
Open Access, Volume 9
Tigecycline induced liver toxicity in a renal transplant recipient with hepatic histology imitating sepsis
Sofia Fragkioudaki1; Maria Darema1; Mina Psichogiou2; Kostas Palamaris3; John Boletis1; Stratigoula Sakellariou3
1Department of Nephrology and Renal Transplantation, Laiko General Hospital, National and Kapodistrian University of Athens, Athens, Greece.
2First Department of Medicine, Laiko General Hospital, National and Kapodistrian University of Athens, Athens, Greece.
3First Department of Pathology, Laiko General Hospital, National and Kapodistrian University of Athens, Athens, Greece.
Stratigoula Sakellariou
First Department of Pathology, Laiko General Hospital, National and Kapodistrian University of Athens, Mikras Asias 75, 11527, Athens, Greece.
Tel: +30-2132061059;
Email: sakellarioustrat@yahoo.gr
Received : February 15, 2023,
Accepted : March 30, 2023
Published : April 05, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: Tigecycline has an expanded broad-spectrum antibacterial activity including multi-drug resistant pathogens. A case of a renal transplant recipient with tigecycline- induced acute liver injury is presented.
Case presentation: A 47-year-old female patient with end-stage renal disease underwent a deceased donor kidney transplantation. Due to donor infection, she received perioperative and postoperative antibiotic prophylaxis, including tigecycline, for 10 days. On day 12 of hospitalization the recipient presented conjugated hyperbilirubinemia and elevated liver enzymes. Liver biopsy revealed severe steatosis, large and small droplet macrovesicular as well as microvesicular and marked hepatocellular, canalicular and cholangiolar cholestasis, the latter raising suspicion of sepsis. Exclusion of bacterial infection rendered drugs as possible causative agent. The findings of patients’ workup complemented by literature data implicated tigecycline as causative agent. Following drug withdrawal, the patient gradually improved and was discharged with near normal hepatic biochemistry.
Conclusion: This case demonstrates that, although tigecycline is known to be well tolerated, high doses can cause severe liver impairment, rendering close patient monitoring mandatory. Awareness of distinct histology combining steatotic and cholestatic pattern with features imitating sepsis can prevent a possible diagnostic pitfall.
Keywords: Tigecycline; Renal transplantation; Low fibrinogen levels; Cholangiolar cholestasis; Drug induced liver injury; Tigecycline induced coagulopathy.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Sakellariou S (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Fragkioudaki S, Darema M, Psichogiou M, Palamaris K, Boletis J, Sakellariou S. Tigecycline induced liver toxicity in a renal transplant recipient with hepatic histology imitating sepsis. Open J Clin Med Case Rep. 2023; 2005.
Introduction
Among advanced antibacterial agents, tigecycline -a glycycline antibiotic- confers activity against a broad range of highly drug resistant bacteria [1]. Complicated intra-abdominal and respiratory infections, as well as complicated skin infections, represent the main indications for tigecycline use [2]. The combination of tigecycline with other broad spectrum antibiotic regimens, such as carbapenems and polymyxins constitutes a common clinical practice against bloodstream infections caused by multi- drug resistant gram negative bacteria [3]. Bacteremia represents one of the leading causes of morbidity and mortality following solid organ transplantation, including renal transplantation [4].
The continuing shortage of organs available for transplant has led to an expansion of the deceased donor pool, including donors with gram-negative bacteremia. However, there is a low risk of infection transmission, especially if the recipient is offered appropriate antimicrobial treatment after transplantation.
Furthermore, the problem of antibiotic resistance is relevant in intensive care units, suggesting that in case of complicated infections with carbapenem-resistant enterobacteriaceae the treatment with a broad-spectrum bacteriostatic agent such as tigecycline, is warranted. Tigecycline is often administered in immunosuppressed patients and is in general well tolerated [7]. Non-specific gastrointestinal disturbances are among the most common adverse events. However, serious complications such as deterioration of hepatic and pancreatic function [5-7] or life threatening coagulation disorders [8-10] have occasionally been reported. In the context of renal transplantation, an additional source of drug intolerance originates from the interaction between tigecycline and calcineurin inhibitors, the main immunosuppressive agents applied to graft recipients. It has been reported that concurrent administration of the two regimens incites increased serum levels of these immunosuppressants [11-13].
