
Open Access, Volume 9
Contrast-enhanced computed tomographic evaluation of coeliac, hepatic and superior mesenteric arterial variants
Jovis Johny1; Arun George1; Shreyas Reddy K1*; Nidhi S1; Babu Philip1; Anna Rachel Menezes2
1Department of Radiology, St John’s Medical College Hospital, Bangalore, India.
2Department of Rural Medicine, St John’s Medical College Hospital, Bangalore, India.
Shreyas Reddy K
Department of Radiology, St John’s Medical College Hospital, Bangalore, India.
Email: Drshreyasreddy111295@gmail.com
Received : March 15, 2023,
Accepted : April 25, 2023
Published : April 27, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: With the advent of new hepato-biliary interventions, preoperative assessment of coeliac, hepatic, and mesenteric arterial anatomy has now become a necessity for surgeons and interventional radiologists. The primary aim is to avoid or minimize the ischemic complications that could occur during surgeries such as liver transplants, abdominal interventions etc. This study was undertaken to evaluate the variants in coeliac, hepatic, and superior mesenteric arteries based on the CECT abdomen.
Results: A prospective study was conducted over 2 years (2020-2021) on 388 patients who underwent CECT abdomen for evaluation of the above-mentioned variants. 14 types of CM trunk and 11 types of hepatic artery variants were identified in this study. Anatomical variations in CM trunk and CHA were seen in 6.4% and 7.7% respectively. The average diameter of the coeliac artery was found to be 6.6 mm, the common hepatic artery was 5.04 mm, and the superior mesenteric trunk was 6.6 mm.
In cases with variant coeliac -SMA axis, the average diameter of the coeliac trunk was 5.7 mm while the average arterial diameter of the hepatic artery in CHA variants was 4.38 mm.
The pathological variations found in the study were: MALS/ Dunbar syndrome, SMA compression syndrome, aortoarteritis and nutcracker syndrome.
A significant correlation was noted between the presence of CHA and coeliac -SMA axis variations i.e., the patients with CHA variation were 3.38 times more likely to have coeliac-mesenteric arterial variation.
The diameters of common hepatic and coeliac arteries were noted to be reduced in cases with anatomical variations (p < 0.05).
Conclusions: There is an association of coeliac-mesenteric artery variations with common hepatic arterial variations. Another correlation was found between the arterial diameters in cases with variant anatomy versus normal cases in the study population. No significant association between pathological variants like median arcuate ligament syndrome, SMA compression syndrome etc. with normal hepatic /CM trunk variations.
An attempt was also made to describe the newly found variations in these target vessels, not previously characterized in the standard classification system.
Keywords: MDCT; Coeliac trunk; Hepatic arteries; Superior mesenteric arteries; Arterial variations; Pre-operative imaging.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Shreyas RK (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Johny J, George A, Shreyas RK, Nidhi S, Philip B, et al. Contrast-enhanced computed tomographic evaluation ofcoeliac, hepatic and superior mesenteric arterial variants. Open J Clin Med Case Rep. 2023; 2028.
Background
Thorough knowledge of the coeliac, superior mesenteric, and inferior mesenteric arterial anatomy and its variants is vital for successful hepatobiliary surgery. Michel et al [1] were the first to propose a classification system for the anatomic variations in the Common Hepatic Artery (CHA) based on cadaveric dissection. Suzuki et al. were the first to perform an angiographic study on hepatic arterial variations in 200 patients [2].
The surgical relevance of the anatomy of the coeliac trunk, Superior Mesenteric Artery (SMA) & CHA is discussed in the following section:
Surgical relevance of CHA variant anatomy
Variations in hepatic arterial branching patterns create unexpected difficulties during the procedure, like trans arterial hepatic artery chemoembolization (TACE). Variants can lead to inadvertent complications like haemorrhage, improper catheter placements causing incomplete embolization of tumour or even lead to damage to the normal liver parenchyma during chemoembolization [3].
The accessory gastric arteries which can arise from the aberrant hepatic arteries should also be considered especially in the treatment of hepatic neoplasms with TACE, as they can lead to complications like gastric perforation. This is because complications like gastric wall ischemia can arise due to the obliteration of the accessory artery. In the liver, reconstruction of the arteries supplying the donor’s liver is required before the procedure to avoid complications like arterial thrombosis [4].
The variant anatomy can also be beneficial in some cases like in cases with replaced Right hepatic artery (RHA) which is beneficial for a donor due to its longer course, thus providing a larger graft and hence reducing complications like arterial thrombosis [5]. At the same time, this can pose a problem for the recipient’s liver as multiple vascular anastomoses are required between the donor and the recipient. Another added problem is the small calibre of the common hepatic artery which can lead to post-op complications [5,6].
In pancreatic surgeries e.g., pancreatic tumour resection or pancreaticoduodenectomy, the presence of an aberrant right hepatic artery can lead to intraoperative vascular damage as the artery courses near the pancreatic head (if its origin is from SMA) [7].
If the origin of the artery is from the Left Gastric Artery (LGA), vascular injury occurs while mobilizing the stomach. Knowledge of these variants helps the surgeon anticipate and manage the complications and determines the outcome of the surgery. An example is anticipating an anastomotic leak in a hepatobiliary surgery due to ischemia of the biliary anastomosis as the major blood supply to the extrahepatic biliary tree is from the aberrant right hepatic artery [4].
There can also be compression of the Common Hepatic Duct (CHD) leading to gallstone formation due to biliary stasis [8].
