
Open Access, Volume 9
The importance of color doppler echocardiography and advanced imaging in evaluation of pediatric cardiac symptoms
Murad Almasri1*; Rashmitha Dachepally1; Markus S Renno1; Brian Reemtsen2; Lawrence Greiten2; Christian Eisenring ACNP2; Dala Zakaria1
1Pediatric Cardiology Department, University of Arkansas for Medical Sciences, USA.
2Pediatric Cardiothoracic Surgery Department, University of Arkansas for Medical Sciences, USA.
Murad Almasri
Pediatric Cardiology Section, Arkansas Children’s Hospital, 1 Children’s Way, Slot 512-3, Little Rock, Arkansas 72202-3591, USA.
Email: almasrimurad@uams.edu
Received : February 28, 2023,
Accepted : April 07, 2023
Published : April 10, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Congenital coronary artery anomalies (CCAs) are rare and can be very challenging to diagnose. We present 4 cases of abnormal coronary arteries origins, a child with a left main coronary artery (LMCA) from the right coronary artery (RCA) and 3 others with an RCA from the LMCA.
Keywords: Congenital heart disease; Coronary artery; Imaging.
Abbreviations: CAAs: coronary artery anomalies; ECHO: echocardiography; ECG: electrocardiogram; LMCA: left main coronary artery; LAD: left anterior descedning; LCX: left circumflex artery; RCA: right coronary artery; CTA: computed tomographic angiography; SCD: sudden cardiac death.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Almasri M (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Almasri M, Dachepally R, Renno MS, Reemtsen B, Greiten L, et al. The importance of color doppler echocardiography and advanced imaging in evaluation of pediatric cardiac symptoms. Open J Clin Med Case Rep. 2023; 2013.
Introduction
Despite being rare in children, congenital coronary artery anomalies (CAAs) can present with spectrum from exertional chest pain to myocardial ischemia, arrhythmias, and sudden death [1,2]. Early diagnosis avoids complications and can be affected by the nature of presenting symptoms, if any. Diagnosis of CCAs by 2D transthoracic echocardiography (ECHO) can be challenging, especially in older children and teenagers, or those with limited acoustic imaging windows. Therefore, a meticulous evaluation with color Doppler echocardiography in addition to 2D images is essential. Although ECHO can suggest an abnormal origin of the coronary arteries, color Doppler echocardiography and advanced imaging techniques such as cardiac Computed Tomographic Angiography (CTA) are valuable as diagnostic and confirmatory imaging modalities. We present four cases of abnormal coronary artery origins from the opposite sinuses, including one child with a Left Main Coronary Artery (LMCA) from the Right Coronary Artery (RCA) and 3 patients with an RCA from the LMCA.
Case Series
Patient 1
A 17-year-old male presented to the cardiology clinic for evaluation of a 3-year history of burning intermittent chest pain associated with exertion. He declined shortness of breath or loss of consciousness. His vital signs were unremarkable except for a blood pressure of 135/90. His family history was significant for hypertension. His physical exam and electrocardiogram (ECG) were normal. His 2D Echo suggested normal coronary origins (Figure 1), but color Doppler of the right coronary artery (RCA) was abnormal (Figure 2). An exercise stress revealed significant ST changes with ST depression and T wave inversion in inferior and lateral leads during maximum exercise and during recovery. CTA of the coronaries demonstrated that the RCA arose from the left wall of the ascending aorta, superior to the origin of the LMCA, with a 7mm intramural course and narrowed caliber (Figures 3 and 4). The RCA gave rise to the posterior descending coronary artery. After consideration of risks and benefits, he underwent unroofing of the RCA intramural course and tolerated the surgery without complications. He currently plays basketball with no symptoms.
Patient 2
A 6-year-old male presented for evaluation of chest pain with activity and eating. Shortness of breath and palpitations often accompanied his chest pain. There were no episodes of syncope. His vitals were normal, and his physical exam was unremarkable. His ECG showed prominent left sided voltages and his ECHO showed Left Main Coronary Artery (LMCA) dilation. The RCA was not well seen by 2D but Color Doppler was abnormal with coronary flow seen originating from the left side of the aortic wall. CTA was remarkable for an aberrant RCA arising from the left sinus of Valsalva near the sinotubular junction with an intramural course (4.5 mm). An exercise stress test was normal. Due to his young age, he was followed conservatively for 2 years during which he reported less chest pain complaints. However, at age of eight years, he presented with an episode of chest pain and associated color change and diaphoresis while playing with friends at home. He underwent RCA unroofing, with intraoperative findings of a slit like RCA ostium and < 2 mm intramural diameter shown in Figure 5.
