
Open Access, Volume 9
Mechanical mitral prosthetic thrombosis in a 52-year-old marfan woman associated with COVID-19 infection
Vasiliki Vartela*; Konstantinos Ritsatos; Georgios Stavridis; Georgios Karatasakis
Cardiology Department and 3rd Cardiac Surgery Department, Onassis Cardiac Surgery Center, 356, Syggrou Av., Athens, Greece.
Vasiliki Vartela
Cardiology Department and 3rd Cardiac Surgery Department, Onassis Cardiac Surgery Center, 356, Syggrou Av., Athens, Greece.
Email: vasvartela@yahoo.gr
Received : January 03, 2023
Accepted : February 06, 2023
Published : February 10, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Patients with coronavirus disease 2019 (COVID-19) may present a hypercoagulable state, which can lead to thrombotic manifestations. We present a case of mechanical mitral valve thrombosis and a large thrombus in the left atrium after COVID-19 infection in a 52-year-old Marfan woman.
Keywords: Mechanical mitral valve; Thrombosis; Covid-19.
Abbreviations: VATS: Video-Assisted Thoracoscopic Surgery; NSAIDs: Non-Steroidal Anti-Inflammatory Medications; MRI: Magnetic Resonance Imaging; CT: Computed Tomography; FSA: Frozen Section Analysis; AP: Anteroposterior; RERAML: Retroperitoneal Extrarenal Angiomyolipomas; SMA: Smooth Muscle Antibody; SMM: Smoldering Multiple Myeloma; MDM2: Mouse Double Minute 2
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Vartela V (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Vartela V, Ritsatos K, Stavridis G, Karatasakis G. Mechanical Mitral Prosthetic Thrombosis in a 52-Year-Old Marfan Woman associated with COVID-19 Infection. Open J Clin Med Case Rep. 2023; 1977.
Introduction
Infection with Covid-19 may cause a hypercoagulable state and people who have mechanical valve prosthesis may have a higher risk of valve thrombosis [1,2].
Case Report
We present the case of a 52-year-old lady with Marfan syndrome, permanent pacemaker, Mitral Valve (MV) repair at the age of 34 years old and mitral valve replacement with a mechanical bileaflet prosthesis at the age of 40 yo who was referred to our Emergency Department (ED) for exertional dyspnea. Approximately 2 months prior due to exhibition fatigue and shortness of breath she was advised to undergo molecular COVID-19 test which was positive. She gradually deteriorated and was admitted in a COVID dedicated hospital. She was treated for coronavirus disease 2019 (COVID-19)-related pneumonia and was discharged ten days later. A month later she was referred to the ED of our hospital because of exertional dyspnea and palpitations. On the admission the ECG showed atrial fibrillation associated with a ventricular rate of 90-110 beats per minute. There were no signs of pulmonary edema in lung x ray. A Transthoracic Echocardiogram (TTE) revealed signs of prosthetic MV stenosis and elevated Right Ventricular Systolic Pressure (RVSP). The left ventricle was slightly dilated with moderate function. One of the discus of the mitral prosthesis was immobilized in closed position resulting obstruction to flow. The mean pressure gradient by Doppler echocardiography was 15 mmHg (Figure 1A) and the RVSP 70 mmHg. The International Normalized Ratio (INR) on admission was 2.6 and no problem with the INR therapeutic range was reported by the patient in the last months. The patient was initially treated with unfractionated heparin infusion. Follow-up TTE on second, fourth and sixth day later did not show signs of improvement.
A cardiac Computer Tomography (CT) examination revealed signs of discus thrombosis, a large thrombus on the anterior surface of the left atrium near the Left Atrial Appendage (LAA) and no coronary artery disease. The patient underwent a cardiac surgery in which thrombus from the LAA and the discus was removed and the LAA was sutured (Figure 2). After surgery the mean pressure gradient of the mitral prosthesis measured by Doppler echocardiography was decreased (4.6 mmHg) and there was no dysfunction of the discus (Figure 1B). Six days later the patient was discharged home.
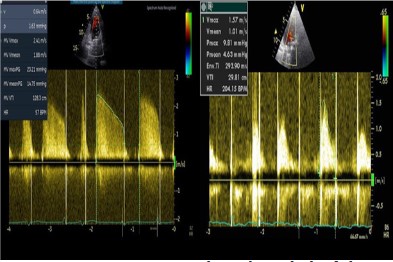
Figure 1: Mean pressure gradient (Doppler) of the mechanical mitral valve before (A) and after (B) surgical removal of thrombus on the valve discus.

Figure 2: Surgical preparation of thrombus removed from
the mechanical mitral discus and the left atrium.
