
Open Access, Volume 9
Lung cancer metastasis to the breast: Consideration of an unusual presentation
Nathan Barron1; Christine MG Schammel2*; Robert Rainer2; David P Schammel2; William J Edenfield1
1Department of Internal Medicine, Prisma Health Upstate, Greenville SC, USA.
2Pathology Associates, Greenville SC, USA.
Christine Schammel
Director, Clinical Research, Department of Pathology, Greenville SC, USA.
Tel: 8643636225; Email: christine.schammel@prismahealth.org
Received : March 15, 2023,
Accepted : April 20, 2023
Published : April 21, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: The EML4-ALK fusion oncogene is found in 2 to 7% of all non-small cell lung cancers, most of which are adenocarcinomas. ALK positive lung malignancies are rare; even more rare are primary ALK positive lung malignancies that metastasize to the breast.
Case Report: A 60-year-old female with a left upper lobe pulmonary lesion suspicious for malignancy underwent a wedge resection; pathology revealed pulmonary adenocarcinoma with positive nodes. While an EML4-ALK fusion was identified, the patient refused adjuvant therapy. One month later, a 7mm lesion in the right lower mid-breast was identified; biopsy identified poorly differentiated carcinoma consistent with lung origin. Pemetrexed, Cisplatin, Carboplatin were initiated. Two months later with new onset of back pain, a PET scan revealed a hypermetabolic bony lesion in the third lumbar vertebral body. Biopsy revealed metastatic adenocarcinoma from the lung. The patient began radiation therapy and, given the EML4-ALK fusion, transitioned from standard chemotherapy to targeted therapy. Currently, following completion of radiation therapy, the bony metastasis has resolved and the patient continues to tolerate targeted therapy well.
Conclusion: Metastases to the breast from other primary locations accounts for only 0.2-1.3% of all breast malignancies, but most often these are lung cancer. EML4-ALK fusions are found in 2-7% of pulmonary adenocarcinomas, but indicate use of targeted therapy which portends a high and durable response rate. This is the fifth EML4-ALK fusion oncogene presence in lung cancer metastasis to the breast that managed with targeted therapy, emphasizing the importance of bioanalysis in management.
Keywords: Lung cancer metastases; Metastases to the breast; EML4-ALK fusions; Bioanalysis for targeted mutations.
Abbreviations: (Echinoderm Microtubule-Associated Protein-Like 4)-(Anaplastic Lymphoma Kinase); ALK: Anaplastic Lymphoma Kinase; ED: Emergency Department; CT: Computed Tomography; PET: Positron Emission Tomography; ER: Estrogen Receptor; PR: Progesterone Receptor; Her-2: Human Epidermal Growth Factor Receptor-2; GATA3: Transcription Factor Important In The Differentiation of Breast Epithelia; TTF-1: Thyroid Transcription Factor 1; SOS-10: Son Of Sevenless-10; developmental protein that stops DNA repair; TKI: Tyrosine Kinase Inhibitor; Napsin-1: functional aspartic proteinase that is a new marker for lung cancer
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Schammel C (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Barron N, Schammel CMG, Rainer R, Schammel DP, Edenfield WJ. Lung cancer metastasis to the breast: Consideration of an unusual presentation. Open J Clin Med Case Rep. 2023; 2024.
Introduction
Lung cancer is classified into two categories: small-cell lung cancer representing 15% of cases and the more prevalent non-small cell lung cancer representing 85% of cases. The EML4-ALK fusion oncogene is found in 2 to 7% of all non-small cell lung cancers, most of which are adenocarcinomas. These gene rearrangements are more prevalent in females and young patients as well as in Asian and Western populations [1].
Breast metastases from extramammary locations are rare, representing 0.2%-1.3% of all breast malignancies [2], typically portending a poor prognosis given that, in most cases, widely diffuse metastases of the primary cancer are often present at the time of the breast metastasis discovery [2]. However, in the limited reports of patients with EML4-ALK positive lung cancer metastasizing the breast, patients have demonstrated favorable outcomes to targeted therapy. Here we present an unusual presentation of a single lung metastasis to the breast.