Patient 3
An 18-year-old male with a past medical history of hypertension presented to the cardiology clinic for an episode of syncope that occurred after he stood up suddenly. He was unconscious for several seconds before awakening and gradually returned to baseline level of consciousness with no neurological defects. He denies any palpitations prior to the episode of syncope. He has had no previous episodes of syncope and none since that time. His vital signs in the clinic were within normal limits except for a blood pressure of 155/74. His physical exam was remarkable for an ejection click along the left sternal border when standing and sitting with no S3 or S4, murmur, rub or gallop. No history of fatigue, inappropriate diaphoresis, cyanosis, tachypnea, or shortness of breath. ECG showed normal sinus rhythm with nonspecific T wave changes. Cardiopulmonary stress test did not show arrhythmia or repolarization abnormalities during all exercise stages and recovery. Because of syncope and hypertension, an ECHO was done and was notable for a bicuspid aortic valve (right and left cusp commissure fused) and a normal LMCA origin. Although the 2D images were reassuring of a normal origin of the RCA, the Color Doppler raised concerns of abnormal origin of the RCA arising from the LMCA with an intramural course (Figure 6). Patient was instructed to start Lisinopril, but was lost to follow up. The patient returned a year later, continued to have hypertension but otherwise asymptomatic.
A CTA of the coronaries showed the RCA arising anomalously from the origin of the LMCA and taking an intramural course of about 17.5 mm in length between the aortic root and right ventricular outflow tract, with the posterior descending coronary artery supplied by the right coronary artery (Figure 7). Although the patient did not have exertional symptoms, such as post exercise syncope or chest pain and his exercise testing was normal, it was decided to repair his RCA surgically due to the length of its intramural course. The patient is scheduled to undergo coronary unroofing during his winter break.
Patient 4
A 4-year-old male was diagnosed with anomalous LMCA arising from the right (single RCA) as an incidental finding on an ECHO performed for evaluation of a heart murmur. He denied chest pain, palpitations or arrhythmia, fatigability, syncope or near syncope. The patient is physically active with no exertional symptoms. He had a normal physical exam and ECG. 2D Echo images suggested an anomalous origin of the LMCA from the RCA with the LMCA coursing anteriorly between the aorta and the pulmonary artery with a possible intramural course. Color Doppler Echo confirmed the diagnosis with coronary flow seen crossing from right to left side of aortic wall (Figure 8). CTA of his coronaries further delineated the anatomy, showing that the LMCA arises anomalously from the proximal RCA, coursing around the aorta at the sinotubular ridge with a stenotic 15 mm intramural segment and normal origin of the RCA from the right sinus of Valsalva (Figures 9 and 10). He will be scheduled for coronary unroofing surgery.

Figure 1: 2D echocardiogram clip suggesting normal origin of the RCA from the right coronary sinus.
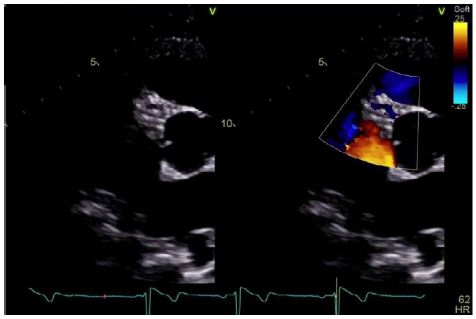
Figure 2: Color Doppler Echocardiogram demonstrating abnormal flow that was thought to be in the RCA.

Figure 3: Flythrough CT reconstruction showing the narrow slit-like orifice of the RCA ostium.
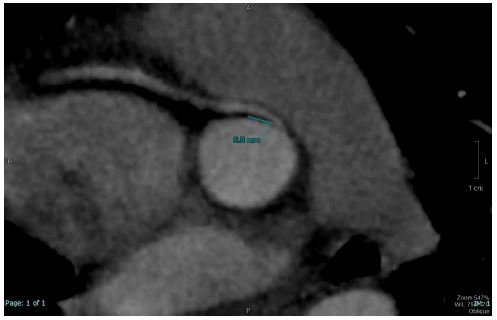
Figure 4: Cardiac CT showing the RCA arising from the left wall of ascending aorta with a 7mm intramural course and narrowed caliber.
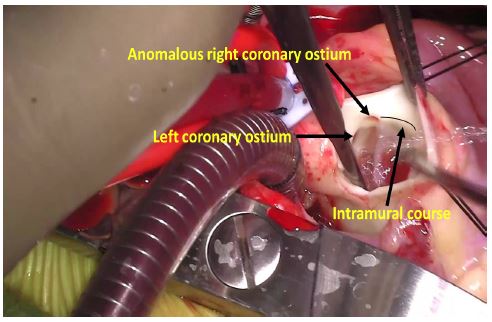
Figure 5: An intra-operative picture showing the slit-like anomalous RCA ostium (upper black arrow) with demonstration of the intramural course (lower black arrow and curved line). The left coronary ostium is also seen and is normal (left black arrow).
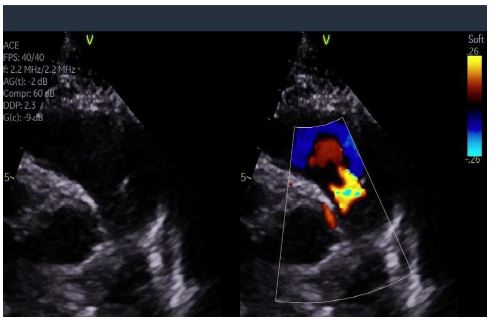
Figure 6: Color Compare Echocardiogram clips suggesting an anomalous origin of the RCA from the left coronary cusp.
