
Open Access, Volume 9
Large right heart thrombus caused by nuss bar displacement
Jian-You Huang1; Chun-Yu Chang1; Han-Yu Lin1,2*
1Department of Anesthesiology, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan.
2School of Medicine, Tzu Chi University, Hualien, Taiwan.
Han-Yu Lin
Department of Anesthesiology, Taipei Tzu Chi Hospital, 289, Jianguo Rd., Sindian District, New Taipei City 23142, Taiwan.
Tel: +886-2-66289779x2639;
Email: bbkeric@gmail.com
Received : March 31, 2023,
Accepted : May 05, 2023
Published : May 08, 2023,
Archived : www.jclinmedcasereports.com
Abstract
We reported a case of a 43-year-old woman with a funnel chest who presented with paroxysmal atrial fibrillation resulting from bar flipping after the Nuss procedure. During the Nuss bar removal surgery, a large floating right heart thrombus was detected on the intraoperative transesophageal echocardiography. Surgical thrombectomy was performed by the cardiac surgeon. During the operation, we found that her right heart was compressed by the dislocated bar, creating an adhesion band resulting in local constriction of the right cardiac chambers. Arrhythmia combined with local constriction and structural anomaly of the right heart could cause blood stasis and turbulent blood flow. The disturbed blood flow with low wall shear stress may modify endocardial endothelium structure and function of the right heart. According to Virchow’s venous thromboembolism triad, these changes are likely to be the mechanism underlying large intracardiac thrombosis. Thus, the surgical team must make every effort to prevent bar dislocation. It is also crucial for clinicians to familiar with echocardiographic skills for intracardiac thrombus identification. Although intracardiac thrombosis is a very rare complication after Nuss procedure, early diagnosis and aggressive management are of great importance because of its high mortality rate.
Keywords: Arrhythmia; Echocardiography; Intracardiac thrombosis; Nuss procedure; Pectus excavatum.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Lin HY (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Huang JY, Chang CY, Lin HY. Large right heart thrombus caused by nuss bar displacement. Open J Clin Med Case Rep. 2023; 2034.
Introduction
The Nuss procedure is a minimally invasive surgery for the correction of pectus excavatum. This procedure remodels the chest wall by employing one or more curved metal bars behind the sternum without resection of the costal cartilage [1]. Complications related to the Nuss procedure are not uncommon. Cardiac perforation is the most serious complication, and there are other complications, including major vascular trauma, pneumothorax, bar displacement, infection, pericardial effusion, and pleural effusion [2]. We describe a rare case of a Right Heart Thrombus (RHT) incidentally found on intraoperative Transesopha geal Echocardiography (TEE) in a patient undergoing bar removal surgery after a previous Nuss procedure.
Case Presentation
A 43-year-old woman presented with occasional chest discomfort since adolescence. She came to the outpatient clinic for medical consultation, where pectus excavatum was diagnosed (Haller index of 7.5 and sternovertebral distance of 6.2 cm), and the Nuss procedure was arranged by a thoracic surgeon. She had no known past medical history, and the cardiac workup did not reveal dysrhythmias or any structural abnormalities, including intracardiac thrombi. During the operation, two stainless steel bars were inserted and fixed with wire sutures, leaving the lower stabilizer (Figure 1A). Her postoperative clinical course was uneventful, so she was discharged on the eighth day after the surgery.
However, intermittent palpitations and chest discomfort occurred approximately one month after discharge. She was hospitalized again, and pertinent examinations revealed that she had paroxysmal atrial fibrillation. A cardiologist was consulted, and antiarrhythmic and anticoagulant medications were administered. After her symptoms subsided, she was discharged and followed up regularly in the outpatient clinic.