Discussion
The annual incidence rate of prosthetic valve thrombosis varies from 0.1% to 5.7%, and it is more common in mechanical prosthesis in mitral and tricuspid positions. Pulmonary embolism, venous and arterial thrombosis have been reported in hospitalized patients with COVID-19 [1]. COVID-19 infection causes cytokine storm, hypoxic injury, hypercoagulability, increased platelet activity, and endothelial damage [2]. The coagulation changes associated with COVID-19 suggest the presence of a hypercoagulable state that might increase the risk of thromboembolic complications. Furthermore, immobilization and vascular damage are other factors that can increase the risk of thrombosis [3]. The acute arterial vasculopathy related to COVID-19 is diverse and associated with a high risk of death. As it is reported in a recent study of 531 COVID-19 adult inpatients, 30 (5.6%) experienced arterial thrombotic events, which happened at a median of 11 (5-20) days after the first symptoms of infection; occurred at patients in high-risk according to traditional cardiovascular risk factors. An atypical pattern, such as thrombosis of the aorta, upper limb, or renal arteries or cerebral microvasculopathy was noted and was associated with an in-hospital mortality rate of 40% [4]. A case of a patient with COVID-19, who developed a pulmonary embolism and thrombosis of a biological mitral valve prosthesis, producing valve obstruction and stenosis was presented a few months ago [5]. Patients with COVID-19 may present hypercoagulability, causing the occurrence of pulmonary thromboembolism and in some cases also thrombosis of heart valve prosthesis, as was the case for this patient 2 weeks after he was discharged from the hospital for COVID-19 pneumonia. With these findings, they supported the recommendation of a prolonged anticoagulation strategy at full therapeutic doses after discharge of selected COVID-19 patients, particularly those with valve prosthesis, including biological ones. Another case of acute thrombosis of mechanical aortic prosthesis in a 65-year-old patient with COVID-19 infection and recent acute myocardial infarction was described recently [6]. Despite full subcutaneous anticoagulation, the patient presented thrombosis of the valve prosthesis, which was probably related to the hypercoagulability represented by COVID-19 infection, in conjunction with the hemodynamic changes caused by recent acute myocardial infarction, which generates a stunned myocardium with consequent reduction in dilution and washout of the periprosthetic coagulation activating factors, contributed to the thrombosis of the mechanism [6,7]. Our patient was the first one reported after COVID-19 infection with mechanical mitral valve thrombosis and presentation of a large thrombus in the left atrium, which may played a significant role in valve thrombosis, even though she was under optimal anticoagulation therapy.
Despite limited evidence the use of anticoagulation as primary prevention in COVID-19 patients has been proposed and some scientific societies have already made some recommendations about the anticoagulation management. They also include the administration of anticoagulant therapy up to 45 days after hospital discharge if there are thrombotic risk factors (eg, reduced mobility, active cancer, elevated d-dimer > 2 times the upper limit of normal) and low risk of bleeding [8].
Patients with COVID-19 may present a hypercoagulable state. This stage can induce thromboembolic events. A prolonged anticoagulation therapy at therapeutic doses in hospitalized and after discharge of selected COVID-19 patients, could be discussed especially in those with valve prosthesis. The role of COVID-19 in thromboembolic events and the clarification of the duration and the dosage of anticoagulation in these specific subgroups remains to be discussed.
References
- Connors JM, Levy JH. COVID-19 and its implications for thrombosis and anticoagulation. Blood. 2020; 135: 2033-2040.
- Chauhan AJ, Wiffen LJ, Brown TP. COVID-19: a collision of complement, coagulation and inflammatory pathways. J Thromb Haemost. 2020.
- Levi M, Thachil J, Iba T, Levy JH. Coagulation abnormalities and thrombosis in patients with COVID-19. Lancet Haematol. 2020; 7: e438-e440.
- Morgane Fournier. Arterial Thrombotic Events in Adult Inpatients With COVID-19 Mayo Clin Proc. 2021; 96: 295-303.
- Guillem Llopis Gisbert, Verónica Vidal Urrutia, Miguel A. Moruno Benita. Bioprosthetic Valve Thrombosis and Obstruction Secondary to COVID-19. Can J Cardiol. 2020.
- Marcos H.F. Jacob, Tatiana C.A.T. Leal, Paulo Rogério Soares Mechanical Aortic Prosthetic Thrombosis in a 65-Year-Old Woman with SARS-CoV-2 Infection. Arq Bras Cardiol. 2018; 115.
- Dangas GD, Weitz JI, Giustino G, Makkar R, Mehran R. Prosthetic Heart Valve Thrombosis. J Am Coll Cardiol. 2016; 68: 2670- 2689.
- Bikdeli B, Madhavan MV, Jimenez D. COVID-19 and thrombotic or thromboembolic disease: implications for prevention, antithrombotic therapy, and follow-up: JACC state-of-the-art review. J Am Coll Cardiol. 2020; 75: 2950-2973.