In Hiatal surgeries for gastroesophageal reflux disease, liver transplantation etc. there is an increased likelihood of injury to the aberrant left hepatic artery as it lies in the hepato gastric ligament which in turn can lead to left liver lobe ischemia [4]. Variant anatomy can also prove beneficial in cases where there is an occlusion in the porta because in such cases, the aberrant left hepatic artery provides the collateral circulation. The presence of an accessory right hepatic artery can also determine the course of progression of bile duct cancer. This is because, in classic cases, bile duct cancer usually spreads to the RHA due to its proximity. However, in patients with accessory hepatic arteries, these vessels are spared as they are further apart [9].
Knowledge of CHA variants is also important in pre-surgical planning of cholecystectomy to know the laparoscopic appearance of porta hepatis [10].
Thus, the knowledge of this variant anatomy imparts individualization of medical and surgical therapies.
Surgical relevance of Coeliac artery variant anatomy
The position of the coeliac trunk is of immense importance to an interventional radiologist as the vertebral level serves as a landmark for the localization of its orifice, for catheter insertion, especially in cases of upper GI bleed embolization. It is also relevant in the treatment of vascular complications like pseudo aneurysms in cases of liver trauma, pancreatitis, and leak from the pancreatic stump after a distal pancreatectomy or pancreatic leak following pancreatojejunostomy or pancreatogastrostomy. These procedures require selective embolization via coeliac trunk-hepatic artery catheterization, thus, in turn, emphasizing the knowledge of the relevant arterial variations [11].
Another situation where coeliac trunk anatomy is of importance is in the repair of thoracoabdominal aneurysms, either through open surgery or endovascular techniques using a stent prosthesis. The procedure requires cannulation of the coeliac trunk, which is then connected to an extracorporeal circulation device following which it is reimplanted in the graft, in open repair. The design of a vascular endoprosthesis for the repair of an aneurysm must consider the position of the coeliac artery and the arterial anatomy and course of its branches [12].
Surgical relevance of SMA variant anatomy
Among the SMA variations, one of the rare variations is the presence of a common coeliac-mesenteric trunk which occurs in < 1% of all abdominal vascular anomalies [incidence of 0.25%]. It occurs due to the regression of the tenth root and persistence of both the 13th root and anterior longitudinal anastomosis [13]. The presence of a variant like a common coeliac-mesenteric trunk will not have collateral circulation which in turn can affect the abdominal viscera (Foregut and midgut). This can also prove a problem during therapeutic management esp. during thrombolysis. Another vascular cause of upper abdominal angina is compression of the coeliac trunk by the diaphragmatic crura also known as median arcuate ligament syndrome or Dunbar syndrome. In patients with classical coeliac trunk anatomy, compression of the coeliac trunk alone would not present early. This is because there is a reformation of collaterals between the coeliac artery and SMA. However, in patients with a common CM trunk, compression of this vessel can cause decreased blood supply even to the mid-gut derivatives [5,14].
Methods
Source of data
The source of data for this study were the patients referred to the department of Radiodiagnosis and imaging, at John’s Medical College Hospital, Bangalore, for CECT abdomen. The study population was 482 patients for whom the CECT abdomen was done for various indications as a part of their diagnostic workup. 94 patients were excluded from the study population as they fulfilled the exclusion criteria. The study was performed, and data were analysed for the rest of the 388 patients who satisfied the inclusion criteria.
Methods
This was a prospective study conducted over two years (2020-2021) on patients who underwent CECT abdomen as a part of their diagnostic workup at the Department of Radiodiagnosis and Imaging. For the evaluation of coeliac, hepatic, and superior mesenteric arterial anatomy, CT was performed using a 128-slice GE Medical Systems Revolution EVO CT scanner.
The raw imaging data obtained was then processed on a workstation for multi-planar reformation (MPR) as well as the 3D reconstruction with maximum intensity projection (MIP) and volume rendering.
INCLUSION CRITERIA
· Patients above 18 years in whom contrast-enhanced CT abdomen was indicated.
EXCLUSION CRITERIA
· Patients in whom the CT evaluation was inadequate as a result of motion artefact/ improper breath-holding technique.
· Patients who underwent major abdominal surgeries and who had a history of vascular interventions involving the coeliac/SMA/hepatic arteries.
· Patients with lesions causing derangement of the target vascular structures (i.e., hepatic, coeliac and mesenteric axis)
· Patients with atherosclerotic calcifications involving the target vascular structures.
Image interpretation and statistical analysis
The coeliac trunk origin and the origin of its main branches namely the LGA, CHA and Splenic Artery (SA) as well as the origin of the SMA and its branches were identified and recorded for statistical analysis to calculate the prevalence of different variants. The variants of the coeliac trunk were classified according to Uflacker’s classification (Table 1) while the hepatic artery variants were classified depending on Michel’s classification (Table 2).
