
Open Access, Volume 9
A case of an adult complicated left diaphragmatic hernia: Case report and literature review
Ribal Aby Hadeer
General Surgery, Mount Lebanon Hospital Balamand University Medical Center, Beirut, Lebanon.
Email: Ribal_hadeer@hotmail.com
Received : March 20, 2023,
Accepted : April 24, 2023
Published : April 27, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Diaphragmatic hernia by definition is the protrusion of abdominal structures into the thoracic cavity. Classified as either congenital or acquired, adult diaphragmatic hernia without a history of trauma is rare, and iatrogenic diaphragmatic hernia is rarer. The array of symptoms may be acute or latent and will depend on the herniated organ, which certainly makes this pathology a challenge at the level of diagnosis and subsequent management.
Case presentation: Here we present the case of a 73-year-old male patient who presented one year post left nephrectomy complicated by splenectomy (post splenic injury), with two weeks history of diffuse abdominal pain, non-bilious vomiting, and shortness of breath. Workup done revealed a left diaphragmatic hernia containing necrotic-perforated small bowel loops. A laparotomy with intestinal resection, loop ileostomy along with a primary repair of the diaphragmatic defect were performed.
Conclusion: Although a great portion of acquired diaphragmatic hernias remains asymptomatic, they may be presenting with severe symptomatology and aggravating complications. At the level of clinical manifestation, suspicion of diaphragmatic hernia ascends the ladder of differential diagnosis in a patient with combined respiratory and gastrointestinal symptoms and hence is essential to avoid delayed treatment and superimposing lethal complications. Definitive treatment of diaphragmatic hernia is surgical repair.
Keywords: Case report; Diaphragmatic hernia; Iatrogenic diaphragmatic hernia; left nephrectomy; Splenectomy.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Hadeer RA (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Hadeer RA. Case of an adult complicated left diaphragmatic hernia: Case report and literature review. Open J Clin Med Case Rep. 2023; 2027.
Introduction
A diaphragmatic hernia is the protrusion of abdominal structures into the thoracic cavity through a defect in the diaphragm [1]. Overall incidence of diaphragmatic hernia is about 0.8-5/10,000 with the majority being congenital [2]. In adults’ diaphragmatic hernia is rare accounting for less the 5% of the cases [3]. They can be either acquired or due to missed congenital diaphragmatic hernias. The most common among acquired diaphragmatic hernias are those of traumatic origin present in 0.8 to 3.6 of the cases [2]. An iatrogenic diaphragmatic hernia is defined as an acquired defect of the diaphragm, following a thoracic or abdominal surgical procedure during which diaphragmatic lacerations occur that may go unnoticed [4]. Intra-abdominal organs such as the stomach, small intestine, or colon can be incarcerated in the diaphragmatic defect, along with ischemia and subsequent necrosis, which may lead to fatal complications with an overall mortality rate up to 31% [5].
We report here the case of a 73-year-old male patient who presented with left diaphragmatic hernia one year post left nephrectomy for left renal cell carcinoma complicated by splenectomy secondary to intraoperative splenic injury.
Case Presentation
A 73-year-old male patient presented to our emergency department in June 2021 with a history of diffuse abdominal pain, nausea, repeated episodes of non-bilious vomiting, obstipation, dyspnea, and shortness of breath of two weeks duration.
On history, the patient presented five days prior to presentation to a peripheral hospital where a thoracoabdominal CT scan without IV contrast was performed identifying a left diaphragmatic hernia with a small bowel loop occupying the left thorax and pleural effusion. A pleural tap was the only intervention performed before being transferred to our hospital.
Past medical history included hypothyroidism, renal cell carcinoma diagnosed two years ago status post-chemotherapy, left nephrectomy, and splenectomy secondary to intra-op splenic injury in August 2020. There was no history of trauma.
