
Open Access, Volume 9
A benign radiological spleen for a rare malignant splenic angiosarcoma
Lianne Cheong1; Ganti Srujana2; Wai Ching Deanna Lee3*
1Associate Consultant, Department of Internal Medicine, General Medicine, Sengkang General Hospital, Singapore.
2Consultant, Department of Radiology, Sengkang General Hospital, Singapore.
3Consultant, Department of Internal Medicine, General Medicine , Sengkang General Hospital, Singapore.
Wai Ching Deanna Lee
Department of Internal Medicine, General Medicine, Sengkang General Hospital, Singapore.
Tel: 65-6930-2914; Email: deanna.lee.w.c@singhealth.com.sg
Received : November 11, 2022,
Accepted : February 08, 2023
Published : April 10, 2023,
Archived : www.jclinmedcasereports.com
Abstract
We discuss a case of a 69-year-old female presenting with unintentional loss of weight. Computer tomography of the abdomen revealed mottled liver appearance and cystic liver lesion equivocal for splenic hemangioma. Subsequent ultrasound guided biopsy reviewed atypical cells with immunohistochemically staining consistent with a diagnosis of Angiosarcoma. In summary Primary Splenic Angiosarcoma is a rare but aggressive neoplasm with variable presentation which may pose a diagnostic challenge.
Keywords: Mottled spleen; Primary splenic angiosacroma; Splenomegaly; Splenic malignancy.
Abbreviations: PSA: Primary Splenic Angiosarcoma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Deanna Lee WC (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Cheong L, Srujana G, Deanna Lee WC. A Benign Radiological Spleen for a Rare Malignant Splenic Angiosarcoma. Open J Clin Med Case Rep. 2023; 2010.
Introduction
Primary Splenic Angiosarcoma (PSA) was first described in 1879 by T Langerhan [1]. While being the most common primary neoplasm of the spleen, it is an extremely rare malignant neoplasm largely confined to case reports with an incidence of 0.14 to 0.25 cases per million persons . Clinical presentation is variable, including weight loss, lethargy, abdominal distension, and abdominal pain. PSA can also present with spontaneous splenic rupture [3].
Case Presentation
Our patient is a 69-year-old Chinese lady who presented with unintentional weight loss of 9 kilograms over a one-year duration. Her past medical history included Type 2 Diabetes mellitus, hypertension, hyperlipidemia, uterine fibroids status post hysterectomy and multinodular goiter for which she underwent a total thyroidectomy and was on Levothyroxine replacement. Her physical examination revealed generalized cachexia but was otherwise unremarkable. The laboratory work up shows normochromic normocytic anaemia. White cell and platelet counts, renal and liver function tests were within normal reference range. Thyroid function test showed adequate replacement.
Computer tomography of the abdomen showed multiple low-density lesions of the liver, some with soft tissue attenuation but without enhancement, and borderline splenomegaly was also noted with mottled splenic enhancement. Multiple sclerotic bone lesions were noted (Figure 1).
Magnetic resonance imaging of the liver was ordered for further delineation of lesions which revealed multiple liver cystic lesions, some with T1w hyperintense signal while others demonstrated internal filling defects (Figure 1). Differentials included polycystic liver disease or biliary hamartomas. Enhancing splenic lesions were also noted and differentials included hamartoma, lymphangioma, extramedullary haematopoiesis or angiosarcoma.
Bone scan done was unremarkable and not suggestive of osteoblastic bone metastasis. Esophagogastroduodenoscopy was unremarkable aside from mild antral gastritis. Colonoscopy revealed a 3 mm descending colon sessile polyp, for which histology was consistent with a hyperplastic polyp.
Tumour Markers were obtained, including Carcinoembryonic Antigen, Cancer Antigen- 125 and Cancer Antigen 19-9 were within normal reference ranges. Myeloma immunofluorescence analysis was negative for M- bands.
Patient subsequently underwent ultrasound guided plugged biopsy of splenic lesions. Ultrasound findings noted very heterogeneous spleen with multiple iso to hyperechoic nodules. Histopathology findings revealed cellular proliferation of atypical cells with vasoformative features and pseudo-papillary architecture. Immuno-histochemical staining was positive for ERG and negative for AE1/3 and CD45 in keeping with angiosarcoma.
The patient was initiated on a chemotherapy regimen of intravenous Paclitaxel and had radiological response with interval reduction of size of primary splenic mass. Unfortunately, she was admitted with acute abdominal pain with imaging showing rupture of liver metastasis. Decision was made for palliative care, and she subsequently demised six days later.