Herein, a case of a renal transplant recipient who developed acute liver injury showing distinct histological features after tigecycline administration, is reported.
Case Presentation
A 47-year-old female patient with end-stage renal disease secondary to familiar focal segmental glomerulosclerosis -dialysis dependent for nine years- underwent renal transplantation, receiving graft from a deceased donor on December 2021. Her past medical history included hypertension, cholecystectomy and tonsillectomy. No drug-induced allergic reactions were mentioned. According to pre-transplant evaluation, no significant pathological findings were determined.
The donor was a 38 years old man who developed central nervous system infection derived from extensively drug-resistant Acinetobacter baumannii and fungi associated urinary tract infection. The persistence of fever and the high levels of inflammatory markers, despite the advanced antibiotic donor treatment, imposed the administration of perioperative and postoperative preventive antimicrobial recipient medication.
Cold ischemia time was 18 hours. The patient received induction therapy with anti-intrerleukin-2 receptor antibody (basiliximab), followed by triple immunosuppressive maintenance regimen consisting of tacrolimus, mycophenolate mofetil and methylprednisolone. After specialist consultation, she was treated with meropenem, colistin, daptomycin with dose adjustment according to estimated creatinine clearance, tigecycline for 10 days, as well as micafungin for 14 days. Tigecycline was administered intravenously with initial loading dose 200mg, followed by maintenance dose of 100 mg every 12 hours thereafter.
The patient experienced delayed graft function, requiring eight dialysis sessions after operation. Progressive increase in urine output appeared from the sixth postoperative day, while gradual serum creatinine decline became obvious from the twentieth postoperative day.
Within twelve days of transplantation, laboratory analysis revealed progressive decline of hepatic function, with direct hyperbilirubinemia and elevated liver enzymes. Laboratory tests were negative for viral infections. On clinical examination, the patient was hemodynamically stable and exhibited painless jaundice, without fever or other pathological symptoms and signs. Bilirubin levels were 12.8mg/dl, serum aspartate and alanine transaminase were 207 U/L and 170 U/L respectively, alkaline phosphatase was 700U/L and Gamma-glutamyl transferase reached serum levels of 950 U/L. Abnormal hematological parameters, including anemia requiring red blood cells transfusion (hemoglobulin levels 7 g/dl) and thrombocytopenia (platelet count: 50 K/μl) were also detected. Of note, fibrinogen was decreased to levels below 100 mg/dl (on the tenth postoperative day), while tacrolimus trough levels presented remarkable increase to 25 ng/ml. Finally, inflammatory markers were within normal range.
Extensive imaging evaluation was performed. Abdominal computed tomography scanning revealed neither focal liver lesions, nor acute vascular event. Echocardiographic study, including ventricular systolic and diastolic function and valve hemodynamic assessment, was also normal. Due to the progressive pattern of abnormal liver function and the risk of developing acute liver failure, a diagnostic liver biopsy was considered necessary.
Histologically, hepatic parenchyma showed severe steatosis, large and small droplet macrovesicular as well as microvesicular, characterized by numerous tiny fat droplets within hepatocyte cytoplasm, resembling alcoholic foamy degeneration. There was also marked hepatocellular and canalicular cholestasis predominantly in zones 3 and 2, as well as prominent ductular reaction periportally (zone 1) accompanied by the presence of bile concretions in the lumen of dilated cholangioles. This feature referred as cholangiolar cholestasis or cholangitis lenta, although not entirely specific, it raises high suspicion of sepsis [14]. On the other hand, the pattern of steatosis implied a toxic liver injury similar to the one observed after parenteral administration of tetracycline. Since no sign of infection was identified after thorough evaluation, drug toxicity was implicated for liver dysfunction and antimicrobial agents were discontinued. After withdrawal, patient’s laboratory status gradually improved. She was discharged with near normal hepatic biochemistry, creatinine concentration approximately 2 mg/dl, no coagulation disorders, and better regulation of tacrolimus levels.
