
Open Access, Volume 9
Severe post-COVID virus positive lymphocytic myocarditis with infective endocarditis: Сhallenges of diagnosis and treatment
Blagova OV1*; Lutokhina Yu A1; Ainetdinova DH1; Evseev EP2; Rubtsova SE1; Krivtsova SN1; Alexandrova SA3; Kogan EA1
1The State Education Institution of Higher Professional Training The First Sechenov Moscow State Medical University under Ministry of Health of the Russian Federation, 8-2, Trubetskaya street, Moscow, 119992.
2B.V. Petrovsky Russian Research Center of Surgery, Russian Federation, Moscow, Abrikosovsky str, 2, 119992.
3A.N. Bakulev Research Center for Cardiovascular Surgery, 135 Rublevskoe Shosse, Moscow, 121552.
Blagova OV
The State Education Institution of Higher Professional Training The First Sechenov Moscow State Medical University under Ministry of Health of the Russian Federation, 8-2, Trubetskaya street, Moscow.
Email: blagovao@mail.ru
Received : February 27, 2023,
Accepted : April 03, 2023
Published : April 05, 2023,
Archived : www.jclinmedcasereports.com
Abstract
A 39-year-old patient with bicuspid aortic valve underwent COVID-19 in August 2020. In September, he developed fever, dyspnea, arthralgias, hemorrhagic rash, followed by biventricular heart failure (December 2020). In March 2021 inflammatory changes in blood and anti-heart antibodies were observed along with heart chambers dilatation, decreased ejection fraction (25%), aortic valve stenosis with regurgitation and vegetation on the aortic valve. Blood culture was negative. Endomyocardial biopsy revealed SARS-CoV-2-positive lymphocytic myocarditis. Antibiotics, intravenous immunoglobulin, and later methylprednisolone were administered. Ejection fraction increased to 42%. Aortic valve replacement was performed six months later. SARS-CoV-2 was not detected in intraoperative myocardial biopsy specimens.
Keywords: SARS-CoV-2; Post-COVID-19 myocarditis; Infectious endocarditis; Endomyocardial biopsy; Corticosteroids
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Blagova OV (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Blagova OV, Lutokhina Yu A, Ainetdinova DH, Evseev EP, Rubtsova SE, et al. Severe post-COVID virus positive lymphocytic myocarditis with infective endocarditis: Сhallenges of diagnosis and treatment. Open J Clin Med Case Rep. 2023; 2009.
Introduction
The new coronavirus infection pandemic (COronaVIrus Disease 2019, COVID-19) has drawn attention to various forms of inflammatory heart disease. The possibility of myocarditis resulting from exposure of the myocardium to coronavirus (severe acute respiratory syndrome-related coronavirus 2, SARS-CoV-2) has been reported [1]. In addition to myocarditis in acute COVID-19, we have described for the first time cases of morphologically verified post-COVID myocarditis with persistence of the virus in the myocardium for up to 9 months [2]. Previously, only short-term (1 month) persistence with rapid myocarditis regression and elimination of the virus has been reported [3]. Even less is known about the development of endocarditis after COVID-19. An epidemiological study in Denmark showed that the incidence of IE in the first quarter of 2020 was similar to that for the period 2018-2019 [4].
Cases of Infective Endocarditis (IE) have been described both in the acute period of COVID-19 [5] and early afterwards [6]. They are particularly noteworthy because of the presumed mutual adverse effects of viral and bacterial infection. The combination of myocarditis and endocarditis is in principle quite rare. Such a coexistence is due to either an infection (bacterial, fungal, viral) or an autoimmune process (rheumatism, systemic vasculitis, lupus, hypereosinophilic syndromes). In COVID-19 both factors are involved, but the results of their interaction at the cardiac level have not been studied. Moreover, there are no cases of successful simultaneous treatment of endocarditis and myocarditis in patients with COVID-19. Treatment approaches for such patients have not been developed.