Table 1: Uflacker’s Classification of Coeliac Trunk Variation [15].
| Types | Variations |
|---|---|
| 1 | Normal trifurcation: classic type |
| 2 | Hepatosplenic trunk |
| 3 | Hepatogastric trunk |
| 4 | Hepato spleno mesenteric trunk |
| 5 | Gastrosplenic trunk |
| 6 | Common CM trunk |
| 7 | Coeliac-colic trunk |
| 8 | No coeliac trunk |
Table 2: Michel’s classification of coeliac trunk variation [1].
| Types | Variations |
|---|---|
| 1 | Hepato splenogastric trunk |
| 2 | Hepatosplenic trunk |
| 3 | Hepatosplenomesenteric trunk with LGA arising separately |
| 4 | Hepatogastric trunk with splenic artery arising from aorta / SMA. |
| 5 | Gastrosplenic trunk with CHA originating from aorta / SMA. |
| 6 | Common CM trunk |
| 7 | Coeliac- colic trunk with middle colic arising from the coeliac trunk |
The analysis data was done using IBM SPSS (Statistical Program for Social Science version 22.0, IBM Corp., USA). The analysis begins with descriptive analysis which includes methods such as pie diagrams, bar diagrams, histograms, and correlation. If the study data is collected from all members of the population, then these descriptive methods alone are sufficient for inferences. However, this scenario is impossible and estimation of population parameters using the sample population that was available for the study is needed.
Categorical variables were reported using numbers and percentages. Continuous variables were reported using mean +/- SD.
Comparison between variables was done by a chi-square test or Fisher’s exact test for categorical variables, and an Independent T test for continuous variables (parametric)/Mann-Whitney U test with post hoc Bonferroni correction for continuous variables (non-parametric). The data normality was assessed using histograms and probability plots. Q-Q plots were used to determine if the data were normally distributed.
To compare categorized characteristics of the study population between the two groups having CHA and coeliac mesenteric axis variations, univariate comparisons were made using the Chi-square test (more than five observations in all cells) or Fisher’s exact test (five or fewer observations in one or more cells). P values for all hypotheses tested were two-sided and statistical significance was set at P < 0.05.
Results
MDCT scans were interpreted for the following: Presence of normal arterial anatomy (involving coeliac-mesenteric axis and common hepatic artery). In the case of variant anatomy, details of origin, vascular course, and co-existence of other vascular variations and pathologies were described and analysed.
· Classification of aberrant arterial anatomy variants based on a standard system.
· Traditional classification for coeliac-mesenteric artery based on Uflacker’s classification.
· Traditional classification for CHA based on Michel’s classification.
· Separate classification of the newly found aberrant variants in both the common hepatic and CM arterial trunk.
The data collected were statistically analysed to calculate the frequency distribution of the variants. Analysis was also done to look for a correlation between CHA and coeliac mesenteric variants.
The sample characteristics are listed in Table 3 and Coeliac -mesenteric artery variations (Table 4).
Table 3: Sample characteristics.
| Mean age of the population | 49.3 years |
| Total no. of males with mean age (SD) | 191, 51 years (17.8) |
| Total no. of females with mean age (SD) | 197, 47 years (17.9) |
| Previous history of surgery | 19 |
| Cases with the presence of lesions causing derangement of the target vascular anatomy | 42 |
| Age group showing the maximum representation | 7th decade – 25.3 % percent |
Table 4: Frequency distribution of coeliac –mesenteric artery variations.
| COELIAC-MESENTERIC TRUNK VARIATION | UFLACKER’S CLASSIFICATION | Number of cases in our study |
|---|---|---|
| Classical coeliac trunk trifurcation | TYPE I | 363 |
| Hepatosplenic trunk | TYPE II | 1 (4 %) |
| Hepatogastric trunk | TYPE III | 1 (4 %) |
| Hepatospleno mesenteric trunk | TYPE IV | 1(4 %) |
| Gastrosplenic trunk | TYPE V | 5 (20 %) |
| CM trunk | TYPE VI | 0 |
| Coeliac- colic trunk | TYPE VII | 0 |
| No coeliac trunk | TYPE VIII | 1 (4 %) |
| gastroduodenal artery arising from the coeliac axis in addition to the 3 branches | NOD | 2 (8 %) |
| Left hepatic artery arising from the aorta and other branches of the coeliac artery together | NOD | 1 (4 %) |
| Right hepatic artery arising directly from the coeliac artery | NOD | 5 (20 %) |
| Left hepatic artery arising directly from the coeliac artery | NOD | 6 (24 %) |
| Right inferior phrenic arising from the coeliac axis | NOD | 2 (8 %) |
| TOTAL = 388 |
363 out of 388 cases showed a normal trifurcation pattern of the coeliac trunk (Uflacker I) representing 93.5 % of the total cases. Among the commonest anomalies among the coeliac, trunk variations were Type V Uflacker in the form of the gastro-splenic trunk with CHA arising from the aorta (most common anomaly) (Figure 1) representing 20 % of cases followed by Uflacker types II, III, IV & VIII (Figure 2) each type found in 4% of cases.
The variations not detected in this study population were Uflacker type VI and VII.
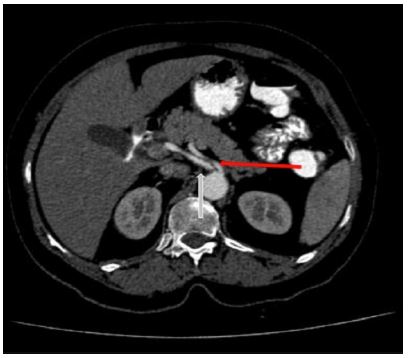
Figure 1: Axial CT cuts showing gastrosplenic trunk (red arrow) with CHA (white arrow) separately arising from the aorta.