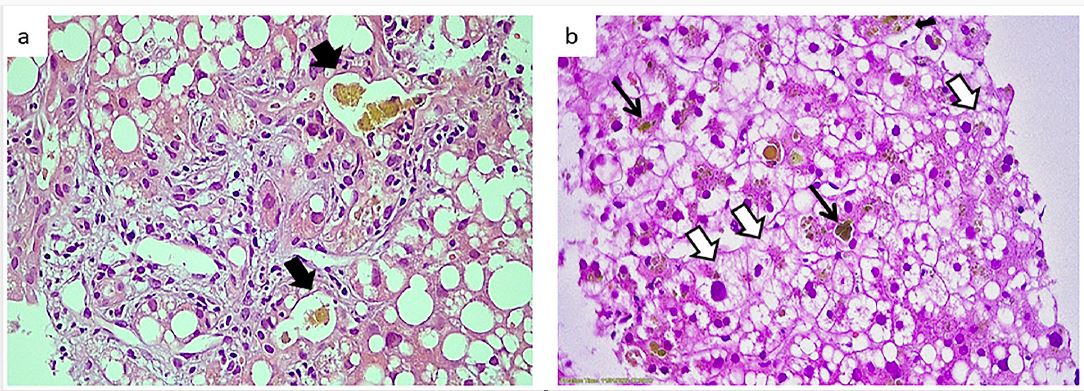
Figure 1: (a). Cholangiolar cholestasis: periportal dilated ductules, their lumina containing bile concretions (black arrowheads). (b). Severe steatosis, large and small droplet macrovesicular as well as microvesicular (white arrowheads), accompanied by hepatocellular and canalicular cholestasis (black arrows) (a,b H/E X400).
Discussion and Conclusion
In the current report, a rare case of renal transplant recipient with tigecycline induced liver dysfunction and intrahepatic cholestasis is presented. Tigecycline administration is usually associated with mild, non-specific complications, mainly disorders of the gastrointestinal tract, although more serious adverse events, including coagulopathy, may also occur [15].
The patient exhibited low fibrinogen levels and decreased platelet count, without bleeding event. Administration of tigecycline, especially in high doses, has been impeached for reversible hypofibrinogenemia, usually accompanied by thrombocytopenia, in several case reports [16-18]. The mechanism of tigecycline derived coagulopathy remains unclear. A potential pathogenetic link could be based on the production of several cytokines mediated by tigecycline. Hepatic dysfunction may also have an impact on fibrinogen biosynthesis [19,20]. Renal function, fibrinogen levels at the time of drug initiation, tigecycline dose and treatment duration are important predictors of tigecycline induced hypofibrinogenemia [21,22]. Regarding tigecycline dosage, although high maintenance doses are associated with better antimicrobial outcomes compared with more conservative ones, they are associated with more pronounced reduction of fibrinogen levels [9,23]. Randomized studies which have investigated the impact of tigecycline on the fibrinogen concentration compared to other antibiotic regimens, provided further indications of ticegycline induced hypofibrinogenemia [24], though without major bleeding events [25]. The high doses given to our patient support a concentration dependent side effect.
Tigecycline–related hepatic impairment manifested by elevated liver enzymes and hyperbilirubinemia is considered a relatively uncommon complication [5]. Previous reports acknowledge liver dysfunction as side effect mainly related to treatment duration [26,27]. Moreover, according to literature data, few renal transplant patients suffered from acute pancreatitis associated with use of tigecycline, and recovered after agent discontinuation [6,7]. It remains unresolved whether immunosuppressed patients are more susceptible to this adverse reaction.
It has to be stated that our patient received maintenance immunosuppressive scheme including tacrolimus, the concentration of which increased to toxic levels, following tigecycline administration. The interaction between tigecycline and calcineurin inhibitors leading to heightened levels is well defined and cautious regulation is required [11-13]. The co-occurrence of increased tacrolimus and decreased fibrinogen levels implicates tigecycline as causative agent among several other antimicrobial drugs given to our patient. In addition, one may suggest a potentiation of the cholestatic toxic effect by the combination of tigecycline and tacrolimus in high concentrations.