Case Report
A 39-year-old male was admitted to the clinic on 05.03.2021 with complaints of shortness of breath at minimal physical exertion, palpitations, weakness, aching pains in extremities, weight loss of about 20 kg within six months. Brother suffers from diabetes mellitus type 1, parents had type 2 diabetes. In childhood a bicuspid aortic valve (AV) was diagnosed. The patient was asymptomatic. In July 2020 he had COVID-19 (fever up to 38oC for a week, weakness). Later appearance of IgG to SARS-CoV-2 was registered. After a month, fever resumed up to 38.5oC with chills and sweating, pain in large joints (took NSAIDs), macular rash with small red lesions on the shins, leg edema. Since October, dyspnea appeared and progressed. EchoCG showed normal ejection fraction (EF, 60%) and I grade aortic regurgitation. Heart chambers were not dilated. No evidence of pneumonia or endocarditis was found. The condition was diagnosed as rheumatoid arthritis, therapy with sulfasalazine 1.0 g/day was initiated, followed by methylprednisolone 4 mg/day. In late December, CT scan revealed interstitial pulmonary edema, bilateral pleural effusion, lymphadenopathy. A right pleural puncture was performed and 1200 ml were evacuated. EchoCG showed EF reduction up to 33%, left ventricular (LV) dilatation and hyperechogenic rounded masses on the AC cusps. Antibiotic therapy was administered for 2 weeks with temporary regression of fever. In January 2021, dyspnea deteriorated. Treatment with antibiotics, diuretics and carvedilol was ineffective.
On admission to the clinic patient’s condition was severe. Body temperature was 36.6oC, BMI 20.07 kg/m2. Heart rate 102 BPM, regular rhythm, BP 80/60 mmHg. The physical examination revealed pale skin with an earthy hue, diminished vesicular breath in the basal parts of the lungs, dull heart tones, systolic murmur with epicenter over the aorta and diastolic murmur best heard at the left sternal border, liver enlargement (+5 cm) and palpable lower pole of the spleen.
Withdrawal of NSAIDs resulted in fever with chills up to 39oC started. Hypotension worsened, which required cardiotonic support. Blood tests showed hypochromic anemia (Hb 84-99 g/l, serum iron 15.8 μmol/l,), proinflammatory changes (dysproteinemia, neutrophilic leukocytosis (12.3-19.4x109/l), CRP (17.5-177.3 mg/L), D-dimer (1.18-3.99 μg/L), ferritin 1832.1 μg/l), signs of cytolysis and cholestasis (AST up to 5016 units/L, ALT up to 3993 units/L). Troponin levels were within normal ranges. Urinalysis shows slight proteinuria and leukocyturia.
ECG showed sinus tachycardia (Figure 2a), 24-hour ECG monitoring revealed no significant rhythm abnormalities. EchoCG visualized dilated left chambers (LV EDD 6.4 cm, 3.72 cm/m2, EDV 204 ml, ESV 136 ml, left atrium 78 ml), systolic function dramatically decreased (EF 25%, VTI 14 cm, dp/dt 909 mmHg), sPAP 40 mmHg. The Transesophageal EchoCG revealed a 0.3 × 0.5 cm echopositive mobile mass in the right commissure area (Figure 2b), bicuspid valve cusps were thickened, aortic stenosis (aortic orifice area 1.1 cm2, AV velocity 441 cm/s, maximum and mean gradients 77 and 42 mmHg.) was combined with grade II aortic regurgitation (Figure 2c).
Blood culture was negative, but procalcitonin level were significantly increased (1.94 ng/ml, normal less than 0.07 ng/ml). On the basis of one major and at least 4 minor criteria, bicuspid AV IE was diagnosed. Antibiotic therapy with vancomycin 2 g/day and ceftriaxone 2 g/day, intravenous infusion of 50 g immunoglobulin were performed for 4 weeks. Body temperature and procalcitonin levels normalized. At the same time there was evidence of myocarditis: elevated anti-heart antibodies levels (1:160-1:320), signs of myocardial oedema and subepicardial delayed accumulation on MRI (Figure 2g).
Endomyocardial Biopsy (EMB) of the right ventricle was obtained: no evidence of active endocarditis was found (Figure 2B). PCR detected no DNA of cardiotropic viruses or pathogenic bacteria and biopsy culture was negative. Active lymphocytic myocarditis was confirmed both by hematoxylin and eosin staining and immunohistochemical study (Figure 3B,G). SARS-Cov-2 spike and nucleocapsid proteins were detected predominantly in infiltrate and vascular endothelial cells, PCR detected SARS-Cov-2 RNA in myocardium.
