
Open Access, Volume 8
Peripartum cardiomyopathy with severe mitral regurgitation:
A novel application of an intra-aortic balloon pump as
a bridge to recovery
Elisa Padron1*; Anne R Waldrop2; Kathleen Minor2; Abha Khandelwal3; Jess Ansari4; Deidre Lyell5; Katherine Bianco5
1Stanford University School of Medicine, USA.
2Department of Obstetrics and Gynecology, Stanford University School of Medicine, USA.
3Department of Cardiovascular Medicine, Stanford University School of Medicine, USA.
4Department of Anesthesiology, Stanford University School of Medicine, USA.
5Department of Maternal Fetal Medicine, Stanford University School of Medicine, USA.
Elisa Padron
Stanford University School of Medicine, USA.
Email: ep23874@stanford.edu
Received : August 11, 2022,
Accepted : September 15, 2022
Published : September 20, 2022,
Archived : www.jclinmedcasereports.com
Abstract
There is evidence that an Intra-Aortic Balloon Pump (IABP) may be used in hemodynamically unstable patients to reduce afterload, improve coronary perfusion and prevent myocardial damage. Current mainstays of treatment in Peripartum Cardiomyopathy (PPCM) include optimization of preload and inotropic support through medical management. The data for use of IABPs in PPCM is limited to case reports in situations that are refractory to medical management. We present a case report about 29-year-old primigravid woman with dichromatic/diamniotic twin pregnancy at 32 weeks and 2 days who presented with threatened preterm labor. Her medical history was notable for cutaneous lupus erythematosus managed without recent flares, on hydroxychloroquine. Preterm labor was arrested at 0.5 cm during first day of admission. Antenatal steroids were given ongoing symptomatic contractions. Additionally, upon presentation, she was found to have progressive dyspnea. A chest x-ray was performed, with results concerning for pulmonary edema, and mild cardiomegaly. Due to her ongoing and worsening dyspnea, an echocardiogram was performed which showed moderate to severe eccentric mitral regurgitation, with a right atrial pressure of 20 mmHg. During her admission, serial echocardiograms were performed, with subsequent findings of her Ejection Fraction (EF) dropping precipitously from 62% to 50.4% over 24 hours. There was no evidence of mitral valve prolapse and there was a preserved Left Atrial (LA) size and biventricular size and function. Given her history of cutaneous lupus, rheumatology was consulted during her inpatient stay, and felt the presentation was not consistent with a lupus flare or Libman-Sacks endocarditis given the absence of lupus anticoagulant antibodies
A multidisciplinary conference determined that due to severe Mitral Regurgitation (MR) and concern for worsening peripartum cardiomyopathy, the plans should be made to proceed with delivery. In the setting of anticipated hemodynamics during delivery, the cardiology team recommended she receive an Intra-Aortic Balloon Counter Pulsation (IABP) prior to undergoing cesarean section. Moreover, it was determined that Caesarean section was indicated due to acutely worsening cardiac function.
Two days after the multidisciplinary meeting, the IABP procedure was performed prior to the start of the Cesarean section. Both procedures were uncomplicated. The IABP was removed the day of surgery. The patient recovered well. During the postpartum period, she was managed with losartan, Lasix, metoprolol. She was discharged on metoprolol 50 mg daily and had a recovery of cardiac function by 2 months postpartum. Based on our case, the use of an IABP is a viable option as a bridge to recovery for patients at risk of PPCM and have anticipated hemodynamic demands during delivery.
Keywords: Peripartum cardiomyopathy; Cardiomyopathy; Intra-aortic balloon pump; Twin gestation; Mitral regurgitation; IABP
Abbreviation EF: Ejection Fraction; ECMO: Extracorporeal Membrane Oxygenation; IABP: Intra-Aortic Balloon Counter Pulsation; LA: Left Atrial; LV: Left Ventricular; LVAD: Left Ventricular Assist Device; MR: Mitral Regurgitation; PPCM: Peripartum Cardiomyopathy
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Padron E (2022)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Padron E, Waldrop AR, Minor K, Khandelwal A, Ansari J, Lyell D, Bianco K. Peripartum cardiomyopathy with severe mitral regurgitation: A novel application of an intra-aortic balloon pump as a bridge to recovery. Open J Clin Med Case Rep. 2022; 1907.
Introduction
Peripartum Cardiomyopathy (PPCM) affects 1 in 1000 pregnancies worldwide and accounts for 25% to 30% of maternal deaths [1]. PPCM is classified as heart failure occurring in the last month of pregnancy or postpartum with a left ventricular systolic dysfunction with an Left Ventricular (LV) ejection fraction of less than 45% [2]. The current theory of the physiology of PPCM is known as the two hit hypothesis, where patients who have one or more cardiac genetic mutations [3]. Prolactin secretion by the maternal pituitary and antiangiogenic factor secretion by the placenta cause myocardial damage and is compounded by the secretion of a vascular endothelial growth factor inhibitory molecule, which is found in multifetal pregnancy [3]. Risk factors for this condition in patients often include age greater than 30, black race, a hypertensive disorder of pregnancy such as preeclampsia, multiple gestations, and history of PPCM [2,7- 11]. The incidence of PPCM is increasing in the US, which may be due to increasing prevalence of these risk factors during pregnancy [4]. Conversely, improved diagnostic modalities may also be causing the incidence rate to rise. Complications of PPCM can lead to arrhythmias and thromboembolisms.