Clinical Case
A 60-year-old female presented to the ED for dyspnea and tachycardia. A CT angiogram of the chest incidentally revealed a left upper lobe spiculated pulmonary lesion (1.4 cm) that was suspicious for malignancy; no mediastinal hilar lymphadenopathy was noted. CT/PET demonstrated a single hypermetabolic left upper lobe lesion with no other evidence of disease. A robotic wedge resection and left upper lobectomy was completed; pathology revealed an invasive pulmonary adenocarcinoma that invaded the visceral pleura, as confirmed on elastin stain, with negative margins; 1/12 nodes were positive for metastatic carcinoma (T2aN1; Figure 1).
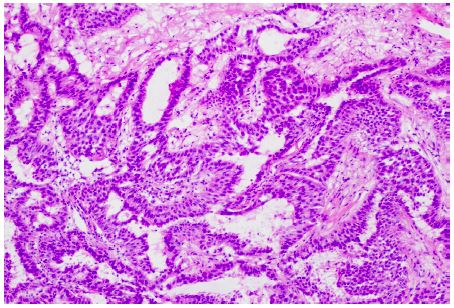
Figure 1: Lung adenocarcinoma histology. The nested pattern with nuclear hyperchromasia (100x), consistent with adenocarcinoma.
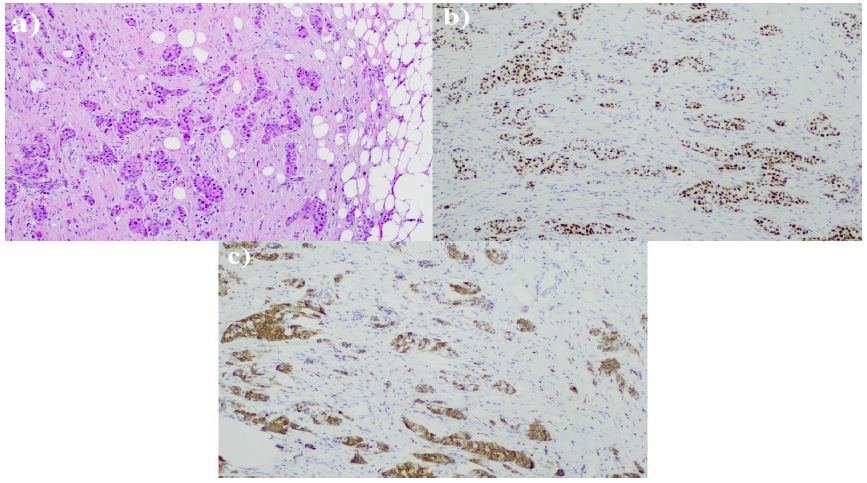
Figure 2: Breast biopsy histology. (a) Infiltrating nests of adenocarcinoma within desmoplastic stroma (100x); (b) immunohistochemical staining for TTF-1 demonstrating positive nuclear staining and (c) immunohistochemical staining for Napsin-A demonstrating positive cytoplasmic staining, indicative of lung adenocarcinoma.
Concordance with the lung adenocarcinoma confirmed that the breast lesion was consistent with metastatic lung cancer (GATA-, mammoglobin -, TTF-1+, Napsin A+, SOS-10+). Staging PET/CT scan revealed no uptake in the lung, minimal uptake in the right breast lesion and a concerning lesion at L3. MRI of the brain was negative for intracranial metastatic disease.
An interventional radiology vertebral biopsy revealed metastatic adenocarcinoma diffusely positive for CK7, TTF-1 and Napsin A consistent with the lung primary (ER and GATA3 negative; Figure 3).
