
Open Access, Volume 9
Giant osteochondroma of upper fibula with nerve irritation
Khaled Kamoun1*; Ahmed Mdaoukhi1; Wajdi Arfa1; Wajih Oueslati1; Leila Abid2; Mourad Jenzri1
1Pediatric Orthopedic Department, Kassab Institute, El Manar University, Tunisia.
2Anatomopathology Department, Kassab Institute, El Manar University, Tunisia.
Khaled Kamoun
Pediatric Orthopedic Department, Kassab Institute, El Manar University, Tunisia.
Email: kawther_ba@yahoo.fr
Received : February 13, 2023,
Accepted : March 10, 2023
Published : March 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Osteochondroma or Exestosis are the most common benign bone tumor mostly arises from long bone metaphysis. Sessile or pedenculated, they are always covered by cartilaginous cap and occur more often in children. Osteochondroma can be part of hereditary disease with multiple location or isolated. Tumor size and location are the most important factors predicting complications such as mechanical compression. This rare situation can occur when ostechondroma arise near nerve trajectory.
We report a rare case of a 14 years old boy followed for neck fibular osteochondroma since 3 years and recently complaining from nerve irritation in Common Peroneal Nerve (CPN) territory. Radiograph showed a pedenculated osteochondroma arising from the fibula neck confirmed by CT scan and MRI extending medially and posterior with intimate contact with CPN. A tumor has been resected and common peroneal nerve dissected and released. The child has recovered from these sensitive neurological disorders with no local recurrence at follow up. This case could make us reflect about early surgical management of such tumor, even benign, when it develops near anatomic vascular nerve structures.
Keywords: Osteochondroma; Fibula; Peroneal nerve; Child; Exestosis.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Kamoun K (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Kamoun K, Mdaoukhi A, Arfa W, Oueslati W, Abid L, et al. Giant osteochondroma of upper fibula with nerve irritation. Open J Clin Med Case Rep. 2023; 1995.
Introduction
Osteochondroma or Exestosis are the most common benign bone tumor that mostly arises from long bones metaphysic. They could be sessile or pedenculated and always covered by cartilaginous cap. They occurs more often in children and stops growing in adulthood; they could be isolated or being part of hereditary disease with multiple location. Tumor size and location are the most important factors predicting complications such as mechanical compression. This rare situation can occur when ostechondroma arise near nerve trajectory. This risk of nerve irritation can be majored by it superficial situation.
Case Presentation
Setting
We report a case of fourteen-years-old boy seen in outpatient department for swelling and left knee pain, evolving since 3 years and recently complaining from sensation of electric discharge in his left leg lateral side. There was no fever no weight losses but a mild limping when walking. A four-centimeter hard mass regarding the left upper fibular was identified, painful at the palpation with no inflammatory signs. dynamic knee maneuver did not reveal laxity. The neurological exam found hypoesthesia in the territory of the common peroneal nerve (CPN) without motor deficiency.
Knee x-ray showed a pedenculated tumor developing from the fibula neck (Figure 1a, 1b) increased in size compared with previous radiographs (Figure 2a, 2b). CT confirm findings with this “cauliflower like” exestosis developing from fibula neck with cartilage cap and with no invasion of the cortical bone (Figure 3).
Magnetic resonance imaging confirms the benign aspect of the tumor with no invasion of the soft tissue , the CPN was in intimate contact with the tumor (Figure 4).
A surgical resection was conducted by posterior lateral approach. CPN was initially identified anterior to the osteochondroma released and then tumor was totally removed (Figure 5).
Histopathologic exam confirmed the diagnosis of osteochondroma with bony trabeculae,enchondral ossification and hyaline cartilage cap (Figure 6). The child has recovered from these sensitive neurological disorders with no local recurrence at follow up (Figure 7).

Figure 1: (a,b) Knee x-ray showing fibular neck pedencu-Knee x-ray showing fibular neck pedenculated tumor with high-density and clear boundaries.
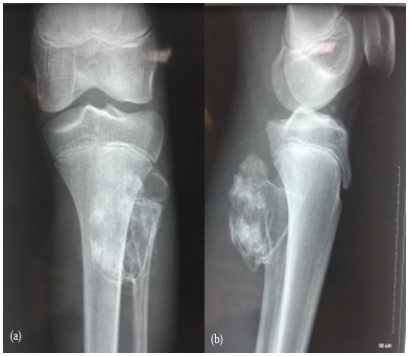
Figure 2: (a,b) increasing in osteochodroma size extending postero-medially.
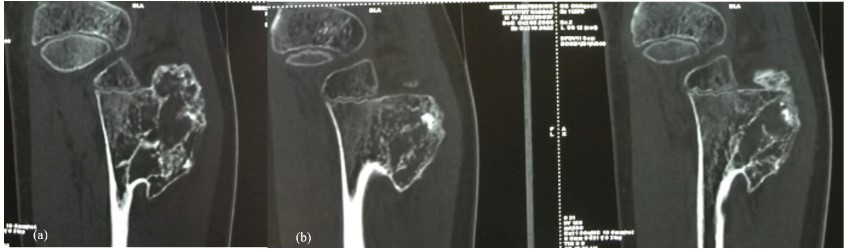
Figure 3: (a,b): CT Scan showing voluminous “cauliflower like” pedenculated tumor arising from fibula neck with no
sign of malignancy.
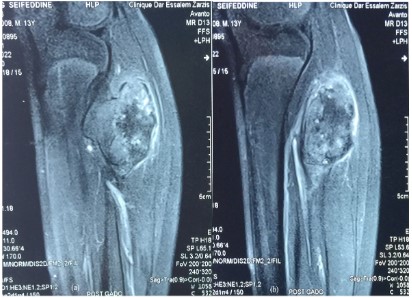
Figure 4: (a,b): Coronal T1weigted showing osteochondroma with large cartilage cap and contact with the CPN
with no sign of sufferance.