The cardiac output and circulating blood volume is greatly increased during a twin pregnancy, increasing up to 15% more than a singleton pregnancy [5]. During labor, delivery, and after delivery, the maximum cardiac output occurs with increase 60% to 80% higher than previously seen in pregnancy, which puts patients with PPCM at risk [5]. Current mainstay treatments for PPCM are assisted ventilation, optimization of preload support, and inotropes and vasopressors [6]. When medical therapy does not improve hemodynamic status, mechanical circulatory support can be used. Circulatory support devices include Intra-Aortic Balloon Counter Pulsation (IABP), Extracorporeal Membrane Oxygenation (ECMO), and Left Ventricular Assist Device (LVAD). These devices can be utilized while the patient is recovering from heart failure, in transition to a durable device, or in severe circumstances, in need of transplant [6].
There are limited publications on Intra-Aortic Balloon Pump (IABP) being used prophylactically in patients with PPCM and anticipated hemodynamic instability during a planned cesarean delivery [12-13]. However, there is evidence to show that use of prophylactic IABP in cardiac patients can serve to increase left ventricular ejection fraction [14]. We report a case of a patient with PPCM successfully undergoing a Cesarean section with preoperative IABP placement and post operative IABP removal.
Case Report
A 29-year-old primigravid woman with history of systemic lupus erythematosus, managed with hydroxychloroquine, and no previous cardiac history was admitted for concern of preterm labor with dichorionic/diamniotic twin pregnancy at 32 weeks and 2 days. Preterm labor was arrested at 0.5 cm during first day of admission. Antenatal steroids were given ongoing symptomatic contractions. She started to have progressive dyspnea and had decreased oxygen saturation of 94%. Upon work up, there was no evidence of an infectious etiology. A chest x-ray showed moderate to severe pulmonary edema and cardiomegaly (Figure 1). Electrocardiograph showed sinus tachycardia. On presentation, her echocardiogram showed moderate to severe eccentric mitral regurgitation, a right atrial pressure of 20 mmHg and an EF of 62% (Figure 2). There was no evidence of mitral valve prolapse. LA size and biventricular size were preserved. Rheumatology was consulted during her inpatient stay, and felt that this was unlikely a lupus flare or Libman-Sacks endocarditis and instead was diagnosed with worsening peripartum cardiomyopathy. Repeat echocardiogram was performed 24 hours after initial echocardiogram and showed severe mitral regurgitation and worsening ejection fraction of 50.4% (Figure 2).
A multidisciplinary team was employed, including cardiology, anesthesia, maternal fetal medicine, intensive care, and her primary OB team, and the decision was made for her transfer to the Critical Care Unit. Due to PPCM with severe Mitral Regurgitation (MR), and anticipated hemodynamic shifts during delivery, the decision was made to place a prophylactic Intra-Aortic Balloon Pump (IABP) prior to undergoing cesarean section to optimize afterload reduction and to improve forward flow. The IABP procedure as well as the Cesarean section were uncomplicated.
A combined spinal/epidural for regional anesthesia was placed by anesthesiology and caesarean section was performed at 32 weeks and 5 days with delivery of both twins. For the presenting twin, Apgar scores at 1 minute and 5 minutes were 4 and 7 and birth weight was 1.76 kg. For second twin, Apgar scores at 1 minute and 5 minutes were 8 and 7 and birth weight was 1.76 kg. Following ongoing stability in the Post Anesthesia Care Unit and recovery, the IABP was removed the day of surgery and she was monitored in the Critical Care Unit for 24 hours. Cardiology team recommended patient be transitioned to postpartum unit. A postpartum echocardiogram following IABP removal showed improving mitral regurgitation and cardiomyopathy with improved ejection fraction of 56% (Figure 2). In the postpartum period, she was managed with Losartan, Lasix, and Metoprolol and experienced relatively uncomplicated postpartum course. She was discharged on Metoprolol 50 mg daily and her cardiac function returned to normal by 2 months postpartum (Figure 2).

Figure 1: A chest x-ray during third day of admission showing bilateral pleural effusions
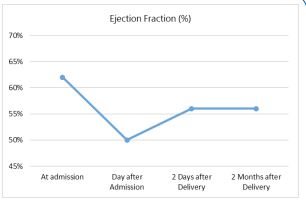
Figure 2: Ejection fraction of patient with mitral regurgitation before and after IABP prophylactically
used during caesarean section.
