
Open Access, Volume 9
Bilateral coronary ostial stenosis and aortic regurgitation due to syphilitic aortitis
Xingli Fan; Chengliang Cai; Yangfeng Tang; Lin Han*
Department of Cardiovascular Surgery, The First Affiliated Hospital of Naval Medical University, Shanghai, 200433, China.
Lin Han
Department of Cardiovascular Surgery, The First Affiliated Hospital of Naval Medical University, Shanghai,
200433, China.
Email: sh_hanlin@163.com
Received : January 10, 2023,
Accepted : February 08, 2023
Published : February 10, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Syphilitic aortitis classically involves aortic root, resulting in coronary ostial stenosis (COS) and aortic valve insufficiency.
Case report: We present a 63-year-old male with aortic valve regurgitation and recurrent COS due to syphilitic aortitis after percutaneous coronary intervention (PCI), the patient accepted Aortic Valve Replacement (AVR) and Coronary Artery Bypass Graft (CABG). Antibiotic therapy (benzathine penicillin G) is a supplement for cardiovascular syphilis.
Conclusion: CABG is a possible and effective interventions to treat syphilitic COS and long-term follow-up is mandatory.
Keywords: Syphilitic aortitis; Coronary ostial stenosis; Percutaneous coronary intervention; Coronary artery bypass graft.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Han L (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Fan X, Cai C, Tang Y, Han L. Bilateral coronary ostial stenosis and aortic regurgitation due to syphilitic aortitis. Open J Clin Med Case Rep. 2023; 1823.
Introduction
Cardiovascular syphilis usually occurs 10-20 years after the initial syphilis infection [1]. Syphilitic aortitis classically involves aortic root, resulting in Coronary Ostial Stenosis (COS) and aortic valve insufficiency [2]. COS is the second most common complication of syphilitic aortitis [3], and is caused by aortic wall thickening, and is characterized with normal coronary distal vessels [1]. We present a case of bilateral COS and aortic regurgitation due to syphilitic aortitis.
Case Report
A 63-year-old male was admitted to the emergency department due to acute severe chest pain, accompanied by excessive perspiration. He was a long-term smoker and suffered from hypertension for two years, without previous cardiovascular diseases. The cardiopulmonary examination was normal. Laboratory test revealed troponin I was 1.303 ug/L, Treponema pallidum immunoglobin G (TP-IgG) was positive, and the value of syphilis toluidine red without serum test (TRUST) was 1: 128. Electrocardiogram (ECG) showed sinus tachycardia with ST depression in leads DII, DIII, aVF, V3, V4, V5 and V6 and complete Right Bundle Branch Block (RBBB) (Figure 1C). The echocardiography showed no apparent abnormality.
The patient was rapidly transferred to the cath lab. Coronary angiography showed severe bilateral COS (Figure 1A-B). Primary Percutaneous Coronary Intervention (PCI) was performed used a Xience Alpine 3.5 × 15 mm balloon stent (Abbott Vascular, Santa Clara, CA USA) implanted in right coronary ostial, and a Xience Alpine 4.0 × 12 mm balloon stent (Abbott Vascular, Santa Clara, CA, USA) implanted in left main stem. The final angiography showed good stent expansion and patency of blood flow. After the procedure, the chest pain was disappeared. Three days later, the patient was discharged and took aspirin, ticagrelor, statin and beta-blocker for postoperative cardiovascular treatment. A recommended dose of benzathine penicillin for syphilitic was supplemented (3 doses of 2.4 million units i/m each at 1-week intervals).
Five months later, the patients suffered from intermittent chest pain again and admitted to the cardiovascular department. Laboratory test revealed troponin I was 0.882 ug/L, BNP was 1172 pg/ml, and the value of syphilis TRUST was still 1: 128. Electrocardiogram (ECG) showed sinus rhythm with ST depression in leads V3, V4, V5 and V6 compatible with complete RBBB (Figure 1D). Echocardiography revealed an increase of the left ventricular end-diastolic diameter (LVEDD, 62 mm), severe aortic valve regurgitation and normal left ventricular function (LVEF, 59%). Aorta computed tomography confirmed severe stenosis in both right and left main coronary ostia and thickened wall at ascending aorta (Figure 2A-C). Coronary angiography showed severe bilateral COS (Figure 3A-B).