Upon presentation to our emergency department, blood pressure of 90/70 mmHg was found along with tachycardia (heart rate of 110/min), desaturation (oxygen saturation of 87% on 10 L O2 NC), and temperature of 38oC. No breath sounds were detectable in the left chest area. The abdomen was distended, rigid with diffuse tenderness to palpation, and positive bowel sounds.
Laboratory analysis revealed an elevated inflammatory marker (White blood cell count of 11,650/mm3, C-reactive protein of 493 mg/l, LDH 309 IU/L), acute kidney injury (creatinine 1.63 mg/dl) with hyperkalemia (K 6 mmol/l).
Chest radiography showed blunting of the left costophrenic angle reaching the axillary level occupied by bowel loops with a right-sided mediastinal shift. Ct scan of the thorax and abdomen without iv contrast revealed a large left-sided effusion with left diaphragmatic hernia containing small bowel loops with sub-pleural air bubbles, complication secondary to pleural tap, or bowel strangulation/perforation. The caecum was seen in the left side of the abdomen with a swirl sign of the mesentery (whirlpool sign) and associated proximal small bowel dilatation in the left hemithorax through the left posterior diaphragmatic defect. Findings were suggestive of cecal volvulus and small bowel obstruction with left-sided diaphragmatic hernia (Figure 1).
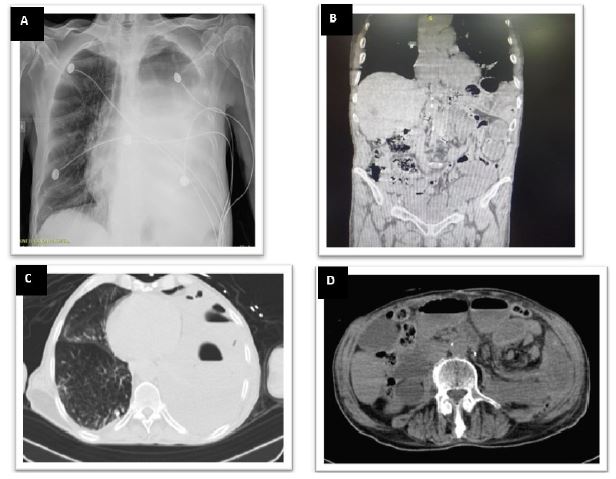
Figure 1: Left diaphragmatic hernia.
(A) Chest X-ray with visceral herniation in the chest and mediastinal shift.
(B) CT, coronal view with small bowel in left side of chest.
(C) CT, transverse view: Left diaphragmatic hernia containing small bowel loops with sub-pleural air bubbles.
(D) CT, transverse view: swirl sign of the mesentery (whirlpool sign) and associated proximal small bowel dilatation in the left hemi-thorax.
(A) Chest X-ray with visceral herniation in the chest and mediastinal shift.
(B) CT, coronal view with small bowel in left side of chest.
(C) CT, transverse view: Left diaphragmatic hernia containing small bowel loops with sub-pleural air bubbles.
(D) CT, transverse view: swirl sign of the mesentery (whirlpool sign) and associated proximal small bowel dilatation in the left hemi-thorax.
Due to hemodynamic instability, a decision was taken for urgent laparotomy.
Intraoperative findings showed a 4 × 2 cm left posterior diaphragmatic hernia (Bochdalek hernia), and a sac containing an ischemic, necrotic and perforated terminal ileal-loop, manifesting as a complicated closed-loop small bowel obstruction. One liter of fecal material was aspirated from the left pleural cavity. Trans-abdominal blunt dissection was followed until complete liberation and reduction of strangulated bowel loops; 20 cm of necrotic terminal ileal loop was retrieved 10 cm away from the ileocecal valve. After an extensive lavage of the abdominal and left thoracic cavity through the diaphragmatic defect with 15L of warm distilled water, the defect was closed with interrupted Ti-Cron non-resorbable sutures 2-0. In this hemodynamically unstable patient, we decided to perform a discontinuity resection with a double-barrel ileostomy. Because of the bacterial contamination and the possibility to approximate the diaphragmatic edge without tension the defect was not reinforced with mesh prosthesis. Drainage to the left upper quadrant and left thoracic chest was placed (Figure 2).