The present case is also remarkable for its histological manifestation. Foremost, cholangiolar cholestasis is an alarming finding requiring careful clinical assessment in order to exclude the possibility of underlying sepsis. Thus, only by exclusion, other causes, in particular drug-related toxicity, should be taken into consideration. According to the European Association for the Study of the Liver Clinical Practice Guidelines this particular type of cholestasis in a patient with drug induced liver injury (DILI) is an adverse histological prognosticator, pointing to more severe cases possibly requiring liver transplantation [28]. Secondly, the observed microvesicular type of steatosis is a well-established, drug-related pattern of hepatic injury, characteristic for tetracyclines. In contrast to the severity of our case, tigecycline is thought to be relatively safe causing mild, transient transaminasemia and very rarely jaundice of clinical significance. Liang et al [29] reported the case of a 41-year-old woman who developed cholestasis while receiving tigecycline. Liver function improved after cessation of the drug, supporting the diagnosis of cholestatic liver injury induced by tigecycline. A biopsy was not performed, so histology remains unknown. Roussel Uclaf Causality Assessment Method (RUCAM) score was 6, indicating probable DILI. In our case Rucam score was 7, also indicative of probable DILI [30].
Considering normalization of liver enzymes after drug withdrawal, we may support that tigecycline, especially in high doses and probably in combination with high levels of calcineurin inhibitors, may cause severe toxic liver injury, rendering close patient monitoring mandatory. Awareness of distinct histology combining steatotic and cholestatic pattern with features imitating sepsis can prevent a possible diagnostic pitfall.
Statements and Declarations
Funding: The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Competing interests: The authors have no relevant financial or non-financial interests to disclose.
Author contributions: The first draft of the manuscript was written by Sofia Fragkioudaki and Stratigoula Sakellariou and all authors revised it critically for important intellectual content. All authors read and approved the final manuscript.
Acknowledgments: None.
References
- Yaghoubi S, Zekiy AO, Krutova M, Gholami M, Kouhsari E, et al. Tigecycline antibacterial activity, clinical effectiveness, and mechanisms and epidemiology of resistance: narrative review. Eur J Clin Microbiol Infect Dis. 2021; 1-20.
- Doan TL, Fung HB, Mehta D, Riska PF. Tigecycline: a glycylcycline antimicrobial agent. Clin Ther. 2006; 28: 1079-1106.
- Candel FJ, Calvo N, Head J, Sánchez A, Matesanz M, et al. A combination of tigecycline, colistin, and meropenem against multidrug-resistant Acinetobacter baumannii bacteremia in a renal transplant recipient: pharmacodynamic and microbiological aspects. Rev Esp Quimioter. 2010; 23: 103-108.
- Tsikala-Vafea M, Basoulis D, Pavlopoulou I, Darema M, Deliolanis J, et al. Bloodstream infections by gram-negative bacteria in kidney transplant patients: Incidence, risk factors, and outcome. Transpl Infect Dis. 2020; 22: e13442.
- Kadoyama K, Sakaeda T, Tamon A, Okuno Y. Adverse event profile of tigecycline: data mining of the public version of the U.S. Food and Drug Administration adverse event reporting system. Biol Pharm Bull. 2012; 35: 967-970.
- Lin J, Wang R, Chen J. Tigecycline-induced acute pancreatitis in a renal transplant patient: a case report and literature review. BMC Infect Dis. 2018; 18: 201.
- Yazirli B, Kara E, Inkaya AC, Maden S, Ozberk U, et al. A case report of tigecycline induced acute pancreatitis in a renal transplant patient and review of the literature: Should we avoid tigecycline in patients on calcineurin inhibitors? Transpl Infect Dis. 2021; 23: e13593.
- Sabanis N, Paschou E, Gavriilaki E, Kalaitzoglou A, Vasileiou S. Hypofibrinogenemia induced by tigecycline: a potentially life-threatening coagulation disorder. Infect Dis (Lond). 2015; 47: 743-746.
- Fan Q, Huang W, Weng Y, Xie X, Shi Z. Hypofibrinogenemia induced by high-dose tigecycline-case report and review of literature. Medicine (Baltimore). 2020; 99: e22638.
- Pieringer H, Schmekal B, Biesenbach G, Pohanka E. Severe coagulation disorder with hypofibrinogenemia associated with the use of tigecycline. Ann Hematol. 2010; 89: 1063-1064.
- Stumpf AN, Schmidt C, Hiddemann W, Gerbitz A. High serum concentrations of cyclosporin related to administration of tigecycline. Eur J Clin Pharmacol. 2009; 65: 101-103.