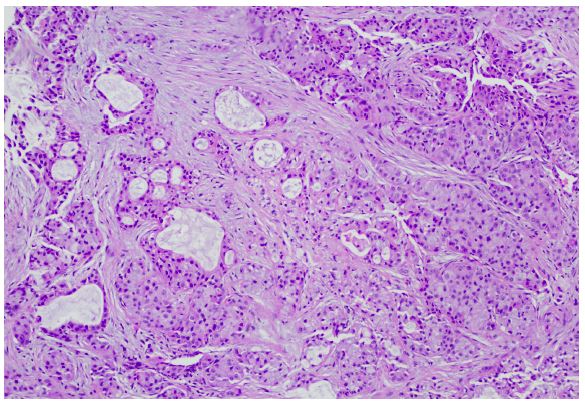
Figure 3: Bone biopsy histology. (a) Adenocarcinoma infiltrating within the bone marrow (100x).
Breast lumpectomy was completed with pathology consistent with adenocarcinoma of lung origin. All margins were negative with the closest margin being 1.2 cm
Radiation therapy for the bony lesion was initiated and completed, which rendered the patient no evidence of disease; once completed, and given the EML4-ALK fusion, the patient was transitioned to, and continues to take, targeted therapy (alectinib; Tyrosine Kinase Inhibitor; TKI). Serial follow-up imaging has revealed stable findings with no evidence of new or recurrent disease 18 months post diagnosis.
Discussion
Breast cancer accounts for 30% of all cancers in women [3]; however, metastases to the breast from other primary locations accounts for only 0.2-1.3% of all breast malignancies [2]. Tumors most often metastatic to the breast are lung cancer (22% of cases), lymphomas (15%), melanoma (13%), gastrointestinal cancers (8%), and papillary serous carcinomas (4%) [4]. Typically, tumors metastatic to the breast portend a poor prognosis.
Histologic analysis and immunohistochemical evaluation of breast lesions can differentiate between primary and metastatic disease. In the case presented here, the IHC of the breast lesion indicated low ER expression with absent PR and Her-2, negative GATA3 [5] and mammaglobin [6], inconsistent with a breast primary; the positive expression of TTF-1 and Napsin A, characteristic of 75% and 84% of lung adenocarcinomas, respectively [7,8] suggested lung origin. While TTF-1 is one of the most commonly utilized IHC markers in the diagnosis of lung cancers, it is also able to distinguish primary lung adenocarcinoma from tumors of other sources, substantiating the breast and spine lesions as lung metastases [9,10].
A comprehensive review of the literature noted 179 reports of lung carcinoma metastases to the breast between 1965 and 2013. In 2013, a systematic review of 31 previously published cases (1989-2013) identified that 87% of patients with lung metastases to the breast were female, 62% were nonsmokers and the median age of diagnosis was 54. Pathologically, 58% of the tumors were adenocarcinomas, none of which expressed ER, PR, or HER-2 positivity [11]. In the case presented here, the presence of the EML4-ALK fusion in both the lung primary and the breast and spine lesions not only suggested metastatic disease, as EML4-ALK fusions are found in only 2-7% [1,12,13] of pulmonary adenocarcinomas, but also indicated use of a targeted therapy that inhibits this fusion kinase and demonstrates high and often durable response [14].
To date, there are only three other reports identifying the EML4-ALK fusion oncogene in lung cancer metastasis to the breast and one widely metastatic breast cancer with this genetic profile. All patients were eventually managed with TKI’s that showed tumor regression [15-17].
Conclusion
Metastasis to the breast is an uncommon phenomenon but must be considered upon discovery of a breast mass in a woman with a history of cancer, especially primary lung cancer. Management of the breast is not the primary concern in such cases as is evidenced by the current case where additional systemic disease was discovered and thus identified the need for effective systemic therapy. Current management of non-small cell lung cancer demands an evaluation for possible actionable mutations. Typically, biomarker assessment is performed with next-generation sequencing panels looking for an ever-growing number of mutations which indicate targeted therapy, often oral agents with a high degree of initial disease control. As noted in our case, targeted therapy allows for effective management of disease that would typically portend a poor prognosis.