The patient was transferred to the ICU post-Operative. Extubated day one post-Operative, hemodynamically stable with 5 L O2 NC requirements (Figure 3). Diet resumed on day two post-Operative. Intra-Operative cultures returned positive for Ecoli ampC and targeted anti-biotherapy started. During his stay patient presented multiple respiratory complications that required a new chest tube placement, bronchoscopy, CT guided drainage of a left pleural effusion.
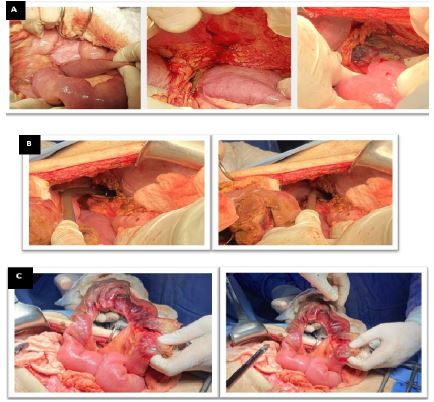
Figure 2: Intraoperative images.
(A) Terminal ileal-loop herniating through a 4x2 cm defect in the left posterior diaphragm and causing a closed loop small bowel obstruction.
(B) Ischemic necrotic bowel loops with fecal material draining from the left thoracic cavity signifying bowel perforation.
(C) 20 cm strangulated and necrotic terminal ileal loop retrieved 10 cm away from the ileo-cecal valve.
(A) Terminal ileal-loop herniating through a 4x2 cm defect in the left posterior diaphragm and causing a closed loop small bowel obstruction.
(B) Ischemic necrotic bowel loops with fecal material draining from the left thoracic cavity signifying bowel perforation.
(C) 20 cm strangulated and necrotic terminal ileal loop retrieved 10 cm away from the ileo-cecal valve.

Figure 3: Chest X-ray pre-OP vs day 1 post-Op.
On the day of discharge, the patient had PUS draining from the chest tube. A CT Chest was done and showed increased air component and decreased fluid
Amount of a previously described loculated pleural effusion with parietal and visceral pleural thickening (Figure 4). Hospital stay was complicated by organized empyema of the left lung, managed with left posterolateral thoracotomy, left lung decortication, and empyema drainage. The patient was then extubated on day 2 post decortication. Re-intubated 10 days after for respiratory failure and then passed away two weeks later from cardio respiratory arrest.

Figure 4: Ct, transversal view: left pleural effusion with parietal and visceral pleural thickening.
Discussion
The diagnosis of diaphragmatic hernia in adults is rare and may be due to missed congenital diaphragmatic hernia or acquired from trauma or as a postoperative complication of certain thoracic and abdominal surgeries. Acquired diaphragmatic hernias are rare, with an overall incidence of < 5% [3]. Trauma is the most common etiology of acquired diaphragmatic hernia. The second most common cause is iatrogenic following surgery, but are very rare, with mostly just case reports in the literature [1].
Two types of congenital diaphragmatic hernias are defined: Morgagni, when the hernia occur through an anterior parasternal foramen, or Bochdalek Hernia (BH), posterolateral hernia, mainly left-sided, representing persistence of the pleuroperitoneal canal. Of all patients with a congenital BH, only 5% will be diagnosed in childhood or adulthood [6,7].
Left sided acquired diaphragmatic hernia are more common. This is due to the protection of the right hemidiaphragm by the liver. The abdominal contents that can herniate into the diaphragm vary, but documented cases include herniation of the stomach, small intestine, mesentery, spleen, and pancreas [8]. In our case, distal ileum with the ileo-cecal valve were herniating through the diaphragmatic defect.