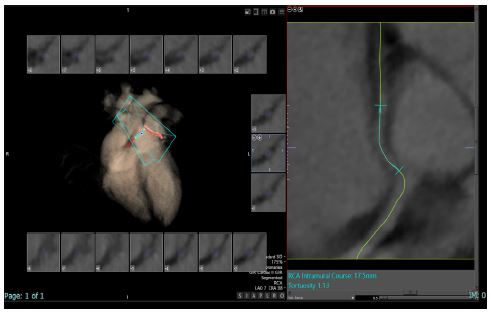
Figure 7: CT angiogram showing the RCA arising anomalously from the origin of the LMCA and taking an intramural course of about 17.5mm in length between the aortic root and right ventricular outflow tract.
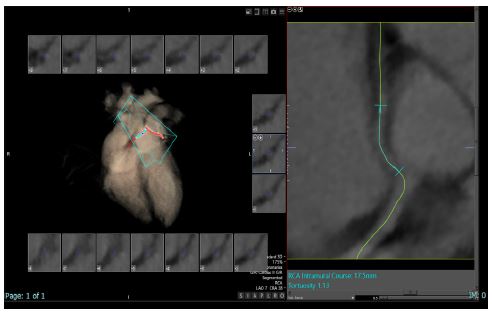
Figure 8: Color compare Echocardiogram demonstrating coronary flow from the right to the left side of the aortic wall consistent with anomalous origin of the LMCA from the right sinus of Valsalva.
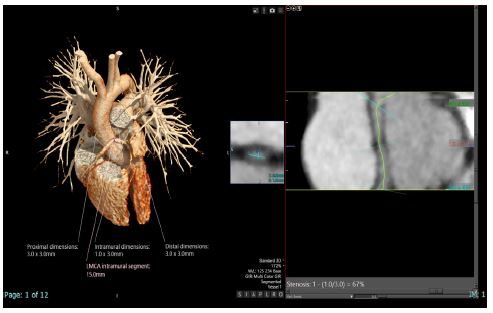
Figure 9: Left: 3D CT reconstruction of the patient’s heart showing the LMCA arising anomalously from the proximal RCA, coursing around the aorta at the sinotubular ridge with a stenotic 15 mm intramural segment. Right: Curved multiplanar CT reconstruction demonstrating the intramural segment.
Discussion
Congenital CAAs include a diverse group of pathologies with different presentations that are classified by some authors as major vs minor anomalies [3]. Patients with congenital CCA can be asymptomatic and are sometimes identified following an ECHO that was done for other purposes. Those with symptoms may present with chest pain, arrhythmia, myocardial infarction, syncope, and sudden death [4,5]. A subgroup of CAAs which can carry serious implications is an anomalous origin of a coronary artery from the opposite sinus which albeit uncommon, have a higher risk of sudden cardiac death (SCD), especially at a younger age. Risk of SCD is increased particularly when the coronary artery has a course between the aorta and the pulmonary artery with compression of the intramural course [6].
Diagnosis is sometimes missed by 2D ECHO. However, color Doppler ECHO is an additional valuable imaging tool that can delineate the abnormal origin of the coronary artery from the opposite sinus and the intramural course. Coronary CTA is currently regarded as the gold standard for the identification and visualization of CAAs, as it offers the best performance in terms of spatial resolution, acquisition time, and image contrast [6]. Coronary unroofing procedure is used to restore a more normal ostia location and luminal diameter thereby alleviating the risk of SCD [7].
Declarations
Disclosures: The authors have nothing to disclose.
Funding: The authors have no relationships relevant to the contents of this paper to disclose.
References
- Frommelt PC, Frommelt MA. Congenital coronary artery anomalies. Pediatr Clin North Am. 2004; 51: 1273-1288.
- Roberto Barriales-Villaaand César Morís de la Tassa, Congenital Coronary Artery Anomalies With Origin in the Contralateral Sinus of Valsalva: Which Approach Should We Take? 2006; 59: 360-370.
- Angelini, Paolo. Coronary artery anomalies. Baltimore: Lippincott Williams & Wilkins, 1999.
- Yamanaka, Osamu, Robert E. Hobbs. “Coronary artery anomalies in 126,595 patients undergoing coronary arteriography.” Catheterization and cardiovascular diagnosis. 1990; 21: 28-40.
- Angelini, Paolo. “Coronary artery anomalies: an entity in search of an identity.” Circulation. 2007; 115: 1296-1305.
- Villa AD, Sammut E, Nair A, Rajani R, Bonamini R, Chiribiri A. Coronary artery anomalies overview: The normal and the abnormal. World J Radiol. 2016; 8: 537-555.
- Bonilla-Ramirez C, Molossi S, Caldarone CA, Binsalamah ZM. Anomalous Aortic Origin of the Coronary Arteries - State of the Art Management and Surgical Techniques. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2021; 24: 85-94.