Two months later, her palpitations did not improve, and she also experienced chest discomfort, back pain, dyspnea, and even symptoms of heart failure. Under the suspicion of pectus bar displacement, she was hospitalized, and lower Nuss bar flipping was confirmed (Figure 1B). The patient was then referred for metal bar removal surgery. The operation was performed under general anesthesia, and hemorrhage from the surgical wound was noticed after removing the bars and wires. Because cardiac perforation was highly suspected, TEE examination was ordered. It revealed an intact cardiac surface, but a floating Right Atrial (RA) thrombus extending to the Right Ventricle (RV) and Right Ventricular Outflow Tract (RVOT) with moderate Tricuspid Regurgitation (TR) was incidentally found (Figures 2 and 3). Anticoagulant therapy with low-molecular-weight heparin was given postoperatively in the Surgical Intensive Care Unit (SICU). Coagulation workup did not reveal a hypercoagulable state. Computed tomography angiography did not find pulmonary embolism, and deep venous thrombosis was also excluded by compression ultrasound examination on deep veins of bilateral lower extremities. Because RHT remained a potential risk for serious thromboembolic events and needed to be addressed accordingly, further surgical management with open thrombectomy was scheduled three days after the last surgery.
During the operation, a severe band-like adhesion around the pericardial space was noticed, which resulted in a local constriction of the right heart [3]. Cardiotomy was performed following the initiation of cardiopulmonary bypass. On inspection, there was a large RA thrombus extending to the Tricuspid valve (TV), RV and RVOT, which was organized and easily fragmented and had broad-based attachments to the RA and RV free walls. After thrombectomy, TV perforation and RA defects were found, and TV replacement and bovine pericardial patch reconstruction were performed. Afterward, modified reconstruction of pectus excavatum, i.e., combined Ravitch and Nuss procedures, was performed by the thoracic surgeon (Figure 1C). The patient was then transferred to the SICU after the surgery. Her postoperative course was uneventful, and she was discharged one week after the last surgery.
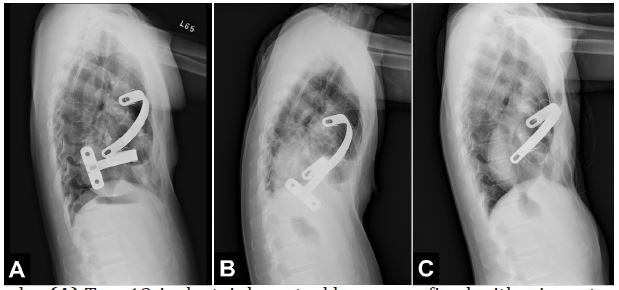
Figure 1: Lateral chest radiographs. (A) Two 13-inch stainless steel bars were fixed with wire sutures and left lower stabilizer on the first postoperative day. (B) Obvious upward flipping of the lower metal bar one month after the Nuss procedure. (C) Image after surgical thrombectomy, combined Ravitch and Nuss procedure with one supporting bar for pectus excavatum reconstruction, and tricuspid valve replacement.
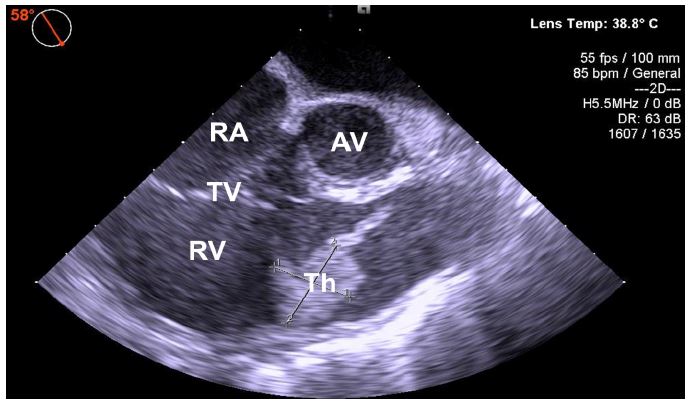
Figure 2: Transesophageal echocardiography image with a floating thrombus in the right atrium crossing into the right ventricle. Midesophageal RV inflow-outflow view at 58° showing the right ventricular portion of the clot of at least 2.30 × 1.95 cm.
AV: Aortic Valve; RV: Right Ventricle; Th: thrombus; TR: Tricuspid Regurgitation; TV: Tricuspid Valve.