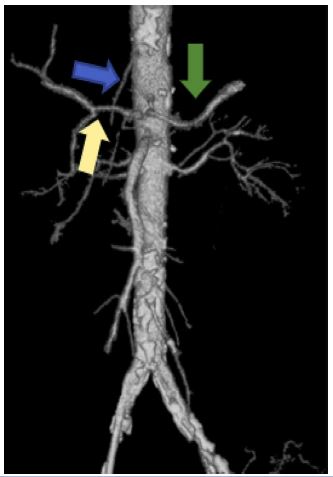
Figure 2: Volume-rendered image showing the separate origin of CHA (Yellow arrow), LGA (Blue arrow) & Splenic artery (Green arrow) from the aorta.
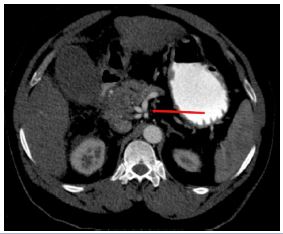
Figure 3: Axial CT section showing quadrifurcation of the coeliac trunk (red arrow) with gastroduodenal trunk arising from the coeliac axis.
A few other variations were found in the study population which were not previously classified. These accounted for 63% of the total arterial variants and were classified as “Not otherwise described”. These variations are the gastroduodenal artery originating from the coeliac axis (Figure 3), the origin of LHA from the aorta, and the origin of the LHA / RHA / right inferior phrenic artery from a coeliac artery. In this category, the commonest was the origin of LHA from the coeliac artery (20% of the cases).
CHA variations (Table 5)
The commonest anomalous hepatic artery variation was Michel type III variation i.e., replaced right hepatic artery originating from the superior mesenteric artery which was found among 63% of the cases.
This was followed by Michel type II found in 10% of cases. The variations not detected in this study population were type IV and Type X.
Variance in the origin of CHA was seen in 7 patients (origin of CHA from SMA in 2 and aorta in 5 patients). Normal origin of RHA from Hepatic Artery Proper (HAP) was seen in 361 patients. Replaced origin of RHA was seen in 63 % of total variants (commonest variant) while the accessory origin of RHA was seen in 1 (3.5%) case. Replaced LHA origin was seen in 3 (Figure 4) (10%) cases and accessory LHA origin in two (6.5%) cases.
In 2 cases (8%), the gastroduodenal artery was seen arising from the coeliac artery.
There were two cases of early bifurcation of the common hepatic artery (this was not classified as a variant as it followed the classical pattern of coeliac trifurcation).
In addition, one case showed the origin of the LHA from the aorta. (This was classified under the category of “Not otherwise described”: categorized under the coeliac-mesenteric axis variations).
Table 5: Frequency distribution of cha variations.
| HEPATIC ARTERY VARIATION | MICHELS’S | OUR STUDY |
|---|---|---|
| Normal anatomy | TYPE I | 358 |
| Replaced the left hepatic artery originating from the left gastric artery | TYPE II | 3 (10.00%) |
| Replaced right hepatic artery originating from the superior mesenteric artery | TYPE III | 19(63.33%) |
| Co-existence of Type II and III | TYPE IV | 0 |
| Accessory left hepatic artery originating from the left gastric artery | TYPE V | 2(6.7 %) |
| Accessory right hepatic artery originating from the superior mesenteric artery | TYPE VI | 1(3.33%) |
| The accessory left hepatic artery originates from the left gastric artery and the accessory right hepatic artery originates from the superior mesenteric artery (Figure 1a and 1b) | TYPE VII | 1(3.33%) |
| Accessory left hepatic artery originating from the left gastric artery and replaced right hepatic artery originating from the superior mesenteric artery | TYPE VIII | 1 (3.33%) |
| Common hepatic artery originating from the superior mesenteric artery | TYPE IX | 2 (6.7%) |
| Right and left hepatic arteries originating from the left gastric artery | TYPE X | 0 |
| Replaced left hepatic artery from left gastric along with accessory right hepatic artery from the superior mesenteric artery | NOD | 1 (3.33%) |
| TOTAL = 388 |
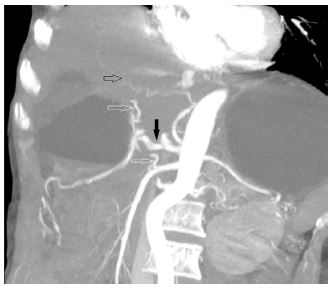
Figure 4: Oblique CT reformats showing replaced LHA (black open arrow) from LGA and accessory RHA (lower white open arrow) from SMA. The hepatic artery (Black arrow) and Right hepatic artery (Upper white open arrow) are also seen.
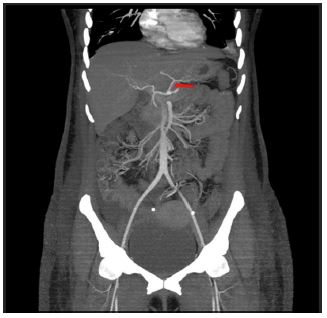
Figure 5: Coronal CT reformats showing the origin of LHA (red arrow) arising from LGA.

Figure 6: Coronal CT reformats showing the origin of RHA (red arrow) arising from SMA.
The latter two variants have often been described as “double hepatic arteries” [1].
The newly found hepatic artery variant (not described in the standard classification) was an accessory LHA (origin of LHA from LGA) along with the presence of an accessory right hepatic artery (origin of RHA from SMA) (Figures 5 and 6). This was seen in 3.5% of the total population.
Association between CHA anatomical variations and Coeliac-mesenteric axis variations.
Variations in both the coeliac-mesenteric axis and hepatic artery were found in 12.6% of the total study population.
