
Open Access, Volume 9
Endobronchial lipoma in a 62-year-old woman: A case report
Siming Meng
Department of Respiratory Critical Medicine, Yangpu Hospital of Tongji University, Shanghai, China.
Email: mengsiming1234@163.com
Received : March 26, 2023,
Accepted : May 03, 2023
Published : May 08, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Lipoma is a common soft tissue tumor, but lipoma in lung is rare. Here is an endobronchial lipoma that was occurred in a 62-year-old woman, and cured by Argon Plasma Coagulation (APC) via bronchoscope.
Lipoma is a common soft tissue tumor, but lipoma in lung is rare. Endobronchial lipoma consists of mature adipocytes, fibrous components and bronchial columnar epithelium [1]. Clinical manifestations include cough, recurrent pneumonia, hemoptysis and even intraluminal obstruction. Endobronchial lipoma often causes lung injury due to atelectasis and secondary lung abscess, so it needs lobectomy or endotracheal argon knife treatment. The diagnosis and treatment of an endobronchial lipoma patient treated by APC via bronchoscope is reported as follows:
Keywords: Bronchoscope; Lipoma; Argon plasma coagulation.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Meng S (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Meng S. Endobronchial lipoma in a 62-year-old woman: A case report. Open J Clin Med Case Rep. 2023; 2032.
Case Report
Clinical data: The patient is a 62-year-old woman from Shanghai, China. She was admitted to hospital with the chief complaint of “cough and shortness of breath for one week”. She had not suffered hemoptysis, fever, palpitation or chest pain. The patient was admitted to our department on January 31, 2020 after no remission from anti-infective treatment for 3 days. She had no smoking history, no harmful gas or dust exposure. In 2018, she received cervical cancer surgery in the external hospital.
Physical and laboratory examination: On her physical examination, she had minor shortness of breath and inspiratory phase wheezing rales were heard in left upper lung. Laboratory workup was remarkable for leukocytosis (11.1 cells × 109/l). Nothing abnormal detected in tumor markers including SCC antigen, neuron specific enolase, carbohydrate antigen (CA125, CA199, CA153). Both anti-neutrophil cytoplasmic antibody (P-ANCA MPO, PR3) and anti-glomerular basement membrane antibody GBM were negative. An enhanced computed tomography (CT) scan demonstrated a nodule with CT value of-100HU in left main trachea, and inflammation in left lower lobe (Figure 1).
In order to determine the nature of the left main bronchus nodule, bronchoscope was carried out on February 4, 2020. Under the microscope, it can be seen that a smooth, yellowish, pedunculated new biological occluded the bronchi (Figure 2).
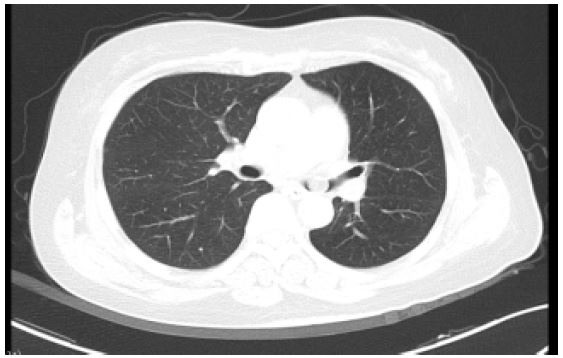
Figure 1: Chest Enhanced Scan showed Airway nodule in left main trachea (CT value - 100 HU).
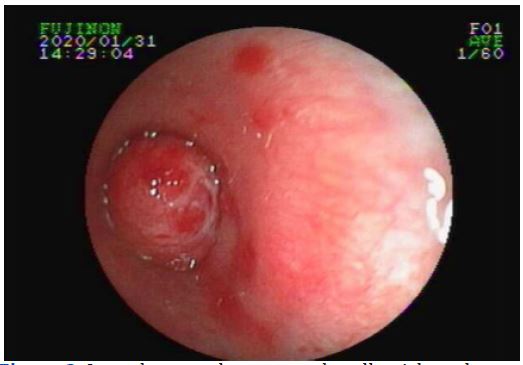
Figure 2: It can be seen that a smooth, yellowish, pedunculated new biological occluded the bronchi in bronchoscope.
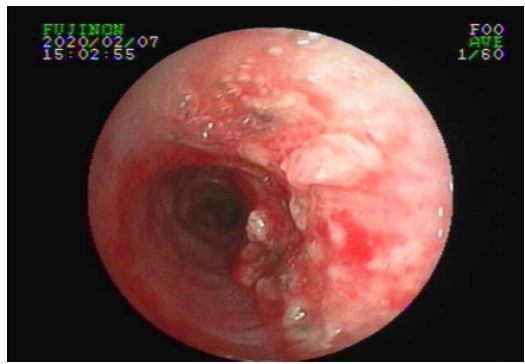
Figure 3: Reexamination of tracheoscopy indicated that the burn site of the original new organism was completely repaired.
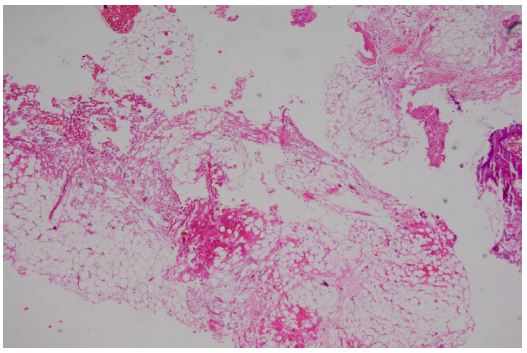
Figure 4: The biopathology examination showed the fibrous fat and a small amount of mucosal tissue. HE 40×.