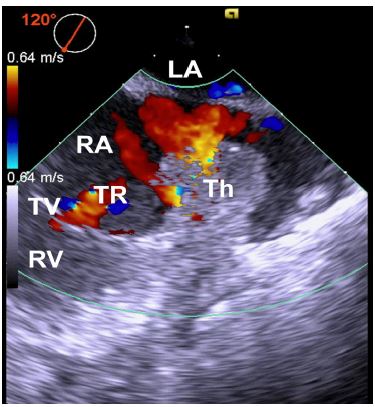
Figure 3: Midesophageal modified bicaval view of transesophageal echocardiography image at 120° with color flow Doppler showing the right atrial portion of the clot and moderate tricuspid regurgitation.
LA: Left Atrium; RA: Right Atrium; RV: Right Ventricle; Th: Thrombus; TR: Tricuspid Regurgitation; TV: Tricuspid Valve.
Discussion
Intracardiac thrombi may generate de novo in any cardiac chambers (type B) or form elsewhere in the body and be identified in the heart while in transit (type A) [4]. However, regardless of the etiology, the development of venous thrombosis mostly demonstrates components of Virchow’s triad: stasis of blood, endothelial injury, and a hypercoagulable state [5]. In our case, paroxysmal AF developed after the first Nuss procedure, which predisposes patients to atrial blood stasis and may lead to a subsequent procoagulant status. In addition, a band-like adhesion around the right pericardial space due to malposition of the metal bar could further bring about local constriction of the heart chamber and structural anomaly. This phenomenon may cause turbulent blood flow in the right heart with low wall shear forces, and it may modify the structure and function of the endocardial endothelium of the right heart [6]. These pathophysiological mechanisms potentially facilitate the development of large intracardiac thrombosis.
To our knowledge, this is the first case of thrombogenic cardiac abnormalities caused by bar displacement, eventually giving rise to a floating RHT formation. Thus, the surgical team must make every effort to reduce the occurrence of bar displacement, including the use of bar stabilizers, suturing, or wiring the pectus bar and stabilizers, as well as adding additional novel fixation devices. Moreover, because the mortality rate in patients with RHT is approximately 28%, early diagnosis and aggressive treatment are of great importance [7]. In this case, we use cardiovascular ultrasound to diagnose the RHT and to guide the surgical plan intraoperatively. It is crucial for clinicians to familiar with echocardiographic skills for intracardiac thrombus identification and measurement.
Declarations
Acknowledgments: We offer special thanks to Dr. Shih-Ching Wang and Yung-Chu Teng for their excellent assistance in writing and revising the draft of this manuscript. We are also express our gratitude to Prof. Yeung-Leung Cheng and Dr. Chan-Yang Hsu, who performed the surgery and cared for the patients in this study.
Author Contributions: All authors reviewed and approved the final manuscript.
Informed Consent: Written informed consent was obtained from the patient for the publication of this report.
Ethics approval statement: Ethical approval was waived by the Institutional Review Board of Taipei Tzu-Chi Hospital in view of the observational nature of the study.
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- Nuss D, Kelly RE, Croitoru DP, Katz ME. A 10-year review of a minimally invasive technique for the correction of pectus excavatum. J Pediatr Surg. 1998; 33: 545-552.
- Nuss D, Croitoru DP, Kelly RE, Goretsky MJ, Nuss KJ, Gustin TS. Review and discussion of the complications of minimally invasive pectus excavatum repair. Eur J Pediatr Surg. 2002; 12: 230-234.
- Hsu CY, Cheng YL, Wang SC, Shen TC. Massive right heart thrombus after the Nuss procedure: A case report. JTCVS Tech. 2022; 12: 69-71.
- The European Working Group on Echocardiography, Kronik G. The European Cooperative Study on the clinical significance of right heart thrombi. Eur Heart J. 1989; 10: 1046-1059.
- Egolum UO, Stover DG, Anthony R, Wasserman AM, Lenihan D, et al. Intracardiac thrombus: diagnosis, complications and management. Am J Med Sci. 2013; 345: 391-395.
- Chiu JJ, Chien S. Effects of disturbed flow on vascular endothelium: pathophysiological basis and clinical perspectives. Physiol Rev. 2011; 91: 327-387.
- Otoupalova E, Dalal B, Renard B. Right heart thrombus in transit: a series of two cases. Crit Ultrasound J. 2017; 9: 14.