We performed Aortic Valve Replacement (AVR) used 21 mm biological valve (St. Jude Medical, St. Paul, Minnesota, USA), aortic root enlargement used bovine pericardium (Bairen Medical Technology, Beijing, China) and Coronary Artery Bypass Graft (CABG). The left Internal Mammary Artery (ITA) was diverted to the left anterior descending artery, the Saphenous Vein Graft (SVG) was diverted to the left marginal branch, and to the posterior descending artery. The surgical approach was performed through a median-thoracotomy. After harvesting of the left ITA, a cardiac arrest burst that the harvesting of the right ITA was force suspension. We established Cardiopulmonary Bypass (CPB) immediately followed by cannulation of the femoral artery, superior and inferior vena cava, clamping of the ascending aorta. Persistent retrograde cardiac perfusion was performed via cannulation of the coronary sinus due to the COS. The patient presented with thickened wall at the aortic root and the ascending aorta, epidermoid hyperplasia around bilateral coronary ostial, and fibrosis at the aortic valve edge. Because of the thickened wall at ascending aorta, we used bovine pericardium to enlarge aorta root, and anastomosed the saphenous vein to the bovine pericardium.
The patient was transmitted to the intensive care unit for postoperative cardiovascular treatment. Mechanical ventilation was ceased three days later, and IABP was removed ten days later. Pathological biopsy showed multifocal infiltration of lymphocytes and plasma cells in the media, and coagulative necrosis in the local area (Figure 3C). Laboratory test showed syphilis TRUST descended to 1: 16. Two months after surgery, the patient visited a cardiologist with no complaint. During the follow-up visit, echocardiography revealed reduced LVEDD (46 mm), normal left ventricular function (LVEF 54%), and normal aortic biological valve function, coronary artery computed tomography showed patency of blood flow of graft vessels (Figure 3D).
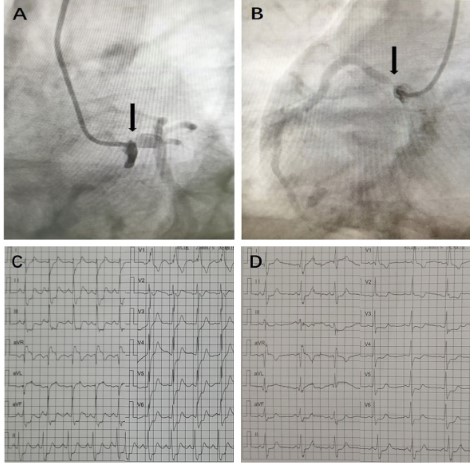
Figure 1: (A) Coronary angiography showed left coronary ostial stenosis. (B) Coronary angiography showed right coronary
ostial stenosis. (C) Electrocardiogram showed sinus tachycardia with ST depression in leads DII, DIII, aVF, V3, V4, V5 and V6
and complete right bundle branch block. (D) Electrocardiogram showed sinus rhythm with ST depression in leads V3, V4, V5
and V6 compatible with complete right bundle branch block.
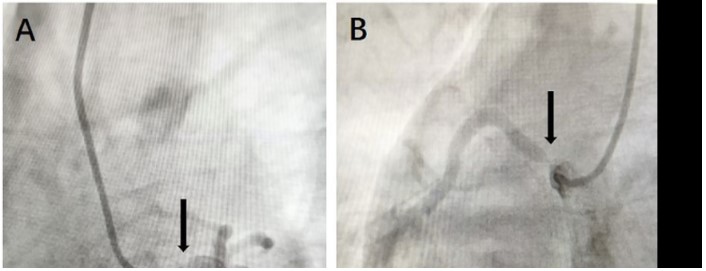
Figure 2: Aorta computed tomography showed (A) Thickened wall at ascending aorta. (B) Severe stenosis in left main coronary ostia. (C) Severe stenosis in right main coronary ostia.
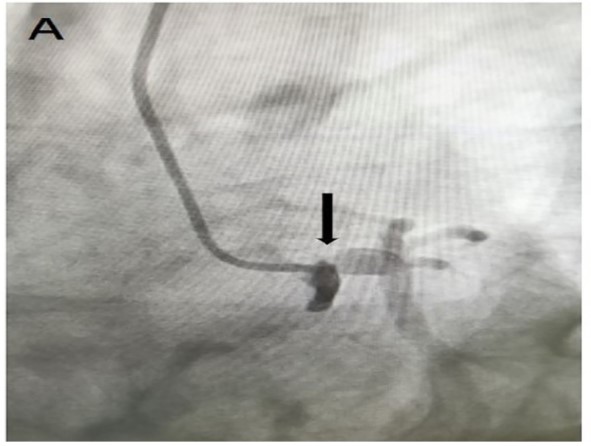
Figure 3: (A) Coronary angiography showed left coronary ostial stenosis. (B) Coronary angiography showed right coronary
ostial stenosis. (C) Hematoxylin-eosin stain at 50x magnification showed multifocal infiltration of lymphocytes and plasma
cells in the media, and coagulative necrosis in the local area. (D) Coronary artery computed tomography showed patency of
blood flow of graft vessels.
