
Open Access, Volume 8
Cupid’s aortic disease
Ana Pericao; Stam Kapetanakis; Andrew D’Silva*
Department of Cardiology, Guy’s & St Thomas’ NHS Foundation Trust, London, UK.
Andrew D’Silva
Department of Cardiology, Guy’s & St Thomas’ NHS Foundation Trust, London, UK.
Email: adsilva@nhs.net
Received : September 05, 2022,
Accepted : September 24, 2022
Published : September 30, 2022,
Archived : www.jclinmedcasereports.com
Abstract
Late syphilis presenting with cardiovascular complications has been rare since the Antibiotic Era. We present an atypical presentation of myocardial infarction with cardiovascular risk factors, complicated by a post-coronary angiogram stroke, likely related to catheter manipulation in the presence of ascending aortic inflammation with large thrombus burden due to syphilitic aortitis.
Keywords: Myocardial infarction; Dilated left ventricle; Aortic root thrombus; Large-vessel vasculitis; Tertiary; Syphilis.
Abbreviations EF: Ejection fraction; MRI: Magnetic resonance imaging; CT: Computed tomography; FDG-PET: F-Fluorodeoxyglucose positron emission tomography; TTE: Transthoracic echocardiogram; LAD: Left anterior descending; CRP: C -reactive protein; ESR: Erythrocyte sedimentation rate.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © D’Silva A (2022)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Pericao A, Kapetanakis S, D’Silva A. Cupid’s aortic disease. Open J Clin Med Case Rep. 2022; 1912.
Introduction/Background
Cardiovascular syphilitic lesions in tertiary syphilis can manifest as aortitis, formation of an aneurysm, aortic root dilatation, aortic regurgitation, and coronary ostial stenosis [1,2]. Aortitis is the most common cardiovascular complication of untreated late syphilis [3]. We outline a case of an unusual presentation of myocardial infarction.
Case Presentation
We report a case of a 62-year-old black man with no known past medical history who presented with acute dyspnoea and pulmonary oedema. He suffered an embolic myocardial infarction, systemic emboli including a stroke, and was found to have extensive inflammation in the ascending aorta associated with a large aortic root thrombus.
His coronary angiogram showed an embolic occlusion of the distal left descending artery and transthoracic echocardiogram showed a severely impaired and dilated left ventricle, EF 15-20%, mild aortic regurgitation and a large mobile thrombus in the aortic root.
Cardiac MRI demonstrated a predominantly ischaemic pattern of enhancement consistent with Left Anterior Descending (LAD) artery infarction. The aortic appearances were further characterised by MRI, CT and FDG-PET, visualising the thrombus burden and demonstrating extensive ascending aortic inflammation, raising the possibility of large-vessel vasculitis. Treponema pallidum antibody was positive in high titre, indicating a likely cardiovascular manifestation of tertiary syphilis. Treatment included penicillin and warfarin anticoagulation.
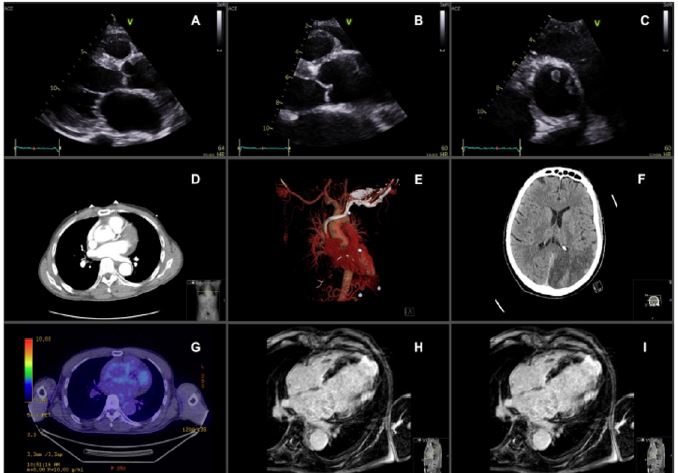
Figure 1: Multimodality imaging panel of syphilitic aortitis, complicated by an aortic thrombus with embolisation causing stroke and myocardial infarction in the LAD territory. A - C - Parasternal views on TTE, A - parasternal long axis view, B - aortic root in long axis, C- aortic root in short axis; D-E – CT coronary angiogram demonstrating aortic root thrombus; F - CT brain demonstrating posterior circulation cerebral infarction; G - PET CT demonstrating aortic wall inflammation; and H-I cardiac MRI demonstrating transmural infarction in a left anterior descending artery territory.
Discussion/Conclusion
This represents a presentation of a large aortic thrombus secondary to aortitis and cardiovascular syphilis with multiple embolic complications.
His transthoracic echocardiogram (A-C) shows a severely dilated left ventricle and mobile echogenic mass circling the aortic root, consistent with a thrombus. The aortic root was also mildly dilated with thickened walls and mild aortic regurgitation. The aortic appearances were further characterised by CT (D) and FDG-PET (G), visualising the thrombus burden and demonstrating extensive ascending aortic inflammation respectively, raising the possibility of large-vessel vasculitis. Cardiac MRI (H-I) demonstrated transmural infarction in the distal LAD territory.
He was initially treated with intravenous methylprednisolone and cyclophosphamide on initial suspicion of vasculitis with a CRP of 75 mg/L and ESR of 56 mm/hr. However, his Treponema pallidum antibody took a few days to process and was positive in high titre, indicating a likely cardiovascular manifestation of tertiary syphilis. Therefore, immune suppression was stopped and intravenous benzyl penicillin 2.4 g six-hourly was given. He was also anti coagulated with warfarin.
At five months follow-up, there was resolution of the aortic root thrombus with anticoagulation and improvement of left ventricular systolic function to an ejection fraction of 46% on optimal heart failure therapy. His neurological deficits had also significantly improved.
This case is an unusual presentation of a myocardial infarction in a 62-year old man who is an ex-smoker, complicated by a post-coronary angiogram stroke, likely related to catheter manipulation in the presence of ascending aortic inflammation with large thrombus burden due to syphilitic aortitis. Whilst syphilis is recognised as a rare cause of aortitis and should be tested for when the disease is suspected or there is a past medical history of syphilis infection(4), this case highlights that the test should be performed as soon as possible, given the typical delays in results reporting and the implications in management, as demonstrated in his case by altering strategy from immunosuppressing corticosteroid therapy to antibiotic treatment. This case of cardiovascular syphilis was diagnosed in the absence of clinical suspicion of syphilis infection in a patient presenting with ST-elevation myocardial infarction.
References
- Žvirblytė R, Ereminienė E, Montvilaitė A, Jankauskas A, Ivanauskas V. Syphilitic coronary artery ostial stenosis resulting in acute myocardial infarction. Medicina. 2017; 53: 211-216.
- Barbosa-Barros R, Pérez-Riera AR, Koivula K, de Carvalho Santos J, de Abreu LC, Nikus K. Acute coronary syndrome of very unusual etiology. Ann Noninvasive Electrocardiol. 2018; 23: e12531.
- Fernandes B, Santos A, Carvalho L. Syphilitic Aortitis Diagnosis in Clinical Setting. Rev Port Cir Cardiotorac Vasc. 2017; 24: 166.
- Pugh D, Grayson P, Basu N, Dhaun N. Aortitis: recent advances, current concepts and future possibilities. Heart. 2021; 107: 1620-1629.