Data availability: Data is available with institutional permissions.
Funding statement: No funding was used for this work.
Conflicts of interest: All authors have no conflicts of interest.
All authors have no financial disclosures.
Approvals: This report received IRB approval prior to completion and was found exempt.
References
- Solomon B, Varella-Garcia M, Camidge DR. ALK gene rearrangements: a new therapeutic target in a molecularly defined subset of non-small cell lung cancer. J Thorac Oncol. 2009;4:1450-1454.
- Lee AHS. The histological diagnosis of metastases to the breast from extramammary malignancies. J Clin Pathol. 2007; 60: 1333-1341.
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin. 2021; 71: 7-33.
- Lee AHS, Hodi Z, Soomro I, Sovani V, Abbas A, et al. Histological clues to the diagnosis of metastasis to the breast from extramammary malignancies. Histopathology. 2020;77: 303-313.
- Cimino-Mathews A, Subhawong AP, Illei PB, Sharma R, Halushka MK, et al. GATA3 expression in breast carcinoma: utility in triple-negative, sarcomatoid, and metastatic carcinomas. Hum Pathol. 2013; 44: 1341-1349.
- Baker E, Whiteoak N, Hall L, France J, Wilson D, et al. Mammaglobin-A, VEGFR3, and Ki67 in Human Breast Cancer Pathology and Five Year Survival. Breast Cancer (Auckl). 2019; 13: 1178223419858957.
- Stenhouse G, Fyfe N, King G, Chapman A, Kerr KM. Thyroid transcription factor 1 in pulmonary adenocarcinoma. J Clin Pathol. 2004; 57: 383-387.
- Suzuki A, Shijubo N, Yamada G, Ichimiya S, Satoh M, et al. Napsin A is useful to distinguish primary lung adenocarcinoma from adenocarcinomas of other organs. Pathol Res Pract. 2005; 201: 579-586.
- Schilsky JB, Ni A, Ahn L, Datta S, Travis WD, et al. Prognostic impact of TTF-1 expression in patients with stage IV lung adenocarcinomas. Lung Cancer. 2017; 108: 205-211.
- Kim JH, Kim HS, Kim BJ, Han B, Choi DR, et al. Prognostic Impact of TTF-1 Expression in Non-Squamous Non-Small-Cell Lung Cancer: A Meta-Analysis. J Cancer. 2018; 9: 4279-4286.
- Mirrielees JA, Kapur JH, Szalkucki LM, Harter JM, Salkowski LR et al. Metastasis of primary lung carcinoma to the breast: a systematic review of the literature. J Surg Res. 2014; 188: 419-431.
- Kwak EL, Bang YJ, Camidge DR, et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N Engl J Med. 2010; 363: 1693-1703.
- Pikor LA, Ramnarine VR, Lam S, Lam WL. Genetic alterations defining NSCLC subtypes and their therapeutic implications. Lung Cancer. 2013; 82: 179-189.
- Solomon BJ, Mok T, Kim DW, et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl J Med. 2014; 371: 2167-2177.
- Liu C, Ding L, Sun B, Wu S. Bilateral breast adenocarcinomas with EML4-ALK fusion in a patient with multiple metastases successfully treated with crizotinib: is lung the primary site?. Onco Targets Ther. 2016; 9: 3589-3593.
- Kelly AD, Wiklund T, Kononen J, Creeden J. STRN-ALK Fusion-Positive Case of Breast Cancer With Response to Alectinib. JCO Precis Oncol. 2021; 5: PO.21.00142.
- Wu X, Wang H, Fang M, Li C, Zeng Y, Wang K. ALK or ROS1-rearranged breast metastasis from lung adenocarcinoma: a report of 2 cases. Tumori. 2019; 105: NP67-NP71.