Imaging Findings
On a CT scan, the spleen demonstrated borderline enlargement, measuring 12 cm and contained multiple hypodense lesions. There were also innumerable liver lesions, some of which contained non-enhancing foci of internal hyperdensity. Extensive tiny sclerotic metastases were noted in the axial and appendicular skeleton.
On an MR liver, the splenic lesions demonstrated heterogenous T1 hypointensity with and T2 hyperintense signal. The liver lesions were found to be cystic in nature, some with internal T1 hyperintense signal and in keeping with foci of haemorrhage. A PET CT demonstrated increased avidity of the splenic, liver and bone lesions.
Subsequent to this, the patient presented with acute abdominal pain and was found to have a ruptured segment V liver metastasis with a large haematoma in the pelvis, measuring 7.7 x 6.2 cm and moderate volume haemoperitoneum. No active focus of haemorrhage was found on catheter angiography but the right hepatic artery branches were empirically embolised.
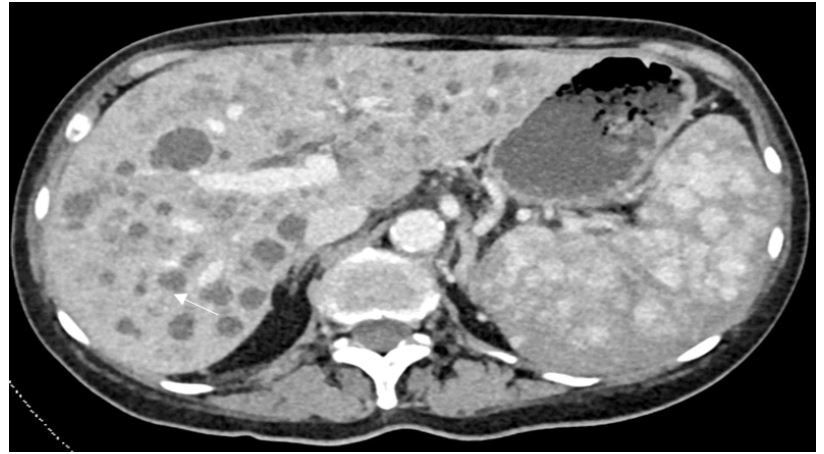
Figure 1: Axial CT scan image demonstrating a mottled appearance to the spleen and multiple liver hypodense lesions, some of which contain internal hyperdensity (white arrow)

Figure 2: Coronal CT image showing extensive sclerotic bone metastases.
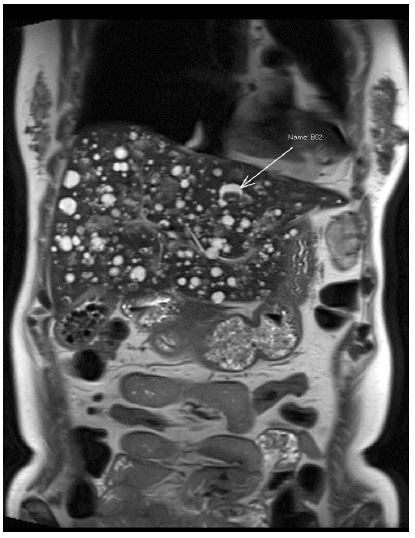
Figure 3: Coronal T2 weighted image demonstrating multiple cystic liver lesions with internal hypointense components (white arrow).
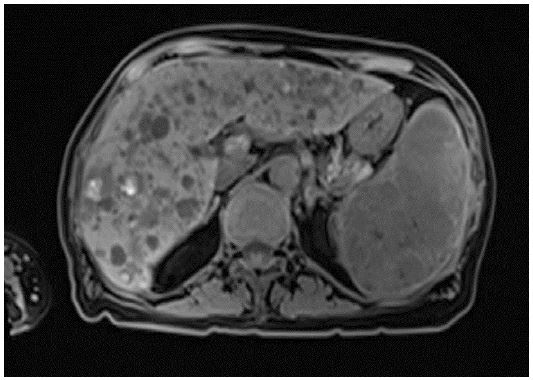
Figure 4: Axial T1 weighted image demonstrating hyperintesnse foci within the liver lesions, in keeping with haemorrhagic foci.

Figure 5: Coronal CT image demonstrating a large haematoma inferior to the liver (white arrow) and within the pelvis (black arrow), secondary to a ruptured, haemorrhagic liver metastases.