A careful evaluation of a patient with herniated viscus is important to avoid the risk of iatrogenic perforation. Herniated bowel may be massively dilated and mimic tension pneumothorax. A tube thoracostomy in such a situation may result in perforation and/or faecopneumothorax, [9] as is the complication of our case.
The clinical symptoms of patients with a diaphragmatic hernia are usually nonspecific and vary between chest and/or abdominal and in some cases cardiac symptoms. The abdominal contents on the chest put pressure on the lungs and result in shortness of breath and chest pain [9].
On the other hand, medical imaging is very important in the detection of this pathology. The presence of air meniscus signs on the chest x-ray should draw the attention of the clinician to this possible diagnosis. As with our case, this approach may result in some cases being initially misdiagnosed as complex pleural effusions or hydropneumothorax, with dangerous consequence as a diagnostic or therapeutic thoracentesis would be undertaken without further investigation. Furthermore, ultrasonography could be a useful tool, especially for traumatic diaphragmatic hernia, having its significance lies in the ability to show diaphragmatic continuity and herniated organs and reveal associated abdominal organs pathologies. As for the golden standard examination, a computed tomography scan is effective the most in many diaphragmatic cases. It has been reported in previous studies that multi-slice CT imaging is the most efficient modality for diagnosing patients with a high clinical suspicion of acquired DH, owing to that its accessibility, short duration, and ability to identify concomitant pathologies including rib fractures, hydro-pneumothorax, abdominal injuries and degree of bowel compromise if any. The usual features of diaphragmatic injury seen on the MDCT scan are diaphragmatic discontinuity, thickened diaphragm, “collar sign,” visceral herniation, dependent viscera sign, and so on. As for the MRI modality with a well-known high sensitivity for soft tissue, MR imaging may be performed in the selected patients, or on the late presenting diaphragmatic hernia cases where the diagnosis is still in doubt [9].
In our case, the patient presented with hemodynamic instability and acute onset of obstructive gastrointestinal and respiratory symptoms 1-year post left nephrectomy and splenectomy. Chest x-ray and CT scan findings were suggestive of a diaphragmatic hernia with strangulated perforated small bowel loops. In a comprehensive literature review, we have found 13 cases of diaphragmatic hernia post nephrectomy. In this context, it has been suggested that this delay in presentation is a result of the gradual enlargement of small tears in the diaphragm that go unnoticed during surgery. However, referring to our case and intraoperative findings of a bochdalek hernia, delayed presentation of a congenital diaphragmatic hernia couldn’t be ruled out (imaging before nephrectomy was not available for comparison).
The treatment of choice of diaphragmatic hernia is surgical repair. Defects in the diaphragm, no matter how small, will not heal alone due to the thoracoabdominal pressure gradient which will favor enlargement of the defect and hence herniation of abdominal contents [10]. In this acute presentation of our case with strangulated and obstructed viscera, the decision for immediate surgery was appropriate.
The approach to repair depends on the presentation (emergency or elective), size and side of the defect, and the presence of complications. For emergent cases, laparotomy is the preferred approach. An open abdominal approach, and primary closure using simple, figure-of-eight, or horizontal mattress sutures using 0 or 1 non-absorbable material is the most common procedure [11]. Repair using a mesh may be required when the size of defect is too large, and primary closure is not possible. Prosthetic repairs are performed with expanded polytetrafluoroethylene mesh secured by 0 or 1 non-absorbable braided suture, ensuring 2 to 3 cm of overlap beyond the diaphragmatic defect [12]. As well as for chronic long-standing diaphragmatic hernias, edges of the defect become fibrotic, unlike acute diaphragmatic laceration in which the edges can be pulled together without tension. Fixing chronic diaphragmatic hernia frequently requires prosthetic mesh to provide a tension-free repair [12].