Therapy with methylprednisolone 32 mg/day in combination with ceftriaxone, linezolid, spironolactone, furosemide and carvedilol was initiated, later an insulin was added due to manifestation of diabetes mellitus as an adverse effect of glucocorticosteroid administration (glycaemia up to 26 mmol/l). The fever did not relapse. The patient’s condition improved: dyspnea decreased dramatically and inflammatory changes in the blood regressed. Three months later, EF increased to 42%, and the patient returned to his usual activities. In September AV was replaced with a mechanical prosthesis. At revision the AV was monocusp, with calcified vegetations up to 5 mm on the leaflets, in the area of the mitral-aortic junction there was an open abscess cavity. The valve culture was also negative for any growth. Intraoperative biopsies revealed signs of bacterial valve endocarditis (Figure 3E) and lymphocytic infiltration in the myocardium (Figure 3E). SARS-Cov-2 RNA was not detected in the myocardium by PCR.
Therapy with methylprednisolone 4 mg/day was continued. A follow-up echocardiography showed increase in EF over 40% in the first month after the surgery. Later the patient went to the USA, returned to active sport exercises (running), did not perform EchoCG.
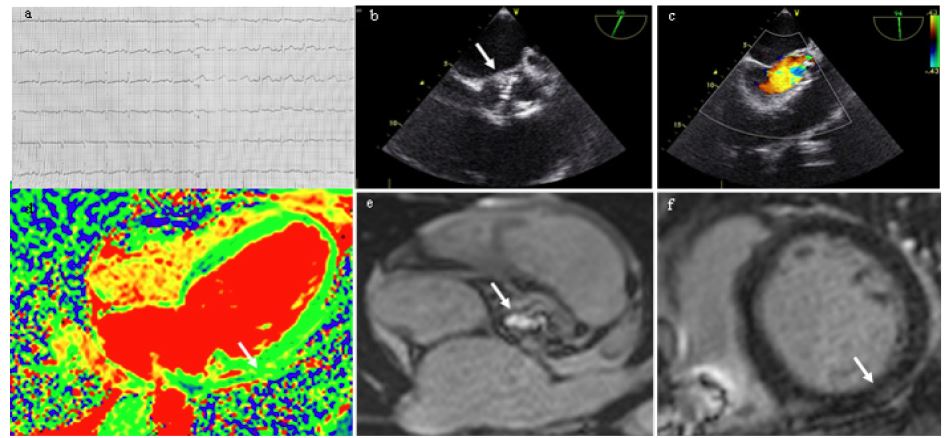
Figure 1: Results of instrumental investigations. (a) - ECG, paper speed 25 mm/sec: sinus tachycardia; b, c - EchoCG: vegetation on the aortic bicuspid valve cusp (b), aortic regurgitation (c); d-f - Contrast enhanced cardiac MRI: LV lateral wall edema, T2, arrow (d); marked aortic orifice narrowing, arrow (e); subepicardial LGE along the LV posterior segment at basal level with spreading to the middle segment, arrow (f).
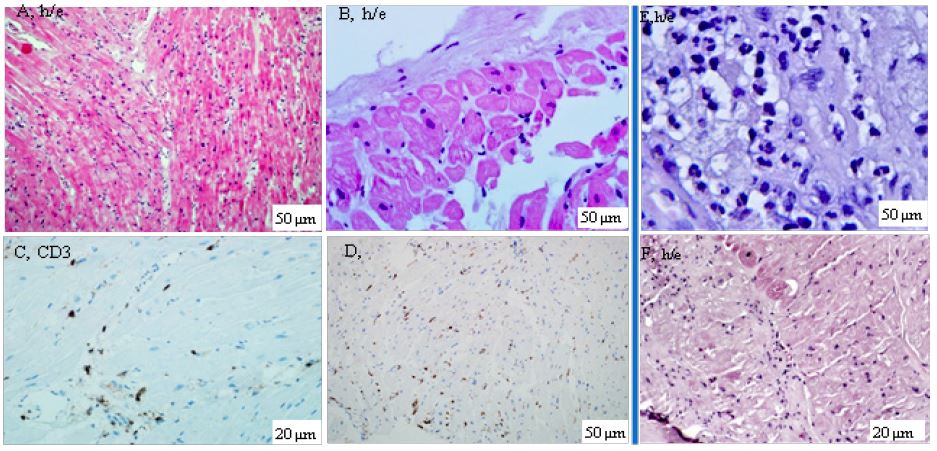
Figure 2: Results of morphological study of the heart. A-F - endomyocardial biopsy specimens from the right ventricle; cardiomyocyte dystrophy and death combined with lymphohistiocytic infiltration (A), sclerosis and endocardial thickening without signs of inflammation (B), presence of more than 7 CD3 positive cells (C) and more than 14 CD45 positive cells (D) per 1 mm2 - immunohistochemical study confirms the diagnosis of lymphocytic myocarditis; E and F are intraoperative biopsy specimens from the endocardium of the removed aortic valve with diffuse neutrophilic infiltration (E) and the left atrial myocardium with lymphocytic infiltration (F); h/e - hematoxylin-eosin staining. Explanation in the text.