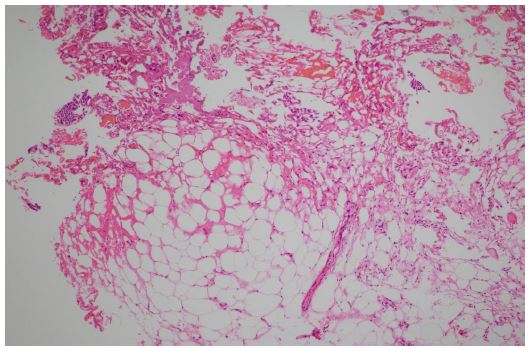
Figure 5: The biopathology examination showed the fibrous fat and a small amount of mucosal tissue. HE 100×.
The tumor was removed by argon plasma coagulation and biopsy forceps. On February 7, 2020, reexamination of bronchoscope indicated that the burn site of the original new organism was completely repaired (Figure 3).
The biopathology examination showed the fibrous fat and a small amount of mucosal tissue (Figure 4-5).
After the operation, the symptoms of shortness of breath and cough disappeared. Besides, there was no recurrence of cough symptoms in one month.
Discussion
Lipoma is the most common soft tissue lesion in pathology. The middle-aged patients are prone to this disease, but the incidence of lung disease is rare. The literature reports that this disease accounts for 0.1% - 0.5% of all lung tumors [2,3]. Smoking and obesity are important risk factors for tracheal lipoma [1]. In most cases, the polypoid lesions that block the bronchi originate from the fat cells located in the trunk or around the bronchi and under the mucosa. Under bronchoscope, lipoma is presented as round or oval soft mass with yellowish color, with or without pedicle, and covered with ciliated columnar epithelium [4].
There are no specificity in the clinical manifestations and imaging of the disease. The ability of airway ventilation compensation is strong, and there is no specificity in the early stage. Broncholipoma grows slowly in the lumen and has a large focus, which affects ventilation. Cough, wheezing and dyspnea when tired may occur [5]. The imaging manifestations are mostly obstructive pneumonia or atelectasis, and often misdiagnosed as chronic obstructive pulmonary disease or malignant lung tumor. CT scan and MRI are common tools for fat detection [6]. Lipoma in tracheobronchial presents fatty like hypo-dense shadow, and has no enhancement after strengthened scanning. Bronchoscopy can be used to locate the tumor, but it is difficult to diagnose the tumor by biopsy because of the solid capsule on the surface of the tumor. The chest CT of this case suggests that the left main airway and the basal segment of the left lower lobe should be differentiated from the recurrent respiratory papillomatosis (RRP). Respiratory papilloma is a benign tumor derived from epithelial cells on the surface of tracheal and bronchial mucosa, which is related to human papillomavirus (HPV) infection [7]. The patient had a history of cervical cancer, and the respiratory papilloma could not be excluded without pathological consideration. On February 4, 2020, when tracheoscopic biopsy was performed, it was difficult to clamp tissue due to the smooth mucosa of the tumor. The initial biopsy specimen showed chronic mucosal inflammation. Later, the pathology of the new clamped organism showed that there was a small amount of fibrous fat and mucosal tissue. The nucleic acid test results of human papilloma virus (HPV) were negative. A large amount of clear mucus was aspirated during the interventional treatment in the bronchi. On February 6, 2020, the chest CT reexamination results showed that the left main bronchus and inferior lobe nodules disappeared.
Bronchoscopic resection is considered the first choice for the treatment of broncholipoma. Compared with surgical resection, bronchoscopy is less invasive, which can save lung tissue and reduce incidence rate. Although Nassiri study points out that both rigid bronchoscope and soft fiberoptic bronchoscope are successfully used in clinic. But in the aspect of diagnosis, rigid bronchoscope has obvious advantages [8]. Bronchoscopic treatment is the first choice, and APC is a simple, economical and effective method. After complete resection, the recurrence rate of broncholipoma is very low, and almost no malignant change occur [9].
The identification and diagnosis of broncholipoma is challenging. This case suggests that the possibility of lipoma should be taken into account. Clinically, the less invasive treatment should be chosen to save the lung function of patients. Surgical lobectomy or pneumonectomy may be used if complicated airway diseases such as lung cancer occur.
References
- Muraoka M, Oka T, Akamine S, Nagayasu T, Iseki M, et al. Endobronchial lipoma: review of 64 cases reported in Japan. Chest. 2003; 123: 293-296.
- Jensen MS, Petersen AH. Bronchial lipoma. Scand Thorac Cardiovase Surg. 1970; 4: 131-134.
- Schraufnagel DE, Morin JE, Wang NS. Endobranchial lipoma. Chest. 1979; 75: 97-99.
- Cao D, Sun Y, Yang S. Endobronchial lipoma: an unusual cause of bronchial obstruction. Case Rep Med. 2011; 2011: 939808.
- Muraoka M, Oka T, Akamine S, Nagayasu T, Iseki M, et al. Endohronchiallipoma, review of 64 cases reported in Japan. Chest. 2003; 123: 293-296.
- Kim NR, Kim HJ, Kim JK, Han J. Intrapulmonary lipomas: report of four cases. Histopathology. 2003; 42: 305-306.
- Seedat RY, Combrinck CE, Burt FJ. HPV associated with recurrent respiratory papillomatosis. Future Virol. 2013; 8: 477-492.
- Nassiri AH, Dutau H, Breen D, Colchen A, Quiot JJ, et al. A multicenter retrospective study investigating the role of interventional bronchoscopic techniques in the management of endobronchial lipomas. Respir Int Rev Thorac Dis. 2008; 75: 79-84.
- Alazemi S, Majid A, Ruiz AI, Litmanovich D, Feller-Kopman D, Ernst A. An elderly woman with chronic dyspnea and endobronchial lesion. Chest. 2010; 137: 460-466.