The percentage of CHA variations having coeliac -mesenteric trunk variations was 16.7% while the percentage of common hepatic artery variations without coeliac -mesenteric trunk variations is 6.9%
Fischer’s exact T-test was performed to analyse the presence of any correlation between the coeliac-mesenteric axis and CHA variants.
The results showed a significant correlation (Fischer’s test statistic = 0.034) between the presence of CHA variants and coeliac mesenteric trunk variations (a < 0.05).
The odds ratio between the 2 variables (variation in common hepatic artery & CM arterial trunk) was 3.38 indicating that the patients having CHA variations were 3.38 times more likely to have coeliac-mesenteric arterial variation.
The 95% confidence interval for the above correlation was 1.17 (lower limit)- 9.764 (upper limit) indicating that there exists a similar representative population where the patients having CHA variations were 9.76 times more likely to have a coeliac-mesenteric artery variation (Upper limit is considered in this scenario).
Association between average diameters of Coeliac & Common hepatic artery with the presence of anatomical variations:
The next aim of the study was to determine if there existed a significant correlation between the coeliac artery diameter in cases with Uflacker’s type I coeliac artery as compared to the rest of the cases that had other coeliac artery variations.
This study also aimed to test a similar correlation between Michel’s type I hepatic artery and the rest of the CHA variants.
After assessment of the normality of the hepatic artery and coeliac artery using a Q-Q plot and histogram analysis, an independent T-test was used to determine the equality of means.
The average diameter of the coeliac artery was found to be 6.6 mm, CHA was 5.04 mm, and the superior mesenteric trunk was 6.6 mm.
In the case of CHA, the total number of cases with a classical pattern was 358 with the average diameter of CHA being 5.09 mm.
The total number of cases with variant CHA anatomy was 30, and in these cases, the CHA had a mean diameter of 4.38 mm. The mean difference between the arterial diameters while comparing both the groups (ie. Type I vs rest of the CHA variations) was 0.71 mm with a significance of 0.003 (Level of significance for the study: p < 0.05).
In the case of the coeliac artery, the total number of cases with a classical pattern was 363 with the average diameter being 6.72 mm. The total number of cases with variant anatomy was 25, with a mean diameter of 5.7 mm.
The mean difference between the arterial diameters while comparing both the study populations was 1.02 mm with a p-value of 0.001 (Level of significance for the study: p < 0.05).
In both scenarios, there exists a significant reduction in the average vessel diameters in CHA and coeliac trunk in patients with anatomical variations
Various vascular pathologies were noted as associated findings in this study (Table 6).
E.g., MALS i.e., Median arcuate ligament syndrome (Dunbar syndrome). The median arcuate ligament is a fibrous arch uniting the diaphragmatic crura at the level of the aortic hiatus and passes superior to the coeliac artery origin. However, if the insertion is low, it can cause abdominal pain. The diagnosis of coeliac axis compression / median arcuate ligament syndrome / Dunbar syndrome is done with conventional angiography/ CT angiography. The CECT imaging findings are characteristic focal narrowing in the proximal coeliac axis with a characteristic juxta-ostial hooked appearance with coeliac artery origin stenosis (Figure 7)[2].
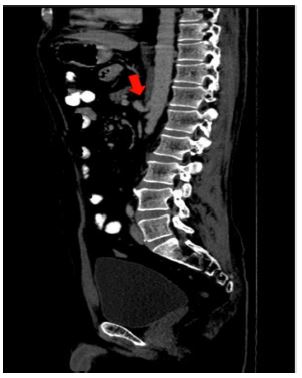
Figure 7: Sagittal CT reformats showing juxta ostial fishhook configuration of the coeliac artery with narrowing of the coeliac artery near the origin (Red arrow).

Figure 8: Sagittal reformats of a patient with anterior nutcracker syndrome showing the compression of the left renal vein. (Blue arrow).
Table 6: Frequency Analysis of Vascular Pathologies Involving Coeliac -Mesenteric Arterial Axis.
| PATHOLOGICAL CASES | FREQUENCY OF VARIANTS |
|---|---|
| Dunbar syndrome | 5 |
| Nutcracker syndrome | 2 |
| SMA compression syndrome | 1 |
| Vasculitis | 2 |
The other pathology found in this study was SMA compression syndrome which is also known as Willkie’s syndrome/Cast syndrome. In this pathology, there is a reduced aortomesenteric angle and distance between the vessels which in turn causes compression of the third part of the duodenum.
The normal aortomesenteric angle is 45 degrees (normal range: 25° to 60°). However, in patients with significant loss of mesenteric fat, the aortomesenteric angle becomes acute (< 22°) causing compression of the third part of the duodenum, thus causing resulting in SMA syndrome [3].
Nutcracker syndrome was another pathology found in this study which is the compression of the Left Renal Vein (LRV) between the aorta and (SMA). This condition is called “anterior nutcracker syndrome” (Figure 8). In contrast, a circumaortic or retro aortic LRV can also be compressed between the aorta and vertebral body, which is called the “posterior nutcracker syndrome”. One of the many causes of anterior nutcracker syndrome is aberrant SMA branching from the aorta. The patient may present as a case of pelvic congestion syndrome secondary to renal venous hypertension. The imaging findings are the presence of the beak sign (i.e., abrupt narrowing of the LRV between the aorta and SMA) with concomitant dilatation of the proximal LRV. Another CT parameter is a ratio of the LRV diameters at the hilar and aortomesenteric regions of more than 4.9. A few other findings include a reduced aortomesenteric angle (less than 41°) which is a very sensitive parameter /a measured beak angle of more than 32° [4].