Discussion
An IABP was prophylactically used before caesarean delivery of twins for a patient that presented with progressive dyspnea, peripartum cardiomyopathy, and acute severe mitral regurgitation. Historically, patients with peripartum cardiomyopathy require medical therapies such as inotropes and vasopressors, arrhythmia management, anticoagulation therapy, investigational therapies, and in severe circumstances, mechanical supports. Mechanical support options include the IABP which has been shown to improve the hemodynamics of patients with acute mitral regurgitation and decreased left ventricular ejection fraction by increasing the mean arterial pressure resulting in improved ventricular function. A study by Gevaert et. al described 6 cases in which short term, IABP, mechanical supports were utilized for patients with severe PPCM and acute heart failure including 2 patients during caesarean delivery and 4 patients in the postpartum period [15]. Two patients had recovered left ventricular function and 4 patients were transitioned to left ventricular assistant devices and eventually received heart transplants [15].
Patients with peripartum cardiomyopathy may not respond to medical treatment, and the prophylactic placement of an IABP can serve as a bridge to overcome anticipated hemodynamic shifts during delivery for patients with PPCM. We present this case to demonstrate a successful prophylactic IABP insertion, which in this case, avoided worsening left ventricular function and needing a LVAD or ECMO during delivery or postpartum. More studies are needed to show risks and benefits of prophylactic IABP placement prior to caesarean deliveries, in effort to lessen maternal cardiac morbidity and mortality during pregnancy and postpartum. We also recommend the importance of delivery in a tertiary hospital where a multidisciplinary team can evaluate and create an individualized delivery plan for patients.
Acknowledgements: We want to thank the patient for allowing us to share their story. We would also like to thank Dr. Justin Thompson for managing the care of the patient and the Maternal Heart Team at Stanford School of Medicine.
References
- Farrell A, Kuller J, Goldstein S, Dotters-Katz S. Peripartum Cardiomyopathy. Obstetrical & Gynecological Survey. 2021; 76: 485- 492.
- Arany Z, Elkayam U. Peripartum Cardiomyopathy. Circulation. 2016; 133: 1397-1409.
- Cunningham F, Byrne J, Nelson D. Peripartum Cardiomyopathy. Obstetrics & Gynecology. 2019; 133: 167-179.
- Kolte D, Khera S, Aronow WS, Palaniswamy C, Mujib M, et al. Temporal trends in incidence and outcomes of peripartum cardiomyopathy in the United States: a nationwide population-based study. J Am Heart Assoc. 2014; 3: e001056.
- Sanghavi M, Rutherford J. Cardiovascular Physiology of Pregnancy. Circulation. 2014; 130: 1003-1008.
- Zagelbaum N, Bhinder J, Gupta C, Frishman W, Aronow W. Peripartum Cardiomyopathy Incidence, Risk Factors, Diagnostic Criteria, Pathophysiology, and Treatment Options. Cardiology in Review. 2020; 28: 148-155.
- Hafkesbring E, Hull E. «Toxic» postpartal heart disease. New Orleans Med Surg J. 1937; 89:550.
- Demakis JG, Rahimtoola SH, Sutton GC, Meadows WR, Szanto PB, et al. Natural course of peripartum cardiomyopathy. Circulation 1971; 44:1053.
- Elkayam U, Akhter MW, Singh H, Khan S, Bitar F, et al. Pregnancy-associated cardiomyopathy: clinical characteristics and a comparison between early and late presentation. Circulation. 2005; 111:2050.
- Veille JC. Peripartum cardiomyopathies: a review. Am J Obstet Gynecol. 1984; 148:805.
- Bello N, Rendon IS, Arany Z. The relationship between pre-eclampsia and peripartum cardiomyopathy: a systematic review and meta-analysis. J Am Coll Cardiol. 2013; 62:1715.
- Guasch NBE, Puertas L, Alsina E, Lopez T, Gilsanz F. Acute early postpartum cardiac failure associated with dilated cardiomyopathy: successful treatment with intra-aortic balloon counter-pulsation and levosimendan. Ann Fr Anesth Reanim. 2010; 29: 807-810.
- Samalavicius RSL, Radaviciute PI, Norkiene I, Urbonas K, Misiuriene I, et al. Prophylactic Use of an Intra-Aortic Balloon Pump in a High-Risk Patient with Peripartum Cardiomyopathy Requiring Cesarean Delivery. International Journal of Obstetric Anesthesia. 2018; 33: 67-71.
- Lorusso R, Gelsomino S, Carella R, Livi U, Mariscalco G, et al. Impact of prophylactic intra-aortic balloon counter-pulsation on postoperative outcome in high-risk cardiac surgery patients: a multicentre, propensity-score analysis. Eur J Cardiothorac Surg. 2010; 38: 585-591.
- Gevaert, Sofie, Yves Van Belleghem, Stefaan Bouchez, Ingrid Herck, Filip De Somer, et al. Acute and Critically Ill Peripartum Cardiomyopathy and ‘bridge to’ Therapeutic Options: A Single Center Experience with Intra-Aortic Balloon Pump, Extra Corporeal Membrane Oxygenation and Continuous-Flow Left Ventricular Assist Devices. Critical Care. 2011; 15: 1-7.