Application of a mesh in diaphragmatic injuries associated with solid or hollow viscous injuries was contraindicated given the risk of mesh infection. As biological mesh incorporates into the surrounding tissues which decreases the risk of infection, adhesion, erosion, extrusion, and rejection compared with the synthetic mesh [13].
In our case, urgent trans-abdominal surgery was the best approach in the context of acute presentation and hemodynamic instability, allowing examination of intra-abdominal organs, lysis of extensive adhesions, and exposure of the ischemic area of the bowel. Primary repair without mesh placement was also preferred due to bacterial fecal contamination of the surgical site and the intermediate size of the defect being 4×2 cm. Pulmonary complications are the most common post-operatively with atelectasis being the most frequent complication reported, along with a high incidence of prolonged respiratory failure and a 45% mortality rate [13].
In the case of our patient who passed away due to respiratory complications. Other reported postoperative complications: empyema, anastomosis leak, diaphragm paralysis, evisceration, nosocomial pneumonia, pulmonary embolism, sepsis, cerebrovascular event, and wound infection [11]. On the bright side and for elective repairs, mortality rates of diaphragmatic hernias are low. However, this rate increases up to 80% in emergency surgery, especially in cases accompanied by necrosis and perforation [11].
Conclusion
Acquired diaphragmatic hernias are very rare. Early diagnosis and management are essential to avoid fatal complications. Treatment is operative repair and depends on the presence of other intra-abdominal injuries, patient stability, technical ability of the surgeon, chronicity, location, and the size of the diaphragmatic injury.
References
- Spellar K, Gupta N, Diaphragmatic Hernia, StatPearls Publishing, 2020.
- Kayleigh Spellar. Nagendra Gupta, Diaphragmatic Hernia, Stat Pearls, 2022
- Azam A, Michael K., Post nephrectomy diaphragmatic hernia presenting as progressive dyspnea, BMJ Case Report, 2020.
- Mínguez Ruiz G, García Florez LJ, Arias Pacheco RD, Bear IG, Pérez VR, et al. post-Nephrectomy diaphragmatic hernia, increase suspicion and decrease morbi-mortality: two cases report. Journal of Surgical Case Reports. 2018; 8: rjy224.
- Jing Lu, Bo Wang, Che X, Li X, Qiu G, et al. Delayed traumatic diaphragmatic hernia, A case-series report and literature review. Medicine (Baltimore). 2016; 95: e4362.
- Hemanta K Nayak, Gaurav Maurya, Kapoor N, Kar P. Delayed presentation of congenital diaphragmatic hernia presenting with intrathoracic gastric volvulus: a case report and review. BMJ Case Rep. 2012; bcr2012007332
- Vikramaditya Dump, Praveen Chandrasekharan. Congenital Diaphragmatic Hernia. Stat Pearls. 2021.
- Kishore GSB, Gupta V, Doley RP, Kudari A, Kalra N, et al. Traumatic diaphragmatic hernia: tertiary centre experience. Hernia. 2010; 14: 159-164.
- Suat Eren, Fahri Ciriş. Diaphragmatic hernia: diagnostic approaches with review of the literature. Eur J Radiol. 2005; 54: 448-459.
- Norman Oneil Machado. Laparoscopic Repair of Bochdalek Diaphragmatic Hernia in Adults. N Am J Med Sci. 2016; 8: 65-74.
- Dirican A, Yilmaz M, Unal B, Piskin T, Ersan V, et al, Acute traumatic diaphragmatic ruptures: a retrospective study of 48 cases. Surg Today. 2011; 41: 1352-1256.
- Matthews BD, Bui H, Harold KL, Kercher KW, Adrales G, et al. Laparoscopic repair of traumatic diaphragmatic injuries. Surg Endosc. 2003; 17: 254-258.
- Gulamhusein T, Obeid NR, Pryor AD. Surgical Management: Other Diaphragmatic Hernias in Adults. The SAGES Manual of Foregut Surgery. 2019; 273-297.