Association of pathological variations with anatomical variations
In 6.1 % of cases with anatomical variants in either coeliac-mesenteric axis variant/CHA variants or both, there were pathological variants like Dunbar/SMA compression/nutcracker syndrome.
Fischer’s exact T-test was also done to look for a correlation between anatomical variants and pathological conditions related to the coeliac mesenteric axis.
Fischer’s test statistic was not significant for this association with the test statistic value of 0.092.
Discussion
Digital subtraction angiography (DSA) is the gold standard in the evaluation of vascular structures esp. the presence of arterial variations. However, it is invasive and is associated with iatrogenic risks and complications [16].
These disadvantages are overcome by using CECT images for the vascular structures, which can be obtained in a high spatial and temporal resolution in a short period and is also noninvasive. In addition, reformats of the images can be done in coronal and sagittal planes and the post-processing allows us to view only the vascular structures using minimum-intensity projections. 3-D reconstruction can also be performed for viewing small vessels. On account of these advantages, it has replaced conventional angiography in the assessment of the vascular structures for pre-operative evaluation of the hepatic vasculature [17].
Classification of coeliac artery variations based on its branching pattern has been performed by several studies, the first one done by Lipschulz in 1917 [18] and the most recent by Uflacker in 1997 (described in table 2) [19].
The classical coeliac anatomy is the type I variant which occurs at a frequency of 51-80%. Separate origin of the CHA, splenic artery, and LGA from the CA occurs in 10-19% of cases while in 10%, a quadrifurcating/pentafurcating CA is noted with the dorsal pancreatic artery, GDA, and right and left hepatic arteries originating directly from the trunk [20].
In the context of the Indian population, a similar study i.e., MDCT evaluation of coeliac and common hepatic variations) was undertaken by Thangarajah et al in the south Indian population. In comparison to the current study, no correlative analysis was performed in mentioned study [21].
In almost all the studies Uflacker type I (the normal trifurcation pattern of the coeliac artery) is the commonest variant which is consistent with our study. The incidence of Uflacker type I in this group was 93.5 % [17] which is similar to the results of the studies done by Song et al [16] and Ugurel et al [22].
With regards to the variants (according to the Uflacker’s classification), the commonest was Uflacker type V with gastro-splenic trunk and anomalies origin of the CHA from the aorta/SMA representing 20% and this is relatively higher as compared to Ugurel et al [22].
However, the results in this study were contradictory to studies done by Lipschutz et al [18], and Thangarajah et al [21], who found that Uflacker type II was the commonest variant. In the study by Thangarajah et al, the next common variant was the presence of a hepato-mesenteric trunk and a separate gastrosplenic trunk [21].
In this study, the non-classified variations accounted for the major bulk of the anatomical CM axis variants accounting for 63 % of the total cases. The commonest variation among the non-classified variations was the origin of the left or right hepatic artery from the coeliac axis.
Variant arterial anatomy in the common hepatic artery is noted in approx. 25-30% of the population.
The incidence of aberrant right hepatics as reported in other studies was 11-26% of which replaced right hepatic arteries were seen in 3.5-21% of cases and accessory right hepatic arteries in 1-8% of cases [3].
The incidence of aberrant left hepatics as observed in other studies was 12.5-32% with accessory left hepatic arteries in 4.5-32% of cases and replaced left hepatic arteries in 4-15.5% of cases [23].
With regards to the hepatic artery variations, this study showed that Michel type I is the commonest type (classical type I) with an incidence of about 92.3% which is slightly higher than the prevalence of these variants in the normal population (51-80%) as reported by Kamel et al [24]. With regards to the anomalous arterial variants, this study showed that Type III was the commonest anomaly with replaced RHA from the SMA representing about 63% of the total cases and these results are consistent with studies conducted by Koops et al and De Cecco et al with variable incidences [25,26].
However, in studies by Covey, Thangarajah and Coskun et al Michel type V was the commonest variant in their study group [3,21,26].
In this study, a new hepatic artery variant was found which has not been previously described. This variant was a replaced left hepatic artery from the left gastric along with an accessory right hepatic artery from the superior mesenteric artery which was classified as not otherwise described.
By the above-mentioned findings, this study has added 5 newly found variations to the one found by Uflacker i.e., the origin of gastroduodenal artery from the coeliac artery, the origin of left hepatic artery from the aorta and other branches of coeliac artery together, the separate origin of a right hepatic artery directly from the coeliac artery, the separate origin of left hepatic artery from coeliac artery and aberrant origin of right inferior phrenic arising from the coeliac axis. These variants were grouped into a category not otherwise described (Type IX).
A cadaveric study was done by Silveira et al in which the arterial diameters were compared between the groups which had normal anatomy and those that had anatomical variants. This study showed smaller diameters for variable vessels; however, the difference was not significant [7].
In comparison, this study has a significant reduction in the coeliac artery diameter in the presence of anatomical variations. This finding can be of significance while selecting patients for liver transplantation.
A significant correlation between arterial diameter in patient groups with normal anatomy and group with common hepatic artery variations has also been established.
After an extensive literature review, there was no mention of a previous study for the analysis of the above-mentioned objectives.
However, in both the above scenarios (i.e., Association of arterial diameters with an anatomical variation of common hepatic and coeliac-mesenteric trunk), the correlation between the individual variants with the arterial diameters could not be performed as the frequency of these individual variants are less and because of the relatively smaller size of the study population. However, this is a possibility with a larger study population.