Discussion
PSA is an aggressive malignant vascular neoplasm, presumed arising from vascular endothelium of splenic endothelium. To date only 300 cases of splenic angiosarcoma have been reported, yet it remains the most common primary non lymphoid malignant neoplasm [3]. Most commonly it occurs in patients aged above 40 and peaks in the sixth to seventh decade of life, although any age group can be affected. Radiation exposure is a recognized risk factor in other forms of angiosarcoma of the breast, skin and soft- tissues. Case series reported radiation exposure in 28 out of 110 cases of PSA with an average interval of radiation exposure to presentation of 9.5 years [5].
The most common symptom is abdominal pain, presenting in 60-75% of patient 56~~. Other clinical presentations include abdominal distension, anemia, fever, loss of appetite, loss of weight and breathlessness. 30-60% of patients may present with splenic rupture requiring emergency surgery [5]. Metastasis is noted in virtually all patients at the point of diagnosis, most commonly the liver, followed by lungs, omentum and bones [6]. In view of its variable clinical presentation, misdiagnosis at early presentation is not uncommon. Common misdiagnosis includes splenic metastasis, splenic hemangioma or lymphoma [6]. Diagnosis via splenic biopsy also carries significant bleeding risk as a highly vascular organ and may not be often performed.
PSA remains an aggressive neoplasm. Prognosis is poor with a median survival of 5 months [6 ]. The risk of splenic rupture with resultant hemorrhagic shock and disseminated intravascular coagulopathy remains a feared complication with a high mortality. Splenectomy remains the only curative treatment if diagnosed early.
Primary splenic angiosarcoma is a rare condition that produces a diagnostic conundrum. The splenic lesions can range from multiple discrete masses or as a solitary mass [8] and commonly metastasis to the liver and spine [9]. On Magnetic Resonance Imaging, the splenic, and by extension, liver lesions may demonstrate haemosiderin staining or be of cystic nature with internal high signal, in keeping with blood products [9,10]. They are also prone to haemorrhage or present with acute intraperitoneal hemorrhage, as was the case in our patient.
Conclusion
PSA is a rare and aggressive condition which produced a diagnostic uncertainly in our case here. While the radiological image may look benign, the histopathology concurred with the clinical findings of malignancy where the patient presented with weight loss and cachexia. This is another lesson to correlate patient’s presentation with both radiological and laboratory findings.
Acknowledgement: We would like to acknowledge Prof C Rajasoorya, Dr Richard Yiu, Dr Alvin tan for their assistance in the diagnostic dilemma of this patient.
References
- Langhans T. 1879. “Pulsating cavernous neoplasm of the spleen with metastatic nodules to the liver.” Virchows Arch PAthol Anat. 1879; 75: 273-291.
- Hamid KS, Rodriguez JA, Lairmore TC. “Primary splenic angiosarcoma.” JSLS 2010; 14: 431-435.
- Falk S, Krishnan J, Meis JM. “Primary angiosarcoma of the spleen. A clinicopathologic study of 40 cases.” Am J Surg Pathol. 1993; 17: 959-970.
- Filip K, Ladislav B, Branislav B. “Primary Angiosarcoma of the Spleen: Rare Diagnosis with Atypical Clinical Course.” Case Reports in Oncological Medicine. 2016.
- Neuhauser T., Derringer G, Thompson L. “Splenic Angiosarcoma: A Clinicopathologic and Immunophenotypic Study of 28 Cases.” Mod Pathol. 2013. 978–987.
- Li R, Li M, Zhang L. “Clinical Characteristics and Prognostic Factors of Primary Splenic Angiosarcoma: A Retrospective Clinical Analysis from China.” Cell Physiol Biochem. 2018; 49; 1959-1969.
- Duan YF, Y. Jiang CX, Wu. “Spontaneous rupture of primary splenic angiosarcoma: a case report and literature review.” World Journal of Surgical Oncology. 2013; 53.
- Bhaludin BN, Thway K, Adejolu, M. et al. Imaging features of primary sites and metastatic patterns of angiosarcoma. Insights Imaging. 2021 ;12: 189.
- Krol, J, Krol, V, Dawkins A, & Ganesh HS. Case 213: Primary Splenic Angiosarcoma. Radiology. 2015; 274; 298–303.
- Thompson M, Levy D, Aguilera N, Gorospe L & Abbott M. Angiosarcoma of the Spleen: Imaging Characteristics in 12 Patients. Radiology. 2005; 235: 106–115.