Discussion
The above-described case meets all the criteria of IE, but is quite difficult for understanding. First of all, the combination of IE with severe SARS-CoV-2-positive myocarditis, confirmed by EMB six months after COVID-19, is unusual. Our findings suggest coronavirus persistence in the myocardium as one of the leading mechanisms of chronic post-COVID myocarditis development [2]. In the present case myocarditis
also included an autoimmune component - the titers of anti-heart antibodies were significantly elevated and the morphological picture of inflammation persisted even after virus elimination from the myocardium (intraoperative biopsy six months later).
Due to negative hemoculture the etiology of IE remained unclear - we can assume the involvement of special, rare pathogens on the background of immunosuppression caused by persistent coronavirus. The role of direct coronavirus lesion of valve endocardium cannot be ruled out (although neutrophil infiltrate content and abscess formation make us think about bacterial flora), as well as non-bacterial thromboendocarditis prior to infection. Cases of the latter have been described in COVID-19 [7]; the prothrombogenic status of patients with coronavirus infection predisposes to its development.
We can assume the binary nature of myocarditis as well - immune as part of IE and autoimmune within coronavirus. Myocarditis as an immunocomplex complication of IE is well known, but it is typically much milder than in the presented case. There are only single cases of COVID-associated endocarditis described in the literature, in which one can think of simultaneous myocardial damage (although the authors do not draw such a conclusion). Troponin T elevation, acute systolic dysfunction and sudden death in a patient with IE indicate possible development of myocarditis, but autopsy data are not presented [5]. In another case 3 months after COVID-19 there were significant elevation of troponin level, LV contractility and perfusion impairment, but EMB showed no definite criteria of myocarditis, just endocardial thickening and endocardium neutrophil infiltration were detected [8].
References
- Escher F, Pietsch H, Aleshcheva G, Bock T, Baumeier C, et al. Detection of viral SARS-CoV-2 genomes and histopathological changes in endomyocardial biopsies. ESC Heart Fail. 2020; 7: 2440-2447.
- Blagova OV, Kogan EA, Lutokhina Yu A, Kukleva AD, Ainetdinova DH, et al. Subacute and chronic post-covid myoendocarditis: clinical presentation, role of coronavirus persistence and autoimmune mechanisms. Kardiologiia. 2021; 61: 11-27.
- Pietsch H, Escher F, Aleshcheva G, Baumeier C, Morawietz L, et al. Proof of SARS-CoV-2 genomes in endomyocardial biopsy with latency after acute infection. Int J Infect Dis. 2021; 102: 70-72.
- Havers-Borgersen E, Fosbøl EL, Butt JH, Petersen JK, Dalsgaard A, et al. Incidence of infective endocarditis during the coronavirus disease 2019 pandemic: A nationwide study. Int J Cardiol Heart Vasc. 2020; 31: 100675.
- Toth E, Dancy L, Amin-Youssef G, Papachristidis A, Dworakowski R. Collateral implications of the COVID-19 pandemic: belated presentation of infective endocarditis in a young patient. Eur Heart J. 2020; 41: 4365.
- Alizadehasl A, Salehi P, Roudbari S, Peighambari MM. Infectious endocarditis of the prosthetic mitral valve after COVID-19 infection. Eur Heart J. 2020; 41: 4604.
- Balata D, Mellergård J, Ekqvist D, Baranowski J, Garcia IA, et al. Non-Bacterial Thrombotic Endocarditis: A Presentation of COVID-19. Eur J Case Rep Intern Med. 2020; 7: 001811.
- Aikawa T, Ogino J, Kudo T, Kashiwagi Y. Late-onset endocarditis after coronavirus disease 2019 infection. Eur Heart J. 2021; 42: 3108.