One of the ancillary findings in the study was the presence of bilateral accessory renal arteries (anatomical variant) in 3 cases with replaced right hepatic arteries.
A study by Ugurel et al showed a significant correlation between anatomical variants in the renal artery and coeliac trunk-hepatic arterial system variations [22]. This association was however not explored in this study.
Regarding pathological variations, no significant correlation was seen between the anatomical and pathological cases in this study.
However, previously a case report was published proposing an association between median arcuate ligament syndrome and the presence of a CM trunk (Uflacker’s type VI variation) [27].
A similar theory was also proposed by Loukas et al which stated that the presence of a single trunk was one of the possible causes of MALS [28].
The other pathology found in this study was SMA compression syndrome which is stated to have a prevalence of 0.1 -0.3%. The normal SMA -aortic angle is between 25-60 degrees with an average of 45 degrees. In SMA compression syndrome, the CT criteria are the aortomesenteric angle of fewer than 22 degrees with a reduced aorto-mesenteric distance of 8-10 mm. There is also compression of the 3rd segment of the duodenum with proximal dilatation of the stomach and the 1st/the 2nd parts of the duodenum. The congenital variance in the SMA origin was touted as one of the factors causing SMA compression syndrome [29].
In this study, no coeliac-mesenteric trunk anatomical variants were noted in the cases with SMA compression syndrome.
No prior study was found exploring the correlation between aorto mesenteric angle and variants. This was attempted in this study; however, no significant correlation was found.
Conclusive evidence of the same can only be provided by testing the association in a larger population.
Study limitations
In the context of the association of arterial diameters with an anatomical variation of common hepatic and coeliac-mesenteric trunk, the correlation between the individual variants with the arterial diameters could not be performed as the frequency of these individual variants was less.
Conclusions
Analysis and characterization of the coeliac-mesenteric trunk and hepatic artery variants are important as a part of pre-interventional/pre-surgical workup to decrease the post-surgical complications and morbidity rates. MDCT is a non-invasive modality which is quite efficacious in diagnosing these variants in comparison to the conventional modality of DSA.
The current study comprised 388 patients evaluated by CECT (Revolution Evo 128 slice helical CT, GE medical systems) at the Department of Radiodiagnosis and Imaging, St. John’s Medical College Hospital, Bangalore.
CECT was assessed for the presence of anatomical variations in coeliac, mesenteric, and common hepatic arteries and a comparison of this study with the standard classification proposed in the literature.
The assessment also included the presence of vascular pathologies in these arteries, evaluation of arterial diameters, aorto-mesenteric arteries, and other associated pathologies.
The influence of age and sex in the distribution of the target arterial variant anatomy was investigated. A female predominance was seen, as was the predominance involving the seventh decade of life. Both CHA & CM arterial variations were seen predominantly in males. The classic pattern was the most common variation found in the majority of the subjects. Among the variants, Uflacker’s classification Type V and Michel’s classification Type III were the most common types.
In contrast to a few other previous studies, which showed a higher incidence of type II variation, this study had a higher incidence of type V coeliac axis variation. Coming to CHA variants, the type III variant was the commonest which was comparable to previous studies in the literature.
This study also found a significant association between smaller arterial diameters and the presence of variant anatomy. Another significant correlation found in the study was the linear relationship between CHA variants and coeliac-mesenteric variants. Associated findings like the presence of vascular pathologies like coeliac/SMA compression syndrome, MALS etc were also analysed.
Overall, MDCT acts as an effective imaging modality in the evaluation and characterization of anatomical variations of coeliac/mesenteric artery & common hepatic artery and their associated findings. Such evaluation helps not only in deciding the future course of management. But also, in reducing the associated mortality and morbidity, thus becoming vital to patient care.
Declarations
Ethics approval and consent to participate
Waiver of consent was obtained by the Institutional ethics committee, St. John’s Medical College for the below-stated reasons –
1) Research involves ‘not more than minimal risk’.
2) There is no direct contact between the researcher and the participant.
3) The patient’s name and other identifiable details are not shared with a third party.
4) This study is akin to a record review study.
5) The identifying details of the patient are not utilized in the study.
Consent for publication:Not applicable.
Availability of materials and data: The datasets generated in the current study are available and can be accessed on request from the corresponding author.
Competing Interests: The authors have no relevant financial or non-financial interests to disclose.
Funding: No funding was obtained for the conduction and publication of this study.
Acknowledgements: We would like to express our thanks and gratitude to the Department of Radiology, St. John’s medical college for their everlasting support.
References
- Michels NA: Newer anatomy of the liver and its variant blood supply and collateral circulation. Am J Surg. 1966; 112: 337-347.
- Sureka B, Mittal MK, Mittal A, Sinha M, Bhambri NK, et al. Variations of celiac axis, common hepatic artery and its branches in 600 patients. Indian J Radiol Imaging. 2013; 23: 223-33.
- Covey AM, Brody LA, Maluccio MA, Getrajdman GI, Brown KT. Variant Hepatic Arterial Anatomy Revisited: Digital Subtraction Angiography Performed in 600 Patients. Radiology. 2002; 224: 542-547.
- Kavitha Kamath B. A STUDY OF VARIANT HEPATIC ARTERIAL ANATOMY AND ITS RELEVANCE IN CURRENT SURGICAL PRACTICE: Int J Anat Res. 2015; 3: 947-953.