Discussion
COS and aortic regurgitation occur in patients with syphilitic aortitis. Antibiotic therapy should be recommended according to the guideline for cardiovascular syphilis [4]. Although syphilitic aortitis has declined due to the efficacy of antibiotic therapy [2], the prevalence of COS with aortic regurgitation has been reported to be 14% in patients with syphilitic aortitis [5]. Matsuyama et al. reported a case with high positive titers 2 months after antibiotic therapy for 2 months [1]. Our case developed recurrent bilateral COS after antibiotic therapy and PCI,that suggested continuous infection of the aortic wall.
The options of different revascularization strategies for COS is disquisitive. Marcelo et al. reported a case with Acute Myocardial Infarction (AMI) due to syphilitic COS treated by PCI, that suggested PCI is a possible and effective intervention to treat syphilitic COS [6]. PCI is recommended within first 12 h from onset of symptoms [7], CABG is preferred if there are stable angina or delayed admission from presentation [2,8]. There are no comparative studies of PCI versus CABG in treating syphilitic COS [9], and potential anastomotic stenosis or restenosis in-stent restenosis caused by continuous infection of the ascending aorta may exist [2]. In the present case, we anastomose SVG to the bovine pericardium to avoid this situation, long-term follow is mandatory as a result of potential anastomotic stenosis.
Bilateral ITA, instead of Saphenous Vein Graft (SVG), should be preferred as a result of potential graft failure caused by syphilitic aortitis. Rūta et al. described a 37-year-old male with AMI due to syphilitic COS, which treated by CABG with the left ITA diverted into the proximal part of the left anterior descending artery, and the right ITA diverted to the proximal part of the right coronary artery [2]. In the present case, we abandoned the right ITA due to the cardiac arrest, which was attributed to coronary hypoperfusion caused by COS and low blood pressure during anesthesia. Hence, low blood pressure should be avoided before CPB especially in patients with COS.
Long-term follow-up is mandatory as a result of syphilitic aortitis, the occurrence of prosthetic valve dehiscence, or graft failure caused by continuous infection of the aortic wall. Further comparative studies are required to compare PCI with CABG in syphilitic COS.
Conclusions
Although syphilitic aortitis has declined due to the efficacy of antibiotic therapy, syphilitic COS with aortic regurgitation are still present. CABG is a possible and effective interventions to treat syphilitic COS, and further comparative studies are required to compare PCI with CABG in syphilitic COS. Long-term follow-up is mandatory as a result of syphilitic aortitis, the occurrence of prosthetic valve dehiscence, or graft failure caused by continuous infection of the aortic wall.
Declarations
Conflict of interests: The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding: The authors received no financial support for the research and/or authorship of this article.
References
- Matsuyama K, Kuinose M, Iida Y, Iwahashi T, Sato K, et al. Bilateral coronary ostial stenosis and aortic regurgitation in a patient with cardiovascular syphilis. J Cardiol Cases. 2012; 6: e173-e175.
- Žvirblytė R, Ereminienė E, Montvilaitė A, Jankauskas A, Ivanauskas V. Syphilitic coronary artery ostial stenosis resulting in acute myocardial infarction. Medicina (Kaunas). 2017; 53: 211-216.
- Jackman JD, Radolf JD. Cardiovascular syphilis. Am J Med. 1989; 87: 425-433.
- Workowski KA, Berman SM. Sexually transmitted diseases treatment guidelines, 2006. MMWR Recomm Rep. 2006; 55: 1-94.
- Heggtveit HA. SYPHILITIC AORTITIS. A CLINICOPATHOLOGIC AUTOPSY STUDY OF 100 CASES, 1950 TO 1960. Circulation. 1964; 29: 346-355.
- Nakazone MA, Machado MN, Barbosa RB, Santos MA, Maia LN. Syphilitic coronary artery ostial stenosis resulting in acute myocardial infarction treated by percutaneous coronary intervention. Case Rep Med. 2010; 2010: 830583.
- Windecker S, Kolh P, Alfonso F, Collet JP, Cremer , et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014; 35: 2541-2619.
- Aizawa H, Hasegawa A, Arai M, Naganuma F, Hatori M, et al. Bilateral coronary ostial stenosis and aortic regurgitation due to syphilitic aortitis. Intern Med. 1998; 37: 56-59.
- Predescu LM, Zarma L, Platon P, Postu M, Bucsa A, et al. ST Segment Elevation Myocardial Infarction Due to Severe Ostial Left Main Stem Stenosis in a Patient with Syphilitic Aortitis. Rom J Intern Med. 2016; 54: 74-79.