- Pavan M, Chaudhari AP, Ranganth R. Altered bioavailability of tacrolimus following intravenous administration of tigecycline. Am J Kidney Dis. 2011; 57: 354.
- Chow KM, Pang WF, Chan GCK, Leung CB, Szeto CC, et al. Beware of drug interaction between tigecycline and tacrolimus. Nephrology (Carlton). 2020; 25: 99-100.
- Booth AL, Merwat SN, Merwat SK, Stevenson HL. Cholangitis Lenta: What Hepatologists Need to Know. Clin Liver Dis (Hoboken). 2020; 15: 236-238.
- Cui N, Cai H, Li Z, Lu Y, Wang G, Lu A. Tigecycline-induced coagulopathy: a literature review. Int J Clin Pharm. 2019; 41: 1408-1413.
- Wu X, Zhao P, Dong L, Zhang X. A case report of patient with severe acute cholangitis with tigecycline treatment causing coagulopathy and hypofibrinogenemia. Medicine (Baltimore). 2017; 96: e9124.
- Campany-Herrero D, Larrosa-Garcia M, Lalueza-Broto P, Rivera-Sánchez L, Espinosa-Pereiro J, et al. Tigecycline-associated hypofibrinogenemia in a real-world setting. Int J Clin Pharm. 2020; 42: 1184-1189.
- Giryes S, Azzam ZS, Ismael-Badarneh R, Krivoy N, Berger G. Severe Coagulation Disorder and Thrombocytopenia Associated with Tigecycline - Case Report and Review of Literature. Curr Drug Saf. 2017; 12: 7-9.
- Yılmaz Duran F, Yıldırım H, Şen EM. A Lesser Known Side Effect of Tigecycline: Hypofibrinogenemia. Turk J Haematol. 2018; 35: 83-84.
- Wu PC, Wu CC. Tigecycline-associated hypofibrinogenemia: A case report and review of the literature. IDCases. 2018; 11: 56-57.
- Zhang Q, Wang J, Liu H, Ma W, Zhou S, et al. Risk factors for tigecycline-induced hypofibrinogenaemia. J Clin Pharm Ther. 2020; 45: 1434-1441.
- Hu J, Xiao YH, Zheng Y, Lai YX, Fang XL, et al. Clinical characteristics and risk factors of tigecycline-associated hypofibrinogenaemia in critically ill patients. Eur J Clin Pharmacol. 2020; 76: 913-922.
- Treml B, Rajsic S, Hell T, Fries D, Bachler M. Progression of Fibrinogen Decrease during High Dose Tigecycline Therapy in Critically Ill Patients: A Retrospective Analysis. J Clin Med. 2021; 10.
- Hakeam HA, Al Duhailib Z, Salahuddin N, Amin T. Impact of tigecycline versus imipenem-cilastatin on fibrinogen levels following cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC): a randomized-controlled study. J Chemother. 2018; 30: 224-232.
- Huang YT, Yu CI, Chen PY, Wang CC, Wu CC. Comparison of Bleeding Risk Between Colistin-Tigecycline and Colistin-Carbapenem Treatment Regimens: A Retrospective Cohort Study. Infect Drug Resist. 2021; 14: 4949-4955.
- Gao HH, Yao ZL, Li Y, Huang S, Liu J, Jing Y. Safety and Effectiveness of High Dose Tigecycline for Treating Patients with Acute Leukemia after Ineffctiveness of Carbapenems Chemotherapy Combinating with Febrile Neutropenia: Retrospective study. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2018; 26: 684-690.
- Chen Z, Shi X. Adverse events of high-dose tigecycline in the treatment of ventilator-associated pneumonia due to multidrug-resistant pathogens. Medicine (Baltimore). 2018; 97: e12467.
- EASL Clinical Practice Guidelines: Drug-induced liver injury. J Hepatol. 2019; 70: 1222-1261.
- Liang J ZK, Zhu L, Liu Y. Tigecycline Induced Cholestatic Liver Injury: A Case Report. J Infect Dis Epidemiol. 2018; 4: 060.
- Danan G, Teschke R. RUCAM in Drug and Herb Induced Liver Injury: The Update. Int J Mol Sci. 2015; 17.