- Chaib E, de Souza YE, Maruyama MY, Marinucci LFB, Aranha MR, et al. Left hepatic artery arising from the superior mesenteric artery: a case study of a rare anatomic variation. The. Open Anatomy Journal. 2010; 14: 2.
- López-Andújar R, Moya A, Montalvá E, et al. Lessons learned from anatomic variants of the hepatic artery in 1,081 transplanted livers. Liver Transplant Off Publ Am Assoc Study Liver Dis Int Liver Transplant Soc. 2007; 13: 1401-1404.
- Mugunthan N, Jansirani D, Felicia C, Anbalagan J. Anatomical variations in the arterial supply of liver. International Journal of Anatomical Variations. 2012; 5: 107-109.
- Mendes VM, Nasser HA, Bou Nassif G, Choukr A. Prebiliary right hepatic artery resulting in common hepatic duct compression and subsequent intrahepatic stone formation: myth or reality?. Case Reports in Medicine. 2014; 12014.
- Standring S, editor: Gray’s anatomy e-book: the anatomical basis of clinical practice. Elsevier Health Sciences.2021.
- Hiatt JR, Gabbay J, Busuttil RW: Surgical anatomy of the hepatic arteries in 1000 cases. Annals of surgery. 1994; 220: 50.
- Yi SQ, Terayama H, Naito M, Hirai S, Alimujang S, et al. Absence of the celiac trunk: case report and review of the literature. Clinical Anatomy: The Official Journal of the American Association of Clinical Anatomists and the British Association of Clinical Anatomists. 2008, 21: 283-286.
- Panagouli E, Venieratos D, Lolis E, Skandalakis P. Variations in the anatomy of the celiac trunk: A systematic review and clinical implications. Ann Anat - Anat Anz. 2013; 195: 501-511.
- Aramaki O, Sugawara Y, Kokudo N, Takayama T, Makuuchi M. Branch patch reconstruction in living donor liver transplantation: arterialization of grafts with replaced type arteries. Transplantation. 2006; 15: 1541-1543.
- Saeed M, Rufai AA. Duplication of hepatic artery. Saudi Journal of Gastroenterology. 20011; 7: 103.
- Uflacker R, editor: Atlas of vascular anatomy: an angiographic approach. Lippincott Williams & Wilkins, 2007.
- Song SY, Chung JW, Yin YH, et al.: Celiac axis and common hepatic artery variations in 5002 patients: systematic analysis with spiral CT and DSA. Radiology. 2010; 255: 278-288.
- Winter TC, Nghiem HV, Freeny PC, Hommeyer SC, Mack LA. Hepatic arterial anatomy: demonstration of normal supply and vascular variants with three-dimensional CT angiography. Radiogr Rev Publ Radiol Soc N Am Inc. 1995; 15: 771:80.
- Lipshutz B. A COMPOSITE STUDY OF THE COELIAC AXIS ARTERY. Ann Surg. 1917; 65: 159-169.
- Uflacker R. Atlas of vascular anatomy: an angiographic approach. Veins of the head and neck, veins of the thorax. 1997.
- White RD, Weir-McCall JR, Sullivan CM, et al. The celiac axis revisited: anatomic variants, pathologic features, and implications for modern endovascular management. Radiogr Rev Publ Radiol Soc N Am Inc. 2015; 35: 879-898.
- Thangarajah A, Parthasarathy R: Celiac Axis, Common Hepatic and Hepatic Artery Variants as Evidenced on MDCT Angiography in South Indian Population. J Clin Diagn Res JCDR. 2016; 10: 01-05.
- Ugurel MS, Battal B, Bozlar U, et al. Anatomical variations of hepatic arterial system, coeliac trunk and renal arteries: an analysis with multidetector CT angiography. Br J Radiol. 2010; 83: 661-667.
- Suzuki T, Nakayasu A, Kawabe K, Takeda H, Honjo I. Surgical significance of anatomic variations of the hepatic artery. Am J Surg. 1971; 122: 505-512.
- Kamel IR, Kruskal JB, Pomfret EA, Keogan MT, Warmbrand G, et al. Impact of multidetector CT on donor selection and surgical planning before living adult right lobe liver transplantation. AJR Am J Roentgenol. 2001; 176: 193-200.
- Koops A, Wojciechowski B, Broering DC, Adam G, Krupski-Berdien G: Anatomic variations of the hepatic arteries in 604 selective celiac and superior mesenteric angiographies. Surg Radiol Anat SRA. 2004; 26: 239-244.
- De Cecco CN, Ferrari R, Rengo M, Paolantonio P, Vecchietti F, Laghi A: Anatomic variations of the hepatic arteries in 250 patients studied with 64-row CT angiography. Eur Radiol. 2009; 19: 2765-2770.
- Chaiwatcharayut W, Lekah A, Kurklinsky A.Celiacomesenteric Trunk as a Cause of Median Arcuate Ligament Syndrome. J Med Ultrasound. 2013; 21: 39-42.
- Loukas M, Pinyard J, Vaid S, Kinsella C, Tariq A, Tubbs RS: Clinical anatomy of celiac artery compression syndrome: a review. Clin Anat N Y N. 2007; 20: 612-617.
- Bhagirath Desai A, Sandeep Shah D, Jagat Bhatt C, Umesh Vaishnav K, Salvi B. Measurement of the Distance and Angle Between the Aorta and Superior Mesenteric Artery on CT Scan: Values in Indian Population in Different BMI Categories. Indian J Surg. 2015; 77: 614-617.
