aid and nursing care of 43 patients with acute chlorine poisoning. China Practical Medicine. 2013; 8: 192-193.
- Zhou XX. Clinical analysis of 20 cases of acute chlorine poisoning. Journal of Huaihai Medicine. 2004; 22: 307-308.
- Zhou XL. Treatment experience of group acute chlorine poisoning. Modern Medicine & Health. 2001; 12: 994-995.
- Zhou Y, Zhang H. First aid nursing of chlorine poisoning. Journal of Qiannan Medical College for Nationalities. 2000; 13: 46-47.
- Zhao HD, Bao XQ, Wang K. Extracorporeal membrane oxygenation combined with blood purification in the treatment of acute respiratory distress syndrome caused by chlorine inhalation: a case report. Chin J Ind Hyg Occup Dis. 2017; 35: 312-313.
- Zhen JL, De JH, Zhong QW. Radiographic and computed tomographic manifestations of chest in patients with acute chlorine gas poisoning. Chinese Medical Journal. 2010; 90: 2740-2744.
- Xu WM, Gao HM, Liu YC. Clinical analysis of 6 critically ill children with acute chlorine poisoning. Chinese journal of pediatrics. 2022; 60: 124-128.
- Xue JL. First aid and nursing of acute chlorine poisoning. Occupation and Health. 1999; 8: 17-18.
- Tseng CN. Hyperbaric oxygen therapy and nursing experience in chlorine poisoning. Modern Nurse. 2001; 31-32.
- Schwartz D A, Smith D D, Lakshminarayan S. The pulmonary sequelae associated with accidental inhalation of chlorine gas. Chest. 1990; 97: 820-825.
- Wigenstam E, Koch B, Bucht A. N-acetyl cysteine improves the effects of corticosteroids in a mouse model of chlorine-induced acute lung injury. Toxicology. 2015; 328: 40-47.
- Liu MM, Zhao CQ, Liu SS. Pentoxifylline protects against oxidative stress-mitochondria in experimental model of chlorine-induced acute lung injury in rats. Journal of Air Force Military University. 2022; 43: 1-13.
- Liu MM, Liu JZ, Zhao CQ. Protective effects of pentoxifylline against chlorine-induced acute lung injury in rats. Pharmacol Toxicol. 2023; 24: 12.
- Liu MM, Zhao CQ, Guo P. Protective effect of pentoxifylline on human umbilical vein endothelial cell injury induced by tert-butyl hydroperoxide. Journal of Air Force Military University. 2023; 1-11.
- Zhang XD, Zhao Y, Li WL. Protective effect of salidroside on chlorine-induced lung injury in rats. Journal of Preventive Medical Information. 2013; 29: 269-272.
- Zhang XD, Hai CX, Cai FL. Time course for expression of VEGF and its receptor and regulator levels of contraction and relaxation in increased vascular permeability of lung induced by phosgene. Inhalation toxicology. 2008; 20: 805-812.
- Liu MM, Li YW, Zhang XD. Chlorine inhalation-induced mitochondrial damage in rat pulmonary vascular endothelial cells and the interventional effect of salidroside. Carcinogenesis, Teratogenesis & Mutagenesis. 2018; 30: 31-3641.
- Liu MM, Kong DQ, Zhang XD. Protective effect of salidroside on pulmonary vascular permeability in acute lung injury induced by chlorine exposure. Carcinogenesis, Teratogenesis & Mutagenesis. 2016; 28: 377-382.
- Liu MM. Protective effects of salidroside and pentoxifylline on chlorine-induced ALI in rats. The Fourth Military Medical University. 2017; 1-88.
- Zhang XD, Hou JF, Hai CX. Pentoxifylline inhibits intercellular adhesion molecule-1 (ICAM-1) and lung injury in experimental phosgene-exposure rats. Inhalation toxicology. 2010; 22: 889-895.
- Feily A, Daneshpay K, Alighadr A. COVID-19: Pentoxifylline as a potential adjuvant treatment. International journal of clinical pharmacology and therapeutics. 2020; 58: 406-407.
- Monji F, Al-Mahmood Siddiquee A, Hashemian F. Can pentoxifylline and similar xanthine derivatives find a niche in COVID-19 therapeutic strategies? A ray of hope in the midst of the pandemic. European journal of pharmacology. 2020; 887: 173561.