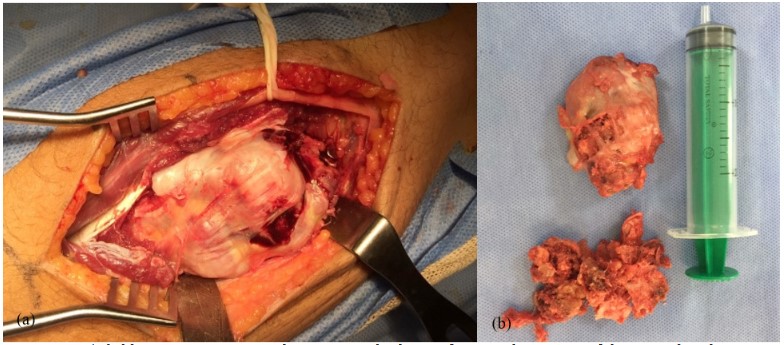
Figure 5: (a,b): Preoperative view dissection and release of CPN and exposing of the osteochondroma.
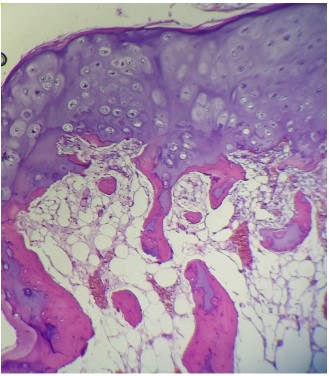
Figure 6: H&E x 200 the lesion shows hyaline cartilage cap underlying an area
of enchondral ossification followed by mature bony trabeculaeconttaining
normal bone marrow.
Discussion
CPN has a superficial situation. Indeed, it is located behind the fibular neck and is covered only by cutaneous and subcutaneous tissus. Thus it’s damaged easier [1]. Etiologies of CFN palsy are dominated by traumatic lesion (40%), tumors of the head or the neck of fibula remain rare (6%) [1,2].
Osteochondroma is the most frequent bone tumor arising growing from the cartilaginous plate of long bones [3], it affected both males and females and stop growing in adulthood [4]. This tumor affects the metaphysis around the knee (distal femur, proximal tibia and fibula) in 40% of cases [3]. Usually, osteochondroma is asyptomatic. It can be revealed by X-ray in fortuitous way [4]. Osteochondromas can cause pain, deformity or compression of noble organs [4].
Neurovascular complications include palsy, sensitive defeciency and pseudoaneurysm and they are the most serious complications of benign tumors [5,6]. The compression of CFN is the most common complication of proximal fibula exostoses. Cherad et all reported a same case with CFN palsy caused by fibular neck osteochondrome, a total resection had done and the patient was recovered in three months after surgery [1]. Murat et all reported a case of 13 years old male patient presenting deep fibular nerve palsy caused by fibular exestosis, the outcome after surgical resection were excellent [8]. In addition to these cases, our patient was satisfied after the surgery and the electric signs disappeared. Surgical excision of the osteochondroma and the CFN nerve release had a good outcomes in all reported cases [8-11].
Conclusion
Despite its benign character, osteochondroma can induce neurological complications by mechanical compression as in our case with CFN irritation. Prognosis depends on early surgical management to prevent size progression. Osteochondroma surgical resection should be performed when compromising nerve integrity even when asymptomatic.
Conflict of interest statement: None.
References
- Cherrad T. Peroneal Nerve Palsy due to Bulky Osteochondroma from the Fibular Head: A Rare Case and Literature Review. Case Reports in Orthopedics. 2020; 5.
- Arabi H, Bakzaza O, El Fikri A, Elktaibi A, Saidi H, et al. Compression of the peroneal nerve by a neurofibroma originating from collaterals of the peroneal nerve: a case report. Journal of Medical Case Reports. 2016; 10: 1.
- Unni KK. Cartilagenous lesions of bone. Journal of Orthopaedic Science. 2001; 6: 457-472.
- Jie Sun, Wang ZP, Zhang Q, Zhou ZY, Liu F, et al. Giant osteochondroma of ilium: a case report and literature review. International Journal of Clinical and Experimental Pathology. 2021; 14: 538-544.
- Antonio D, Lorenzo A, Federico S, Simone C, Rodolfo C. Hereditary Multiple Exostoses: Current Insights. Orthopedic Research and Reviews. 2019; 11: 199-211.
- Kemal G, Ahmet T. Solitary osteochondroma of ischial ramus causing sciatic nerve compression. Joint Diseases and Related Surgery. 2013; 24: 49-52.
- Murat D, Korhan Ö, Bulent K. Deep peroneal nerve palsy due to osteochondroma arising fromfibular head and proximal lateral tibia. International Journal of Surgery Case Reports. 2017; 31: 200-202.
- Kemal G, Halil A. Osteochondromas originating from unusual locations complicating orthopedic discipline: case series. Joint Diseases and Related Surgery. 2015; 26: 100-109.
- Takashi K, Masayoshi M. Peroneal Nerve Palsy Caused by Proximal Fibular Solitary Osteochondroma: Case Report and Literature Review. Case Reports in Orthopedics. 2022; 3.
- Arda C, Feridun Y. A rare cause of ‘drop foot’ in the pediatric age group: Proximal fibularosteochondroma a report of 5 cases. International Journal of Surgery Case Report. 2014; 5: 1068-1071.
